
Abstract
Background:
The latest American Association of Clinical Endocrinologists/American College of Endocrinologists consensus statement published in 2014 does not recommend continuous subcutaneous insulin infusion (CSII) in patients with mental health problems. This study investigated the use and discontinuation of CSII in daily routine care of type 1 diabetes (T1D) patients with or without comorbid mental disorders.
Materials and Methods:
Insulin-treated T1D patients (n = 48,700) between 5 and 30 years of age (median [interquartile range], 15.6 [12.0–17.7] years) from the German/Austrian diabetes patient follow-up registry (DPV) were studied. A comorbid diagnosis and/or specific treatment of mental disorder was documented in 3,158 (6.5%) patients: attention-deficit hyperactivity disorder (ADHD), n = 1,352; depression, n = 692; eating disorders, n = 395; needle phobia, n = 319; anxiety/obsessive compulsive disorder (OCD), n = 231; and psychosis and/or neuroleptic medication, n = 169. Multivariable logistic regression with age, sex, diabetes duration, and migration background as independent variables was used to compare groups.
Results:
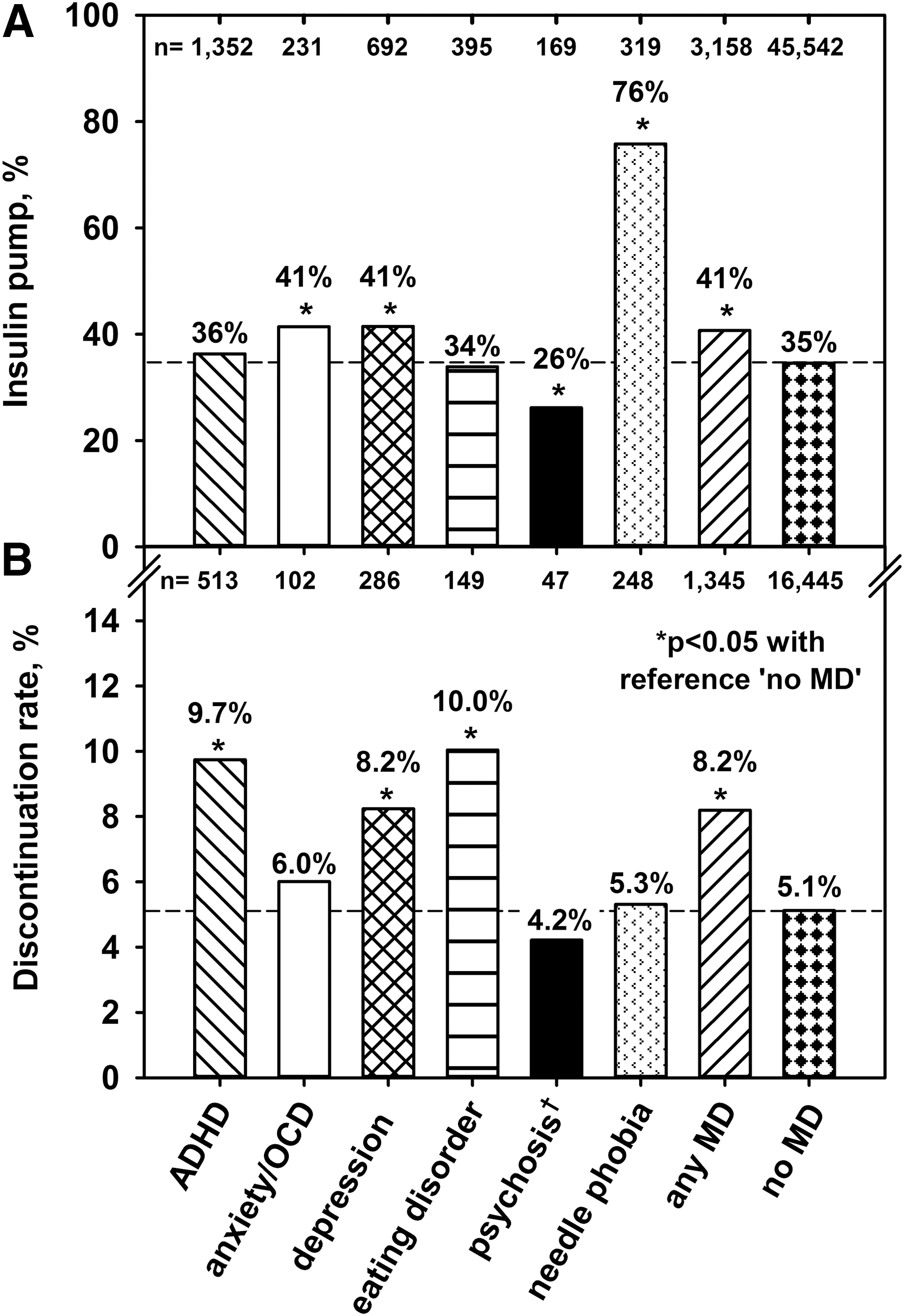
After adjustment for confounders, use of CSII was more common in patients with depression (41.5%), anxiety/OCD (41.4%), or needle phobia (75.8%) compared with patients without mental disorders (34.6%) (each P < 0.05). By contrast, psychotic patients (26.2%, P < 0.05) used CSII less often, and patients with ADHD (36.3%) or eating disorders (33.9%) used it with a similar frequency. Compared with patients without mental disorders (5.1%), the rate of CSII discontinuation was higher in patients with ADHD (9.7%), depression (8.2%), or eating disorders (10.0%) (P < 0.05, respectively) but similar in patients with anxiety/OCD (6.0%), psychosis (4.2%), or needle phobia (5.3%).
Conclusions:
In routine diabetes care, CSII use and discontinuation vary widely among T1D patients with mental disorders and indicate clear differences from the latest recommendations.
Introduction
P
In their latest consensus statement published in 2014, the expert committee on insulin pump management of the American Association of Clinical Endocrinologists considered patients with a history of a serious psychiatric or psychological condition such as psychosis, depression, or severe anxiety as not being good candidates for CSII. 4 As the literature on the use of CSII in these patients is rather scarce, the recommendation is consensus-based, and the reasons remain largely unclear. One key issue is the ability to safely use an insulin pump, which may be compromised in patients with severe mental illnesses. 