
Abstract
Background:
Devices for the treatment of diabetes are not always used as recommended in good practice. Our aim was to evaluate potential insulin underdelivery in cases of premature needle withdrawal after injection with insulin pens, which is a commonly observed misuse, especially in young type 1 diabetes patients.
Materials and Methods:
Potential insulin underdelivery was evaluated using five prefilled insulin pens (lispro Kwikpen® [Eli Lilly, Indianapolis, IN], aspart Flexpen® [Novo Nordisk, Bagsvaerd, Denmark], glulisine Solostar® [Sanofi, Paris, France], detemir Flexpen® [Novo Nordisk], and glargine Solostar® [Sanofi]) and three reusable insulin pens (Humapen® Luxura HD with lispro cartridge [Eli Lilly], Novopen® Echo with aspart and detemir cartridge [Novo Nordisk], and JuniorSTAR® with glulisine and glargine cartridge [Sanofi]) in a laboratory. For each pen and insulin, we simulated premature needle withdrawal 2 and 3 s after an insulin injection of 5 and 10 units, respectively.
Results:
With prefilled pens, mean potential insulin underdelivery was 0.43±0.30 and 0.44±0.32 units after injection of 5 and 10 units, respectively. With reusable pens, mean potential insulin underdelivery was lower (0.29±0.13 and 0.29±0.12 units after injection of 5 and 10 units, respectively; P<0.001). The results were heterogeneous across pens, ranging from 2.6%/1.6% to 20.2%/8.6% of the selected insulin dose for prefilled/reusable pens, respectively (P<0.001).
Conclusions:
Potential insulin underdelivery varies across prefilled and reusable insulin pens but may represent up to one-fifth of the total injected dose. Clinicians should be aware of the potential consequences of premature needle withdrawal and should reinforce insulin injection education.
Introduction
T
Materials and Methods
This laboratory evaluation assessed prolonged leakage of five prefilled insulin pens (lispro Kwikpen® [lisK] [Eli Lilly, Indianapolis, IN], aspart Flexpen® [aspF] and detemir Flexpen [detF] [Novo Nordisk, Bagsvaerd, Denmark], glulisine Solostar® [gluS] and glargine Solostar [glaS] [Sanofi, Paris, France]) and three reusable insulin pens (Humapen® Luxura HD with lispro cartridge [lisH] [Eli Lilly], Novopen® Echo with aspart cartridge [aspN] and detemir cartridge [detN] [Novo Nordisk], and JuniorSTAR® with glulisine cartridge [gluJ] and glargine cartridge [glaJ] (Sanofi)]. These three reusable pens were chosen because they all offered a half-unit injection, which is an important feature for patients with low insulin needs (e.g., children).
All pens and cartridges were provided by the hospital pharmacy of the investigation center. BD Micro-Fine Ultra® 4-mm needles (Becton, Dickinson and Co., Franklin Lakes, NJ) were applied to the prefilled insulin pens as recommended by the manufacturer. All of the experiments were performed in a single laboratory at ambient temperature by the same investigator to improve reproducibility. Insulin pens were operated as recommended. A digital chronometer was used to ensure time compliance during the assessments.
After priming with 4 units (U), all of the pens were assessed with the same method. In brief, the 5-U setting was selected, and the injection button was pushed with the maximum thumb strength of the operator to express insulin into a discard beaker for 2 s. Then, while the injection button remained depressed for an additional 8 s (the total time was 10 s), the remaining drops were ejected into another beaker. This amount of insulin collected was called PIUD and was weighed on an analytical balance that had been previously calibrated and tared with an accuracy of 0.01 mg (Sartorius Pesage Industrie, Les Ulis, France). This experiment was repeated 10 times using two different prefilled pens from each brand. For reusable pens, the assessment was also repeated 10 times using two different cartridges for each type of insulin.
The same procedure was also applied for 10 U of insulin. For this dose, insulin was discarded for 3 s, but the total time during which the injection button remained depressed was 10 s (thus, the time for collecting PIUD was 7 s).
Discard times of 2 and 3 s for the doses of 5 and 10 U, respectively, were chosen because they corresponded to the time of an observed insulin stream before dribbling. Overall, 20 PIUD measurements were performed for each pen with each insulin type at each dose. To convert insulin mass into units, we used a proportional relationship after weighing 10 U of each insulin type eight times.
