
Abstract
Objective:
This study assessed the level of patient satisfaction with diabetes remote consultations via videoconferencing in a virtual outreach clinic.
Materials and Methods:
A cross-sectional observational survey was conducted of people with diabetes who were living in regional cities of Queensland, Australia, and remotely consulted by endocrinologists at the Princess Alexandra Hospital tele-endocrinology clinic in Brisbane during autumn 2013. A questionnaire with 15 multiple-choice questions and one open-ended question was developed for assessing patient satisfaction with videoconferencing for specialty consultation. The questionnaire items showed strong internal consistency (Cronbach's α=0.90). Patient satisfaction was assessed by this 16-item questionnaire exploring four dimensions: equipment/technical issues; communication and rapport; clinical assessment; and program evaluation.
Results:
In total, 62 questionnaires were mailed to the patients, with 24 (39%) surveys completed and returned. The quality of video had the highest satisfaction rate (100%). The lowest satisfaction scores were reported in the “Clinical Assessment” dimension, in which 21% of respondents (five of 24) were concerned that the lack of physical contact could be a problem for managing their diabetes. The patients did not report any problem with building rapport with their consultant over the videoconference.
Conclusions:
The patients with diabetes who were seen remotely by endocrinologists via videoconferencing were generally satisfied with remote consultation. The questionnaire developed specifically for diabetes video teleconsultation in this study is useful for the measurement of patient satisfaction, and a modified version may be used in other clinical specialties.
Introduction
S
In the field of telemedicine, researchers have emphasized that successful implementation and adoption of telemedicine services depend on acceptance and satisfaction of both healthcare consumers and service providers. 6 Despite numerous publications on patient satisfaction with telemedicine, 7 –10 it has been identified that this aspect of telemedicine needs further investigation. 11,12 The published works on telemedicine satisfaction tend to rely on a general assumption that both patient and provider levels of satisfaction with telemedicine are high. Thus further research on patient satisfaction has been a lower priority compared with other domains of telemedicine research such as effectiveness, reliability, or economic benefit. However, there are several insufficiencies associated with satisfaction studies that limit the generalizability of the findings. 11 In addition to general shortcomings of satisfaction studies such as inability to identify the concept and ambiguity in the definition of outcome measures, most of the telemedicine satisfaction studies have been part of exploratory, demonstration, or feasibility studies, rather than surveying a well-established and operational telemedicine service. Furthermore, the patient selection criteria and refusal rate have not been clearly stated in most studies. This suggests the possibility of selection bias in favor of higher levels of satisfaction. 13
In a systematic review of literature, Mair and Whitten 11 analyzed the quality of the satisfaction studies of real-time telemedicine services and more specifically video consultation for publications from 1989 to 1998. They highlighted several limitations with the published work. Only a few studies defined satisfaction, and of those that did, all used different definitions. Therefore it was not possible to discern from the studies which satisfaction parameters they have evaluated. The settings of the studies were also quite heterogeneous. For instance, one of the largest U.S. studies in this field was conducted in a prison setting, which is quite different from the usual clinical environment. 14
Because telemedicine research involves the use of a range of modalities and communication technologies, it is challenging to find a universal set of questions that apply to all telemedicine solutions. For example, a questionnaire developed for a store-and-forward telemedicine project is not suitable for interactive video consultations, and vice versa. As videoconferencing is gaining more popularity for both patient education and remote consultation, there is a need for the development of a reliable and validated instrument for assessing the level of satisfaction with the services that are delivered remotely via videoconference. The aim of this study was to evaluate patient satisfaction with interactive video teleconsultation in a virtual diabetes outreach clinic.
Materials and Methods
Settings of the virtual outreach clinic
The Princess Alexandra Hospital (PAH) is a tertiary teaching hospital in Brisbane, QLD, Australia. It operates a wide range of conventional outpatient clinics, including diabetes and endocrinology. Recently, the PAH Telehealth Centre was established to enhance the capacity of several traditional outreach clinics serving rural areas of Queensland by means of interactive videoconferencing. Specialist doctors from several clinical disciplines, including diabetes and endocrinology, as well as cardiology, orthopedics, geriatrics, and dermatology, provide teleconsultations via videoconferencing to those patients referred by their general practitioner (GP) for specialty consultation. The details of the telemedicine service for diabetes patients and analysis of the process of care provided remotely to them have been published elsewhere. 15 The service delivery conforms to the hub-and-spoke model, 16 in which all the administration and coordination tasks are carried out centrally from the PAH (the hub). The distance of remote sites (the spokes) from the hub varies from 220 km to 1,700 km (Fig. 1).
