
Abstract
Background:
The HOT (Healthy Outcome for Teens) Project is an innovative online educational intervention for middle school children for prevention of diabetes and obesity by balancing food intake with physical activity. The objective was to improve knowledge, outcome expectations, self-efficacy, and self-reported food intake and skills and to compare a passive online learning (POL) control group with an active online learning (AOL) treatment group by implementing a social cognitive theory (SCT)-grounded online intervention.
Subjects and Methods:
In total, 214 participants were recruited from three middle schools. Full data were secured for 181 students. Six valid, reliable questionnaires were administered online, pre/post, to both the AOL and POL groups to assess knowledge gain, self-reported intake, and meal planning skills, as well as change in SCT constructs.
Results:
Subjects in the AOL group improved significantly for all five categories of planning a meal questionnaire (P=0.001) and also for outcome expectations for exercise (P=0.001). At postintervention, no significant differences were found for composite scores of exercise self-efficacy, weight efficacy lifestyle, and rapid eating assessment plan questionnaires between AOL versus POL (by Mann–Whitney test).
Conclusions:
We conclude that teens participating in the AOL version of the HOT Project intervention acquired skills for planning a meal and improved outcome expectations for exercise.
Introduction
I
Health interventions for youth have traditionally targeted parents and schools, as youth spend most of their time either at school or at home. Schools are a popular setting for health promotion and weight control interventions because they provide a safe and supportive environment with policies and practices that support healthy behaviors. 5 Several meta-analyses of the efficacy of obesity prevention programs indicate that the effects of the current obesity preventive approaches are fairly small. 5 Moreover, research literature suggests that more obesity prevention and treatment interventions are needed specifically for the adolescent population, as this population is underserved, and these health habits tend to follow them into adulthood. 1,4
To enhance the efficacy toward healthy decision-making, new strategies are warranted that include the application of electronic media. Interactive media make the program delivery standardized and dramatically reduce the burden on schools. 6 A study conducted by Casazza and Ciccazo 7 indicated that Internet obesity prevention program led to better behavioral and psychosocial outcomes when compared with traditional classroom education. Online obesity prevention programs have been successful in improving dietary behaviors, physical activity, and body mass index (BMI). 8 Literature suggests that there are inadequate online resources for adolescents for prevention and management of diabetes. 9,10
Two reviews that have focused on the effectiveness of Internet-based education for adolescents concerning nutrition education have acknowledged positive as well as negative or neutral outcomes. 5,8 The review articles have also noted that methodological issues such as power analysis for subject recruitment, randomization, and theoretical frameworks should be addressed in future studies.
Background for the Healthy Outcome for Teens Project
The HOT (Healthy Outcome for Teens) Project is an innovative online educational intervention for middle school students focusing on preventing diabetes and obesity by balancing food intake with physical activity. An existing interactive online module for adults (Your Guide to Diet and Diabetes) was modified to the reading level of middle school participants through a developmental process outlined in previous publications. 11 Furthermore, the preexisting modules were aligned with the triadic reciprocity of the social cognitive theory (SCT) variables such as self-efficacy and social persuasion 12 with verbal and visual positive feedback in learning games and observational learning through video.
The study was conducted in a Midwest county with three schools and included students from the 6th, 7th, and 8th grades, 62% of whom received free/reduced lunch. The racial demographics were similar in the three participating schools. Sample size calculations, based on a power analysis for a 2 (treatment or control) ×2 (measures [pre/post]) fixed effect of variance with α at 0.05 and an effect size (f) of 0.25, revealed that including 132 participants would result in 81% power (Sample Power version 2.0 software, 2000; SPSS, Chicago, IL). A 25% dropout rate was included for a recruitment goal of 165 participants (Fig. 1). The study was approved by the Institutional Review Board at the University of Illinois at Urbana-Champaign, and parental consent and child assent were obtained.