4 Furthermore, the risk of suicide, manipulation, or insufficient coping with complex electronic devices may deter physicians from using CSII in patients with mental disorders. As consensus statements or guidelines are also a basis for reimbursement decisions, patients with mental disorders may be disadvantaged, although evidence against the use of insulin pumps is limited, and no systematic review exists. Downloading the pump memory could be a potential advantage to detect manipulation and causes for poor glycemic control.
To study the use and discontinuation of insulin pumps in daily routine care, we analyzed a large cohort of 48,700 pediatric and young adult T1D patients with or without clinically recognized comorbid mental disorders.
Materials and Methods
Between 2005 and 2013, 48,700 insulin-treated T1D patients between 5 and 30 years of age were documented by 387 specialized diabetes clinics in the multicenter, standardized, prospective German/Austrian diabetes patient follow-up registry, DPV. The population-based database covers currently up to 90% of pediatric and young adult T1D patients in Germany and Austria. It comprises anonymized information on each patient's demographics, diabetes onset, therapy regimen, and comorbidities. Further details on the DPV structure have been described recently. 5 –7 The DPV Initiative has been approved by the Ethics Committee of Ulm University, Ulm, Germany, as well as the anonymized data acquisition by the local review board of each participating clinic.
To select patients with comorbid mental disorders, the registry was searched for a diagnosis and/or where applicable for specific pharmacological treatment of a mental disorder by using International Statistical Classification of Diseases and Related Health Problems-10 codes (e.g., for ADHD, “F90.-”) and Diagnostic and Statistical Manual of Mental Disorders-IV and Diagnostic and Statistical Manual of Mental Disorders-5 criteria (e.g., “314.01”), as well as specific search terms (e.g., “attention deficit,” “rubifen”). The method was successfully applied in previous studies on comorbid depression, eating disorders, or antipsychotic medication in diabetes patients using DPV data. 5 –7 DPV is the largest real-life database with documented clinical diagnoses of specific psychiatric comorbidities in T1D patients available for Germany and Austria.