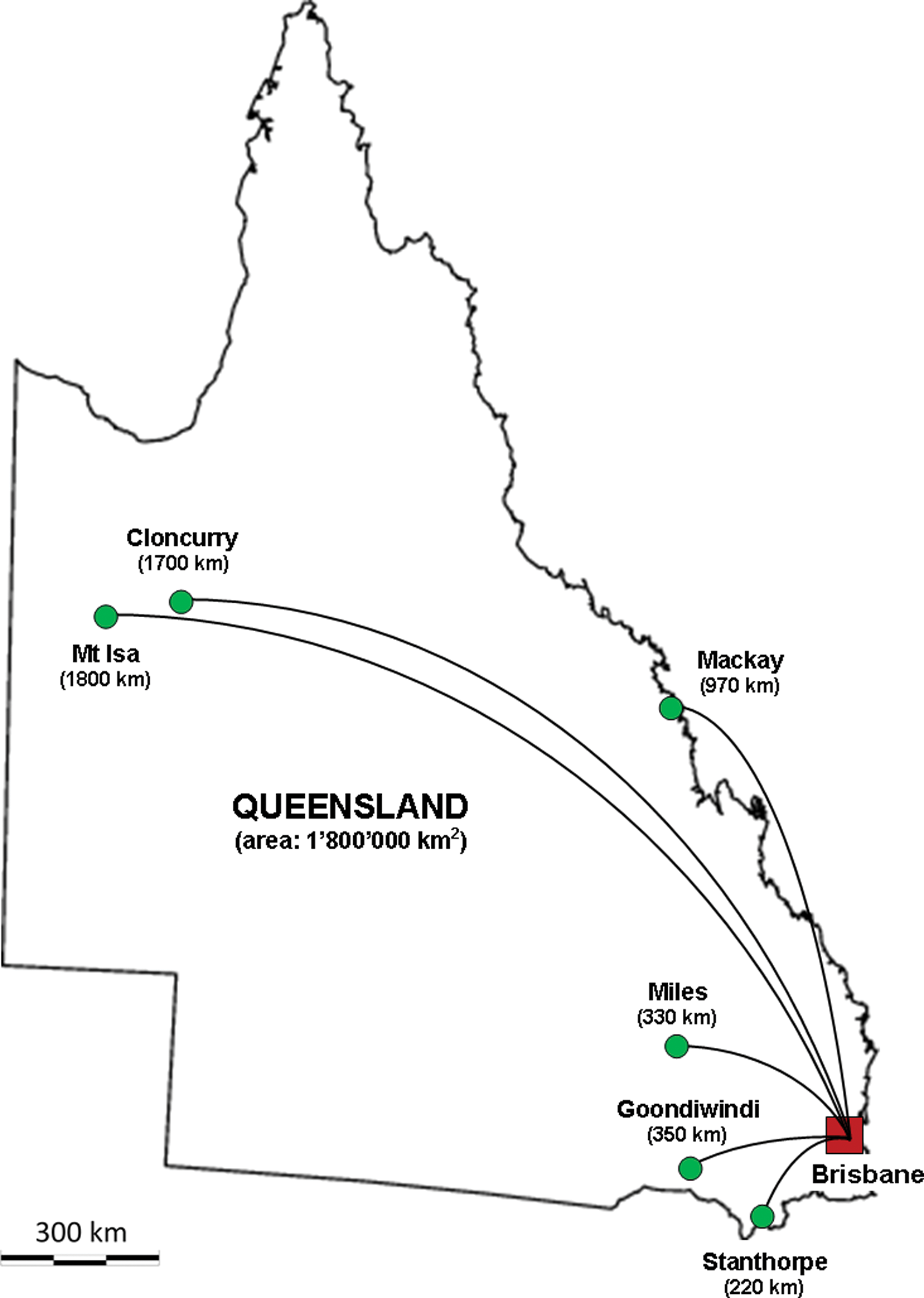
The locations of cities where the diabetes remote consultation was delivered, with their distance to Brisbane, the capital city of Queensland. Color images available online at
The patients who are living elsewhere need to travel to the nearest health center (spoke) to access a videoconferencing system for their teleconsultation with a specialist based in Brisbane. The videoconferencing is achieved using the Queensland Health Wide Area Network, which is a high-speed network that connects to all Queensland Health end points across the state. Both local and remote sites are equipped with dedicated videoconferencing units, including TV screen, commercial grade codec, pan-tilt-zoom camera, and microphone. The general connection speed (technically referred to as bandwidth) ranges from 512 kbits/s to 2.3 Mbits/s, depending on the site-specific connections. The video consultation is hosted by a local clinician (doctor, nurse, or allied health professional) when available. In some cases, the patient may be accompanied by a friend or family member during the videoconference.