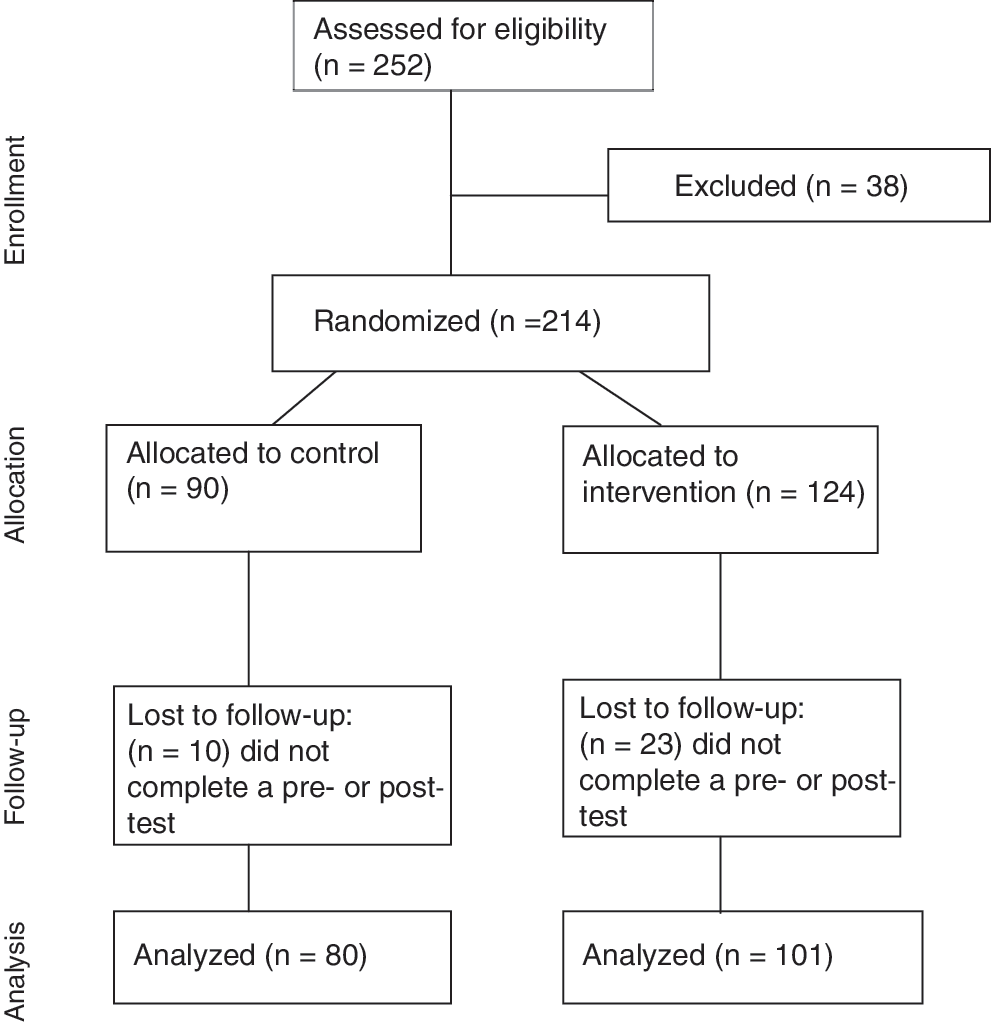
Consort diagram for the Health Outcomes for Teams Project.
The content and outcome measures in the HOT intervention were identified in a previous study 11,13 and included an overview of how food is related to diabetes, food groups and diabetes, physical activity and weight management, and eating for target blood glucose levels organized in five modules. Two versions of the Web site were created with the same information except the site for the treatment group had interactive features such as videos (observational learning), narrated text (social persuasion), and knowledge/skill-based games (outcome expectancies, self-efficacy), whereas the control group had passive, noninteractive texts.
The purpose of this study was to improve knowledge, outcome expectancies, self-efficacy, self-reported food intake, and skills through interactive online modules that compared a passive online learning (POL) control group (n=90) and a treatment group (n=124) that used active online learning (AOL). In line with previous literature, this project included a power analysis, randomization, and theory in development and evaluation.
An abstract of this article was presented as a poster at the Experimental Biology meeting in Spring 2011. 14
Subjects and Methods
Middle school students were recruited from three schools that had agreed to participate, with students meeting inclusion criteria of securing parental consent and participant assent and having diabetes or being at risk for diabetes. Risk for diabetes was defined as having two or more of the following: self-reported BMI at or above the 85th percentile 15 ; having a sibling with diabetes; having a parent or grandparent with diabetes; and getting little or no exercise. 16 Of the 214 subjects recruited, full data were secured for 181 students (80 in the control group and 101 in the treatment group) (Fig. 1). The randomization in the afterschool program was individualized. However, for those participating during class, participants were randomized by intact class cohorts to minimize the contamination of effects between the control and the treatment group. Each student participated in five sessions, 35–40 min in length, during health class, physical education class, or after school to cover the five modules of the intervention and to do a pre- and a posttest. Each participant received a gift valued at $50 for participation.