Quantitative data are expressed as mean±SD values. Student's t tests were used for intra- and intergroup comparisons. Statistical analysis was performed using SAS version 9.4 software (SAS Institute Inc., Cary, NC). A P value of <0.05 denoted statistical significance.
Results
Prefilled pens
For a 5-U injection, mean PIUD was 0.53±0.35 U for rapid-acting analogs (ranging from 0.28±0.09 U [aspF] to 1.01±0.07 U [gluS]; P<0.001) and 0.27±0.07 U for basal analogs (ranging from 0.22±0.04 U [detF] to 0.31±0.05 U [glaS]; P<0.001). Expressed as a percentage of the selected dose, PIUD represented up to 20.2%/10.7% and 6.3%/2.9% for 5/10 U of glulisine and glargine with Solostar, respectively (Table 1 and Fig. 1).
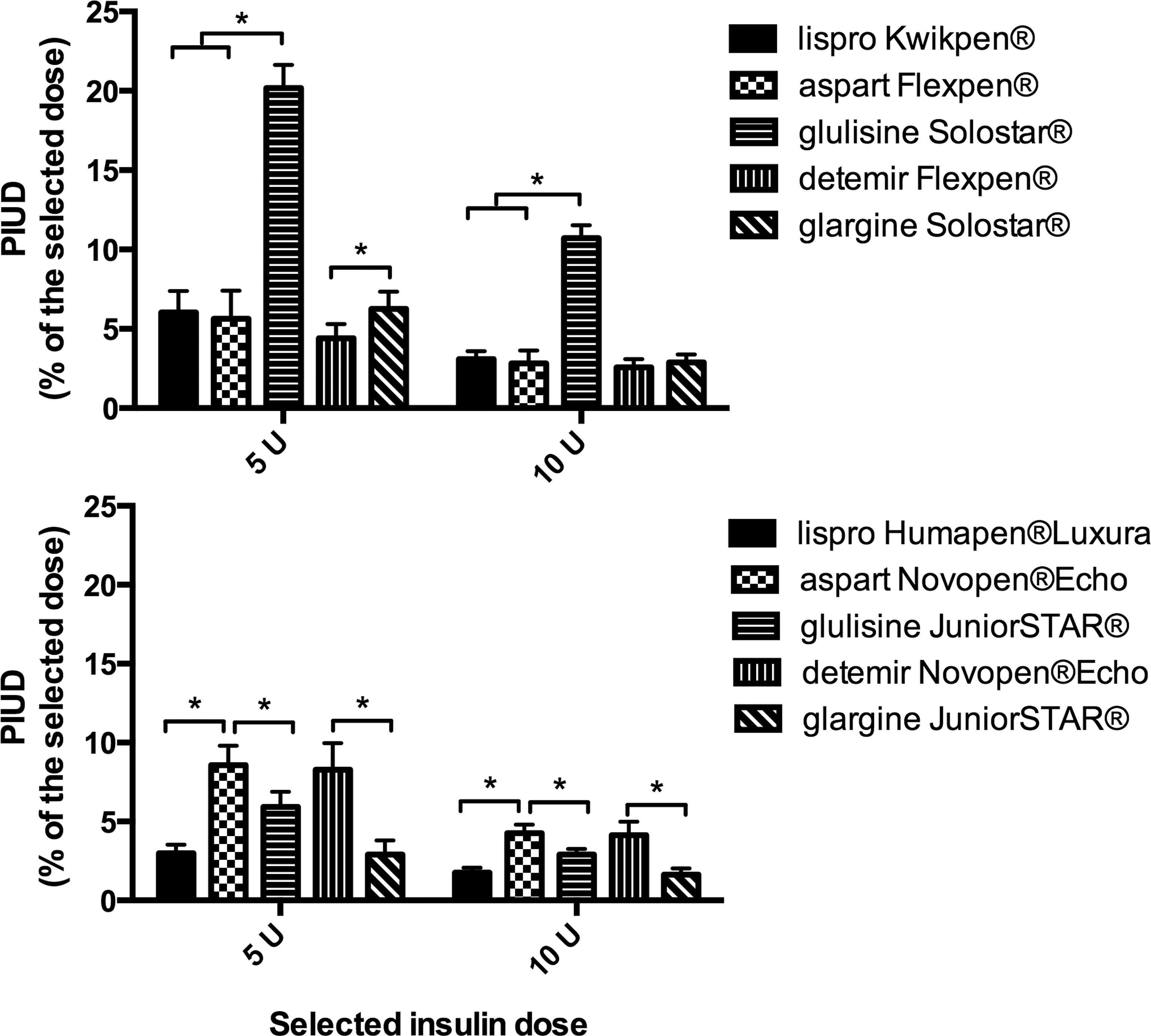
Potential insulin underdelivery (PIUD) expressed as a percentage of the selected insulin dose for 5- and 10-unit (U) doses when simulating premature needle withdrawal after injection with
Data are mean±SD values, expressed in units (% of selected dose). The five prefilled insulin pens were the lispro Kwikpen, aspart Flexpen, glulisine Solostar, detemir Flexpen, and glargine Solostar. The three reusable insulin pens were the lispro cartridge in Humapen Luxura HD, aspart cartridge in Novopen Echo, glulisine cartridge in JuniorSTAR, detemir cartridge in Novopen Echo, and glargine cartridge in JuniorSTAR.