Development of the questionnaire
No validated questionnaire was found in the published literature for assessing satisfaction of patients with video teleconsultation. The main domains of satisfaction with real-time telemedicine were identified through review of the literature, and a set of questions was accumulated from three relevant studies. 17 –19 After duplicate and similar items were removed, 16 questions were selected by a panel of experts. The panel comprised two specialist doctors (one endocrinologist and one geriatrician) with at least 5 years of video teleconsultation experience and two senior researchers with more than 9 years of research in the field of telemedicine.
A questionnaire with 15 multiple-choice questions and one open-ended question was developed to assess satisfaction of diabetes patients who have had an appointment with their endocrinologist via videoconference. The multiple-choice questions scored on a 5-point Likert-type scale (from 1 for strongly disagree to 5 for strongly agree). These questions covered four domains of satisfaction with the video consultation: equipment and technical issues (three questions); communication and rapport (three questions); clinical assessment (four questions); and overall evaluation of the program (five questions). The open-ended free-text question enabled the participants to comment on their experience with the video consultation and express their opinion in this regard (Table 1).
The questionnaire had a scoring range of 15–75. A score of 15 indicates all responses as “strongly disagree,” and a score of 75 means all responses were “strongly agree.” Higher scores favor video consultation, and lower scores favor conventional face-to-face consultations. The overall internal consistency (Cronbach's α) of the questions was 0.90, which indicates a strong correlation between the 15 items of the questionnaire. It was 0.80 for the equipment/technical issues, 0.64 for the communication/rapport, 0.82 for medical concerns, and 0.85 for the program evaluation (Table 2). For new questionnaires, an internal consistency of more than 0.7 is regarded as acceptable. 20
Participants
Those people with diabetes who had a video consultation with specialists at the PAH Telehealth Centre between March and May 2013 were included in the study. The questionnaire was mailed to the patients' postal address along with a prepaid self-addressed envelope for returning the completed questionnaire. The questionnaire was anonymous. It was decided that the completed questionnaire would be returned to the research team (not the healthcare providers), to minimize the potential for biased responses. The study protocol was approved by the appropriate institutional ethics committee (reference number HREC/12/QPAH/479). Participation in the study was voluntary, and completing the survey implied a participant's consent.
Statistical analyses
Reliability of the instrument was measured by internal consistency among all questions as well as within each of the four subgroups. Internal consistency was evaluated by Cronbach's α. No attempt was made to assess the repeatability of the instrument. As the survey was completed anonymously, it was not possible to report demographic information or compare information between respondents and nonrespondents.
Results
Patients' satisfaction with video teleconsultation
In total, 62 questionnaires were sent via mail to patients who had video consultations with a specialist at the PAH Telehealth Centre, and 24 completed questionnaires were returned. We were not able to check what proportion of questionnaires was delivered to the intended persons and how many were sent back to the researchers. There are anecdotes on instances of failure of postal delivery services in rural areas in which the subjects of this survey resided.
Patients' responses to the questionnaire on satisfaction with videoconferencing are summarized in Table 3. On average, more than 22 of the 24 respondents were satisfied/highly satisfied with the equipment and technical features of the videoconference appointment. Also, almost all (23 of 24) of the patients were satisfied with their communication with the specialist via videoconference. The primary focus of dissatisfaction for patients was the perception of the clinical assessment through video consultation. Five respondents reported that the lack of physical contact could be a problem for managing diabetes. Almost all the participants (23 of 24) reported that telemedicine had improved their access to specialist care and would like to use the service again.
Data are the number of responses in each category.
Patients' comments on the remote consultation service
One-third (eight of 24) of the respondents provided comments in the open-ended question regarding their opinion and experience of remote consultation via videoconferencing. Five patients expressed their appreciation and satisfaction with the service, mostly because of avoidance of travel and saving money. One respondent was concerned that the strict scheduling of telehealth appointments could introduce the feeling of being rushed in order to keep to schedule. One respondent expressed unhappiness with the nurse who hosted the remote consultation, and finally one respondent expressed his or her preference for in-person consultation rather than video teleconsultation.