To assess comparative gain in knowledge, self-reported intake, and meal planning skills, and change in SCT constructs (outcome expectancies and self-efficacy), six questionnaires were administered online, pre/post, to both the AOL and POL groups. Personal factors for outcome expectancies were measured using previously validated survey items for exercise outcome expectancies (EOE) 17 and nutrition outcome expectancies (NOE). 18 Items for NOE originally referred only to fruits and vegetables (10 items); however, parallel questions were developed for low-fat eating (10 items), so the two surveys were referred to as NOE-FV and NOE-fat, respectively. Personal factors for self-efficacy were reflected by the Exercise Self-Efficacy (ESE) 19 questionnaire and the Weight Efficacy Lifestyle Questionnaire (WELQ). 20 The Planning a Meal (PM) referred to a skill-based activity in choosing the correct portion sizes for the plate. 12 The Rapid Eating Assessment Plan (REAP) referred to measuring food intake behavior. 21
Cronbach's α was >0.75 for all surveys, for which composite scores were calculated. The five skills (five food groups to correctly put on the plate) within the PM evaluation were assessed individually. Tests of kurtosis and skewness were used to assess the data normality, and nonparametric tests subsequently were used. The Mann–Whitney U test and the Kolmogorov–Smirnov test were conducted for the comparison between the control (POL) and treatment (AOL) groups. The intact control class cohorts as well as individually randomized afterschool students in the control group were compared as one group with intact treatment class cohorts as well as individually randomized afterschool students in the treatment group as the control group. Comparisons of baseline data for AOL and POL were not significantly different, except for NOE data. To compensate for this, a difference in scores between the pretest and posttest was computed as a new variable for NOE data. Data from the REAP were evaluated as a total and for items related specifically to fat (12 items [REAP-fat]) and fruits and vegetables (two items [REAP-FV]). Analysis also included descriptive statistics (i.e., median, 25th/75th percentile, and frequencies). The significance level was P<0.05.
Demographic data included self-reported gender, age, weight, and height. The BMI was calculated using the formula BMI=(weight/[height×height])×703, using weight in pounds and height in inches. The BMI Z-scores were also calculated to use for data analysis 22 and were assigned three categories, with −1 being the underweight category (Z-score values <0), 1 being the normal weight category (Z-score values from 0 to 2), and above 2 being the overweight category (Z-score values >2). 22 Data collected via the Internet within the HOT Project Web site were captured in Excel™ (Microsoft, Redmond, WA) and then exported to SPSS software (version 19.0 for Windows, 2010; SPSS, Inc.) for analysis.
Bivariate correlations (Spearman's ρ) were calculated to assess relationships among outcome expectation indicators, behavior indicators, and fat, fruits, and vegetables indicators. To evaluate the conceptual theory link, that is, whether the interventions' effect on mediating variables were related to the behavior changes, stepwise regression analyses were completed. 23 The dependent variable was fruit and vegetable and fat intake; exploratory regression analyses included self-efficacy and outcome expectancies as the dependent variables.
Results
Demographics
Four students had diabetes (2.2%), 31% were overweight or obese, 7.2% had siblings with diabetes, and 37% had parents or grandparents with diabetes. There was no difference based on gender for any preintervention scores. However, for postintervention scores, the only significant difference based on gender was NOE-fat for the AOL group as indicated in Table 1, with females having higher outcome expectations for fat (P=0.019).
Statistics were calculated by the Mann–Whitney test. Significance was defined by a P value of <0.05.
AOL, active online learning (treatment group); NOE, nutrition outcome expectancies; POL, passive online learning (control group).
PM skills
At the pretest, most students could not place the correct portions of meat, vegetable, starch, fruit, or dairy on the plate (Table 2). There were significant differences for the comparison between pre- and postintervention for the AOL for all the PM items (P<0.001), whereas there was no difference in the POL group. Comparison of postintervention results for PM items, AOL versus POL, was significantly different (P<0.0001). The largest improvement for the AOL group was for vegetables, followed by fruit; the smallest improvement was for meat. The POL group regressed in performance by performing poorer on the postintervention test for starch than they did for the pretest.
Statistics were calculated by the Mann–Whitney test. Significance was defined by a P value of <0.05 for frequencies and difference.
AOL, active online learning (treatment group); POL, passive online learning (control group); Q, survey question numbers.