PIUD, potential insulin underdelivery.
Reusable pens
For a 5-U injection with reusable pens, the mean PIUD was 0.29±0.12 U for rapid-acting analogs (ranging from 0.15±0.03 U [lisH] to 0.43±0.06 U [aspN]; P<0.001) and 0.28±0.15 for basal analogs (ranging from 0.15±0.03 U [glaJ] to 0.41±0.08 U [detN]; P<0.001). Expressed as a percentage of the selected dose, PIUD was highest for 5/10 U of aspart and detemir with Novopen Echo (8.6%/4.3% and 8.3%/4.1%, respectively) (Table 1 and Fig. 1).
Comparison of prefilled versus reusable pens
For lispro, glulisine, and glargine, PIUD after a 5-U injection was significantly higher with prefilled pens (lisK, 0.30±0.07 U; gluS, 1.01±0.07 U; glaS, 0.31±0.05 U) compared with reusable pens (lisH, 0.15±0.03 U; gluJ, 0.30±0.05 U; glaJ, 0.15±0.03 U) (P<0.001 for each insulin). Conversely, for aspart and detemir, PIUD was significantly lower with prefilled pens (aspF, 0.28±0.09 U; detF, 0.22±0.04 U) compared with reusable pens (aspN, 0.43±0.06 U; detN, 0.41±0.08) (P<0.001 for each insulin).
Comparison of rapid-acting and basal analogs with the same pen
For the Solostar and JuniorSTAR pens, PIUD was significantly higher with the rapid-acting analog glulisine compared with the basal analog glargine (for example, 5 U delivered with Solostar was 1.01±0.07 U compared with 0.31±0.05 U, respectively; P<0.001). However, PIUD was similar with the rapid-acting analog aspart and the basal analog detemir using the Flexpen and Novopen Echo pens.
Discussion
We have demonstrated in this laboratory study that during an insulin injection with prefilled or reusable insulin pens, prolonged insulin leakage after the initial stream represents a non-negligible amount of insulin, especially at small doses. Thus, in patients who do not properly use insulin pens and prematurely withdraw the needle, prolonged leakage implies that some insulin remains undelivered. This phenomenon may be critical for subjects with low insulin needs (such as children) because the percentage of potentially undelivered insulin is negatively correlated with the selected dose. For example, in one prefilled pen, the PIUD was 20.2%, 10.7%, and 6.0% at the 5-, 10-, and 20-U doses, respectively (data not shown).
In this particular situation of premature needle withdrawal, the reusable pens Humapen Luxura HD and JuniorSTAR should be preferred to their prefilled counterparts (Kwikpen and Solostar) because they were more efficient and had a significantly lower PIUD.