Discussion
Telemedicine differs from conventional face-to-face encounters in several ways that may adversely affect the doctor–patient relationship. Inability to perform a physical examination and decreased nonverbal communication are among the most important concerns in remote consultations. 21 These characteristics may contribute to patient dissatisfaction. However, a recent comprehensive literature review shows that videoconferencing has been used for remote consultation of patients in a range of medical disciplines, including the ones that may rely more on physical examination, such as neurology. 22 Previous studies have evaluated the level of satisfaction with telemedicine services from various perspectives, but no validated questionnaire was found in the literature specifically designed for video teleconsultation. In this study, we developed a patient satisfaction questionnaire and evaluated the level of diabetes patient satisfaction with remote video consultations.
Our survey showed that some patients were concerned with the lack of physical contact in remote consultation via videoconferencing. This may reflect concern about the long-term complications of diabetes such as foot ulcers or diabetic retinopathy. In circumstances when this is an issue, the endocrinologist would work in partnership with the patient's GP or nurse practitioner, to observe the physical examination being completed if the GP or nurse was in attendance with the patient for the videoconference or to ask for a physical examination to be completed by the GP at the patient's next clinical visit. Previous research shows, from an endocrinologist's perspective, that a GP or a trained nurse can perform the physical examination needed for a diabetes specialist consultation. 23 Despite this issue, the overall proportion of patients with such concerns (five of 24) was relatively low. This supports the findings of other studies on patient satisfaction with telemedicine. 17 Most of the patients (22 of 24) reported their confidence with the clinical assessment of the doctor of their health condition and medication requirement.
All of the respondents in this survey were satisfied with the quality of video during the consultation. One respondent reported dissatisfaction with the audio transmission. None of the respondents indicated any technical difficulty with the videoconferencing. This level of satisfaction with technical aspects of telemedicine is mainly due to highly reliable infrastructure and networking available in the Queensland public hospitals, clinics, and health centers throughout the state. Similar reliable networks and telehealth infrastructure may not be available in other countries.
The comment from one of the respondents on the attitude of the nurse who hosted the remote consultation at the remote side and the responses to the questionnaire shows that he or she has differentiated the level of satisfaction with the vehicle of healthcare delivery from the people who are providing the service, but it could be not true for some people. In order to isolate these two determinants of the healthcare quality (personnel and modality), future studies on development of satisfaction assessment instrument may consider inclusion of a separate set of questions to evaluate the performance of the personnel while asking for the satisfaction with the modality (e.g. videoconferencing).
All the administrative tasks and coordination functions of telemedicine sessions were conducted centrally by the personnel of the PAH Telehealth Centre, which eliminated the burden of those issues from the people on the patient's side. Also, as the patients were attending their local clinic or health center for the videoconference, they did not have to know how to operate the telemedicine equipment; this issue should be specifically considered when evaluating home telecare services in which the remote device needs to be operated by the patients themselves, caregivers, and/or family members.
This study has several limitations. The number of subjects participating in this study and the response rate were not high, and diabetes was the only health condition investigated. Provision of remote consultations for other diseases may need different requirements in terms of physical examination (e.g., for orthopedics) or audio/video quality (e.g., for dermatology) that should be considered in developing a comprehensive instrument. Also, the setting of our study (videoconferencing between a hospital and a rural clinic) limits the generalizability of the results, so that for other situations such as home telecare in which the patients need to operate the telemedicine device by themselves, additional sets of questions should be added to the questionnaire. The questionnaire introduced in this study may be regarded as a preliminary version of an instrument for assessing the satisfaction of patients with remote consultation using videoconferencing. Although the questions have been formulated in the context of diabetes, the specific scripting could be modified to suit other health conditions. Further research is required to confirm the validity of the questionnaire introduced in this article.
Conclusions
The survey demonstrated that patients who had an appointment with their specialist via videoconferencing were generally satisfied with the service provided. This preliminary evidence shows that the questionnaire developed in this study is useful for the measurement of diabetes patients' satisfaction with interactive video teleconsultation and could be modified for use in other clinical specialties.
Footnotes
Acknowledgments
We are grateful for the support of the PAH Telehealth Centre and the Department of Diabetes and Endocrinology at the Princess Alexandra Hospital in Brisbane, Australia. We also thank the patients for their participation in this study. Funding support was provided by the Australian Commonwealth Government, the Queensland Government, and the Centre for Online Health. We also thank Queensland Gas Company Pty. Ltd. for funding research into telehealth in the Western Downs.
Author Disclosure Statement
No competing financial interests exist. F.F. designed the study, collected and researched data, and wrote the manuscript. M.M.-K. and A.C.S. designed the study and edited the manuscript. L.C.G. and A.W.R. designed the study and reviewed and revised the manuscript. F.F. is the sole guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of data analysis.