This research focuses on the following mental disorders: (1) ADHD, (2) depression, (3) eating disorders, (4) needle phobia, (5) anxiety/obsessive compulsive disorder (OCD), and (6) psychosis/neuroleptic medication. The most recent treatment year was used to study each patient's demographics. Multiple datasets per patient were aggregated using the median for quantitative parameters. If the patient or at least one parent was born outside Germany/Austria, this was classified as migration background. The use of CSII at least once was defined as insulin pump treatment. Pump treatment was managed by both the professional diabetes team and the patients or their parents/legal representatives. To analyze the rate of CSII discontinuation, all patients who started pump therapy were included and followed up. In the present study, 95.5% of the 17,790 pump-treated patients had follow-up visits after CSII initiation, with a median [interquartile range] duration of follow-up of 4.1 [1.9–6.4] years. Pump-treated patients with no additional visit after CSII initiation (n = 796) were counted as current pump users. The decision to discontinue CSII was made by physicians as well as patients.
SAS version 9.4 software (SAS Institute, Cary, NC) was applied for statistical analysis. Descriptive statistics are given as medians with quartiles, or as proportions. The Kruskal–Wallis test was used to compare continuous outcomes, and the χ2 test was used for dichotomous outcomes. Bonferroni's stepdown correction (the Holm method) was applied to adjust P values for multiple testing.
To correct for potential confounders, multivariable logistic regression modeling was implemented for group comparisons as detailed elsewhere. 5 In brief, the use or discontinuation of CSII was entered as a dependent variable in the model. Independent variables were age, sex, diabetes duration, and migration background. Age was categorized in four groups (<13 years, n = 15,210; 13 to <15 years, n = 6,853; 15 to <18 years, n = 16,138; and ≥18 years, n = 10,499), and diabetes duration was divided as <2 years (n = 11,310) and ≥2 years (n = 37,390). Significance was set at a two-tailed P < 0.05.
Results
Clinically recognized mental disorders were documented in 6.5% of the eligible T1D patients. Of these, 2.8% had ADHD, 1.4% had depression, 0.8% had eating disorders, 0.7% had needle phobia, 0.5% had anxiety/OCD, and 0.3% had psychosis and/or used neuroleptic medication (Table 1). In T1D with mental disorders, a male preponderance was observed (Table 1) because of the higher proportion of male subjects with ADHD compared with females (4.4% vs. 1.1%, P < 0.001). As expected, eating disorders were more common in females than in males (Table 1). Compared with patients without mental disorders, body mass index z-score was higher in T1D with depression or psychosis/neuroleptic medication but lower in T1D with ADHD (Table 1). Overall, patients with mental disorders were older and had longer diabetes duration than patients without mental disorders (Table 1). Further baseline characteristics separated by type of mental disorder are summarized in Table 1.
Data are unadjusted medians with quartiles or proportions. Comparisons were made (1) between patients with or without mental disorder (MD) and (2) between patients with specific types of MD and no MD. Entries in bold type indicate step-down Bonferroni (Holm method) adjusted P < 0.05.
Includes patients with neuroleptics.
ADHD, attention-deficit hyperactivity disorder; BMI, body mass index; HbA1c, hemoglobin A1c; OCD, obsessive compulsive disorder.
In total, 36.5% of patients were treated with insulin pumps (vs. 63.5% with multiple daily injections [MDI]), with a discontinuation rate of 6.3%. Figure 1 depicts the use and discontinuation of CSII in patients with or without comorbid mental disorders after adjustment for age, sex, diabetes duration, and migration background. In general, patients with mental disorders had a higher frequency of CSII (59.3% MDI) but also an increased rate of discontinuation compared with patients with no mental disorders (Fig. 1). As expected, insulin pump therapy was most frequent in patients with needle phobia (Fig. 1A). Moreover, CSII was more common in T1D with depression or anxiety/OCD than in patients without mental disorders (Fig. 1A). Patients with psychosis/neuroleptic medication used insulin pumps less often, and patients with ADHD or eating disorders used them to a similar extent, compared with T1D patients without mental disorders (Fig. 1A). In terms of CSII discontinuation, patients with ADHD, depression, or eating disorders had a higher rate compared with patients without mental illnesses (Fig. 1B). By contrast, a comparable rate of discontinuation was observed among the other groups (Fig. 1B).