These discrepancies among pen brands should be mostly explained by structural differences. First, the softness of the rubber used in the plunger might play an important role. Indeed, when the injection stroke starts, the first thing that happens is the screw pushes on the rubber plunger in the cartridge. The plunger, being made of rubber, will compress a small amount before it starts moving forward. A softer rubber will compress more at the start of the injection stroke and requires more time to expand back to its original shape after the injection is complete. Conversely, a harder rubber compresses less at the start and expands back to its original length more quickly. Additionally, the device's internal frictional properties might contribute to the injection time observed with insulin pens: the injection force applied on the injection button is indirectly transferred through all of the plastic elements of the pen to the insulin column and is also used for rotating the dose indicator, which must return to zero for the next injection. These steps result in frictional forces that probably occupy an incompressible amount of time, which is longer than that observed with a syringe where the injection force exerted on the piston is directly transferred to insulin, without any lag time. These structural characteristics also explain that the injection force required and the length of dial extension may be different between pens. 3
Furthermore, the physical characteristics of insulin, such as its viscosity, are likely involved in the duration of insulin stroke because we observed significant differences in PIUD by insulin type in the same pen (PIUD is significantly lower for glargine compared with glulisine with Solostar and JuniorSTAR).
Finally, inner needle diameter should also be involved; however, in our study, we used the same 4-mm needles, ruling out this alternative hypothesis. Our choice to use these 4-mm needles exclusively was guided by recent data demonstrating that these small needles result in the same glycemic control as 5- and 8-mm needles with less pain in adults and children. 4,5
However, insulin underdelivery can easily be avoided by following the manufacturer's recommendation on the package insert of each insulin pen. To ensure that the entire dose is delivered, the needle should remain under the skin for 5 s (Kwikpen and Humapen Luxura HD), 6 s (Flexpen and Novopen Echo), or 10 s (Solostar and JuniorSTAR) after injection (per the official device manuals). For the Solostar pen, the recommended time before withdrawing the needle is longer, which is consistent with our results of a higher PIUD with the misuse of this pen.
Beyond the manufacturer's recommendations for the proper use of all insulin pens, an expert panel advised counting slowly to 10 before withdrawing the needle to deliver the full dose and prevent medication leakage. 6 This recommendation relies on an in vivo study that explored the leakage from six different insulin pens after 1–7 s of needle withdrawal; the amount of insulin lost was variable depending on the pen used and the timing of needle withdrawal. 7 This study was conducted over 10 years ago, and most of the pens tested are no longer used. More recent studies have assessed the accuracy of most of the prefilled and reusable insulin pens evaluated in our study (Kwikpen, Flexpen, Solostar, Novopen Echo, and Humapen Luxura HD). All of the tested insulin pens met the requirements for accuracy according the International Organization for Standardization (ISO) guidelines for insulin pen injectors (ISO 11608-1). 8 –11 However, our laboratory evaluation provides additional data because none of these previous studies has explored prolonged insulin leakage from the needle tip after premature needle withdrawal.
The loss of insulin at the needle tip should be distinguished from another related and previously described situation, which is insulin leakage from the puncture. 12 Stewart and Darlow 12 explored the amount of insulin leakage from the skin shortly after giving an injection using a filter paper technique. They demonstrated that 23% of insulin injections were followed by insulin leakage of more than 5% of the injected dose, resulting in irregular insulin delivery that may increase glycemic variability. 13 We demonstrate in our study that insulin leakage from the needle tip could also contribute to irregular insulin delivery and impaired glucose control in case of premature needle withdrawal.
Our study has several limitations. Only one needle size (4 mm) was explored. Using an automated test system to depress the injection button of the pen would have been more reproducible, but we preferred testing our hypothesis with manual handling as it more closely mirrored reality and allowed for global exploration of pen ergonomics (length, weight, pen diameter, injection button access, and stroke smoothness). 14 We acknowledge that pen handling in children's hands might have revealed different results compared with our evaluation by an adult operator (especially concerning the thumb length and strength required to push the injection button). Finally, this laboratory evaluation cannot preclude what might happen during a real injection through the skin; therefore, the potential consequences on patient glycemic control are only speculative.
However, our results should promote clinician awareness of the importance of carefully teaching the insulin injection technique, especially for patients requiring small doses. Patient education should be reinforced, highlighting the importance of waiting before withdrawing the needle after an insulin pen injection to avoid insulin underdelivery, which can represent up to 20% of the selected dose.
Footnotes
Author Disclosure Statement
M.J. and Y.R. conduced clinical trials as co-investigators, provided advisory services, and attended conferences as contributors for Eli Lilly, Novo Nordisk, and Sanofi. A.H., J.M., and A.R. declare no competing interests exist.