ESE, WELQ, and REAP
At postintervention, no significant differences were found for composite scores of ESE (P=0.925), WELQ (P=0.465), and REAP (P=0.310) between AOL versus POL (by Mann–Whitney test) (Table 3). Significant improvement was found for the AOL group in seven of the 19 WELQ statements, which focused on eating under social pressure and stress (P<0.05). Significant improvements were also found for REAP-fat and REAP-FV categories for both AOL and POL groups, for preintervention scores versus postintervention scores comparison, but no significant difference between AOL versus POL.
Statistics were calculated by the Wilcoxon signed rank test. Significance was defined by a P value of <0.05.
Significant difference.
AOL, active online learning (treatment group); POL, passive online learning (control group).
NOE and EOE
At post-intervention, significant improvements with the AOL group were found for EOE (P=0.001) (Table 3). The posttest/pretest variable for NOE total, NOE-fat, and NOE-FV showed no significant differences for POL versus AOL analysis (data not shown).
Regression analysis
Significant equations were found for both the AOL and POL posttreatment groups for outcome expectations and intake of fruits and vegetables (REAP-FV), with additional significant results for the AOL group (Table 4).
Statistics were calculated by stepwise regression analysis. Significance was defined by a P value of <0.05.
AOL, active online learning (treatment group); EOE, exercise outcome expectations; ESE, exercise self-efficacy; FV, fruits and vegetables; NOE, nutrition outcome expectations; POL, passive online learning (control group); REAP, Rapid Eating Assessment Planning; WELQ, Weight Efficacy Lifestyle Questionnaire.
Discussion and Implications
In the HOT Project, participants in the AOL group improved significantly for all five categories of the PM questionnaire. This result suggests that for skill acquisition, an active learning venue is more effective than a passive online approach, as indicated by the PM survey results. Research literature indicates that the choice of pedagogy must take into account the desired outcomes, as it is suggested that traditional classrooms produce better mastery of recalled information, whereas the more technology-intensive classroom produce improved skills, hypothesis generation, and better ability to address a new problem. 24 The PM skills could be considered preliminary introduction to cooking and shopping skills 25 and may be a basis for providing additional opportunities for the participants to experience shopping and cooking skill development. Functional cooking skills related to food preparation have been used in online instruction when embedded videos are used. 26
In the HOT Project study, two constructs of SCT—outcome expectancies and self-efficacy—were incorporated in the intervention and assessed by the surveys. Outcome expectancies are the person's expectations about the consequences of an action. 12 Self-efficacy is the confidence in one's ability to perform the behavior. 12 There was a significant difference in EOE in the AOL group, suggesting that the activity demonstrations (modeling) in videos and pictures in the AOL group Web site had some impact. This improvement in EOE may reflect an eventual progress toward changing physical activity behavior because outcome expectancies have been documented as a determinant of physical activity among older adolescents. 27 The effects of outcome expectancies on exercise is generally less strong than that of self-efficacy, but people who exercise more report higher positive outcome expectancies. Cross-sectional studies have also shown that negative outcome expectations are negatively associated with exercise behavior. 28 Active learning, however, did not influence our subjects' self-efficacy related to exercise (ESE). Taymoori et al. 29 indicated self-efficacy and outcome expectations to be direct predictors of physical activity for adolescent girls. Although social support has been modeled as an antecedent of self-efficacy and outcome expectations, 29 the HOT Project study did not incorporate family/peer support directly, and the physical activity behavior was not measured postintervention. Although the surveys used in this study had adequate reliability as measured by Cronbach's α, additional SCT scales for use with adolescents concerning physical activity and dietary behaviors have been extensively tested and may provide a more applicable method for ascertaining correlates of behavior in the future. 30
In the HOT intervention, there appeared to be no advantage to the active learning venue for certain eating behaviors, certain items of weight efficacy, and ESE as there were no significant differences between AOL and POL for these measures. However, both AOL and POL groups improved significantly for REAP-fat and REAP-FV categories in the REAP survey. Similar results have been seen in a short-duration study conducted by Muth et al. 31 to improve nutrition in school-aged children. Thunfors et al. 32 suggested that pre- to early adolescence may be a more fruitful age than later adolescence for implementing interventions to encourage health behaviors. Surveys have shown that fruit and vegetable intake decreases through adolescence, suggesting a need to intervene, targeting improvement in fruit and vegetable intake of adolescents. 33 Our HOT Project is in line with the above information and targeted early adolescents in the 6th, 7th and 8th grade.