Discussion
The present real-life clinical data on the use and discontinuation of insulin pumps in patients with mental health comorbidities indicate a large heterogeneity and clear differences from the current American Association of Clinical Endocrinologists/American College of Endocrinologists consensus statement on CSII management published in 2014. 4 In addition, the comparatively low rates of mental disorders observed among pediatric and young adult T1D patients studied probably point to difficulties in recognizing or documenting mental disorders in routine diabetes care.
Contrary to the consensus recommendation that patients with severe anxiety or depression are not good candidates for insulin pumps, 4 a higher frequency of CSII was observed among these patients in routine care. Recent findings report also a higher prevalence of depression and anxiety in adult CSII users compared with T1D controls, 8 as well as more psychological disturbances like depression, anxiety, or OCD in females on CSII compared with those using MDI. 9 It was suspected that a higher level of psychopathology may be associated with unsatisfactory glucose control that could not be managed using conventional injection therapy and thereby lead to CSII treatment. 9 As needle phobia is a common indication for CSII and a higher fear of needles has been reported in pump users, 10 it was not surprising that these patients had the highest rate of CSII. Moreover, this high rate of CSII in needle phobia patients explains to a large extent the overall higher frequency of CSII in the mental disorder group. In line with a small previous study suggesting that CSII is feasible in girls with T1D and eating disorders, 11 our data indicate a similar frequency of CSII in patients with eating disorders compared with patients without mental disorders. As recommended by the Insulin Pump Management Expert Committee, 4 CSII was less common in T1D with psychosis/neuroleptic medication but was still used in a considerable number of patients.
Occurrence or deterioration of a mental disorder, as well as insufficient metabolic control during CSII, may lead to discontinuation of insulin pumps. In particular, patients with ADHD, depression, or eating disorders had an approximately twofold higher rate of discontinuation compared with patients without mental disorders. A small study found that depressive symptoms precede the switch from CSII to MDI. 12 Moreover, patients with anxiety were reported to do well on CSII, whereas patients with depression had worse results. 8 Although a reduction in disordered eating behavior was observed after CSII initiation in a small cohort, 13 our data indicate a high rate of discontinuing CSII in patients with severe clinically recognized eating disorders.
Compared with data based on specifically designed screening studies for mental disorders, the rate of psychiatric comorbidities clinically recognized among the T1D population studied is low. However, a recent registry-based Swedish study 2 in T1D patients of similar age reported a comparable frequency of recognized mental disorders to our study (8.3% vs. 6.5%), and in the representative German KiGGS study 5.6% of children and adolescents from the general population used mental health care. 14 Thereby, mental disorders are probably overlooked in routine diabetes care. Moreover, an entry of a psychiatric diagnosis in the DPV registry is possibly made with caution as this may negatively impact employment and insurance.
In summary, routine screening for mental comorbidities as recommended by the American Diabetes Association 15 is desirable in pediatric and young adult T1D patients because a clinically recognized mental disorder has implications on CSII treatment. As the majority of CSII patients with mental disorders do not discontinue pump use, the general consensus recommendation against CSII use in these patients should be reconsidered, and further investigations related to safety and efficacy of CSII in this group are needed. Up to now, the decision to initiate or discontinue CSII in T1D with mental disorders should be made carefully on an individual basis and should involve diabetologists as well as psychological or psychiatric specialists.
Footnotes
Acknowledgments
Financial support for the present study was provided by the Federal Ministry of Education and Research within the German Competence Network for Diabetes Mellitus (grant 01GI1106), which has been integrated into the German Center for Diabetes Research as of January 2015. Further financial support was provided by the German Diabetes Association and the European Foundation for the Study of Diabetes. The authors thank E. Bollow for performing statistical analysis. Furthermore, they wish to express their gratitude to all participating centers of the DPV Initiative for contributing data to the present study (a detailed list is available at
Author Disclosure Statement
S.v.S. reported advisory activity for Medtronic, received speaking fees and reimbursement of travel costs from Bayer Healthcare, Medtronic, Novo Nordisk, and Roche, and obtained three insulin pumps for a research project from Medtronic free of charge. N.P, C.B., M.B., G.B., A.G., H.H., M.M., J.M., P.L.P., M.T., and R.W.H. declare no competing financial interests exist.