Our regression analysis results suggested that the WELQ was more associated with EOE than with ESE or NOE. This may be explained by the fact that healthy eating and exercise are the two factors that balance weight. 34 In a slightly older audience of first-year college students, the WELQ, “trigger situations,” and social pressure for eating behavior were found to be consistent between normal and overweight older adolescents. 35 These areas could also be explored more fully in the middle school-age adolescents and could also be modeled within the online curriculum. The WELQ has also been used to understand binge eating disorders within the female adolescent population, with the belief of one's ability to refrain from eating when food is explicitly available being particularly relevant to achieving a healthy weight. 36
The HOT Project results also indicated that habits, especially about fat and weight, are significant in explaining NOE-FV. NOE-fat and NOE-FV are inversely related in our study, as the subjects in the HOT intervention developed outcome expectations to increase fruit and vegetable intake and decrease fat intake. Healthy People 2020 goals also emphasize incorporating more fruits and vegetables in the diet and limiting total and saturated fat for weight management. 37 In the Diabetes in Adolescents and Youth Study, high fat and saturated fat and low fruit and vegetable intakes were reported, which can increase the risk for diet and obesity related chronic diseases in the future. 38 Thus, any intervention that can positively influence these foods and nutrients would be beneficial. This may be especially true for online programs such as the HOT Project.
The HOT Project study had its limitations in that the intervention posttest was administered very close in time to the pretest, not giving the participants much time to internalize the information and bring about a change in measures of self-efficacy and outcome expectations. Although there were no significant changes in self-efficacy, the researchers believe that it still may be plausible, if more time and participant support were provided, because it takes time for attitudes to change. 39 Changes in self-efficacy usually precede changes in outcome expectations. 31 A longer intervention may be needed to produce strong enough effects on mediating variables to achieve an increase in physical activity and eating a healthy diet. 40
Second, the study did not specify that students were low in SCT beliefs at baseline. There would be increased chances of finding significant improvements if individuals low in such beliefs were selected. 41 Analysis could have been completed with this subset of students, but statistical power would have been lost.
Third, although programs developed in accordance with SCT have proved to be effective in changing individuals' health behaviors, including nutrition behavior, 39 not all constructs of the SCT were used in this project. Social support and self-regulation were not specifically addressed in the HOT intervention. Strengthening the content to include social support and self-regulation and further targeting self-efficacy and outcome expectations may be important to achieve behavior change. Indeed, family support and peer social support have also been shown to be related to physical activity and healthy eating. 40
Fourth, there was no postintervention follow-up, which may have indicated improvement in SCT mediators, allowing for changes in the types of self-perception necessary for observing changes in SCT constructs. 41
Fifth, we randomized the subjects as an intact class cohort, assigning the entire class to either the treatment group or the control group. This randomization assisted in preventing contamination of effects between the study groups.
Finally, we did not measure BMI postintervention, but BMI does not change significantly for a short 2-week intervention. Moreover, BMI is less likely to be improved by a school-based health education intervention. 42 Despite its limitations, the strengths of the study include the application of a well-established theoretical framework and the use of powerful statistical mediation techniques, which allowed the testing of SCT mediators. Moreover, validated questionnaires were used to assess SCT variables and behavior. Additionally, Cronbach's α was high for all surveys in which items were grouped to reflect a psychosocial variable or behavior.
Conclusions and Future Directions
Future research is needed to determine which theories and theoretical constructs are most suitable for the adolescent population to improve health-related behavior. From the results of the study, we conclude that teens participating in active online version of the HOT Project intervention acquired skills for planning a meal, improved in confidence in eating under social pressure and stress, and improved outcome expectations for exercise, and girls improved in outcome expectancies for nutrition related to dietary fat intake. However, no improvement was found for the self-efficacy constructs of the SCT for exercise and other outcome expectations for nutrition. A review conducted by Cerin et al. 23 suggested that interventions aimed at youth will improve their efficacy by targeting key constructs of either the SCT or the theory of planned behavior. There is research evidence that constructs of the theory of planned behavior such as attitudes, subjective norms, and perceived behavioral control can show more rapid changes than SCT constructs and may make it more suitable to apply to short-term interventions. 42 Therefore, to further optimize the effectiveness of this intervention, a framework including the theory of planned behavior constructs (Ajzen I) could be developed.
Footnotes
Acknowledgments
This work was supported by the American Dietetic Association Foundation, National Soybean Laboratory at the University of Illinois, University of Illinois Extension, and Illinois AMVETs. We are grateful for the staff at the Web Coordination and Urban Programming Office of Extension Web Development and graduate students at the University of Illinois at Urbana-Champaign for their help with program development and implementation. We would also like to thank the schools, teachers, and study participants.
Author Disclosure Statement
No competing financial interests exist.