
Abstract
Background:
Testing for beta cell autoantibodies is used for wide-scale identification of early stages of type 1 diabetes. This requires suitable screening assays. We aimed to establish screening that utilized a first step assay (3 Screen) able to detect autoantibodies to the target antigens glutamic acid decarboxylase-65 (GAD), insulinoma-associated antigen 2 (IA-2), and zinc transporter 8 (ZnT8) to identify children positive for multiple beta cell autoantibodies.
Methods:
An ELISA format was used where plates were coated with a mixture of recombinant GAD, IA-2, and ZnT8325W/R-dimer molecules. The performance was determined in venous blood from 686 first-degree relatives of patients with type 1 diabetes, and 200 patients at onset of type 1 diabetes, and applied as a screening assay in capillary blood from 33,639 general population children.
Results:
The 3 Screen assay sensitivity for detecting autoantibody-positive patients at onset of type 1 diabetes was similar to that achieved by separate radiobinding assays (RBAs) for antibodies to GAD, IA-2, and ZnT8. Results in venous and capillary serum were correlated (R = 0.987). At a threshold corresponding to the 98th centile (29.1 U/mL) of all 33,639 capillary samples, the 3 Screen was positive in 123 samples with two or more RBA-positive antibodies to insulin, GAD, IA-2, or ZnT8, 146 with one antibody, and 479 that were RBA negative for beta cell autoantibodies.
Conclusion:
A 3 Screen ELISA was developed that was suitable for first step screening of multiple beta cell autoantibodies in capillary blood.
Introduction
T
Current assays for the detection of beta cell autoantibodies are sensitive, specific, and standardized.
3
–6
In their current format, they are not applicable to population-wide screening, as they are expensive and labor intensive. Furthermore, there is limited experience of using these assays with capillary blood.
7
–9
We reasoned that to identify children positive for at least two (i.e., multiple) of the autoantibodies to the target antigens glutamic acid decarboxylase-65 (GAD), insulinoma-associated antigen 2 (IA-2), zinc transporter 8 (ZnT8), and insulin, a first step screening assay would be suitable if it was able to detect at least three of these four autoantibodies. This would allow selection of a minority of samples for second line testing in the four individual autoantibody assays. If the screening assay was sufficiently specific and sensitive, it could prove a cost-effective strategy for population testing. A commercial assay for combined measuring of GAD and IA-2 autoantibodies is available (2 Screen ICA™ ELISA;
In this study, we aimed to determine the sensitivity and specificity of the 3 Screen assay as a first line test to identify children with multiple beta cell autoantibodies. We tested the overall performance of the assay in children with new-onset diabetes, children with a first degree relative with type 1 diabetes, and applied the 3 Screen to the Fr1da screening of children from the general population.
Materials and Methods
Study population
The specificity and sensitivity of the 3 Screen ELISA to detect GAD, IA-2, and ZnT8 autoantibodies were determined using venous serum samples from 686 beta cell autoantibody-negative first degree relatives of patients with type 1 diabetes participating in the BABYDIAB and TeenDiab studies (median age 3.1 years; IQR = 2.1–4.9 years), and in autoantibody-negative (n = 79) and autoantibody-positive (n = 121) patients at onset of type 1 diabetes from the DiMelli study (median age 12.3 years; IQR = 8.4–14.9 years). 11 –13 Additional capillary serum samples were obtained from 27 children for comparison of venous and capillary serum measurements.
The 3 Screen ELISA was then applied to a general population screening of children aged 2–5 years in the Fr1da study. 1 At the time of analysis, a total of 33,639 children had been tested. Screening was performed in capillary blood serum samples. For the first 10,000 samples tested, all those with 3 Screen ELISA values >10 U/mL were tested in the single radiobinding assays (RBAs) for autoantibodies to GAD, IA-2, ZnT8, and insulin. The threshold for testing in the single RBAs was subsequently adjusted to 20 U/mL (U/mL are arbitrary laboratory units/mL).
The BABYDIAB and TeenDiab studies were approved by the ethical committee of Bayerische Landesarztekammer (No. 95357), Technical University Munich (No. 2149/08), and Medizinische Hochschule Hannover (No. 5644), respectively. 11,12 The DiMelli study was approved by the ethical committee of Bavaria, Germany (Bayerische Landesarztekammer, No. 08043). 13 The Fr1da study was approved by the ethics committee of Technische Universität München (No. 70/14).
Capillary blood draw
In the Fr1da study, capillary blood samples (200 μL in Microvette® 200 Z tubes) were collected by primary care pediatricians and shipped to our institute after storage of up to 5 days in a refrigerator. Upon receipt, they were centrifuged at 3000 rpm to obtain serum. Signs of hemolysis were recorded. The serum samples were stored at −20°C and tested within 1 week after receipt.
Radiobinding assays
Autoantibodies to GAD (GADA), IA-2 (IA-2A), ZnT8 (ZnT8A), and insulin (IAA) were determined using RBAs as previously described. 6,11,14 The upper limit of normal for each assay corresponded to the 99th percentile of 836 control children. Autoantibody assays were evaluated by the Diabetes Antibody Standardization Program, and performances are shown as laboratory 121 in published reports. 3 –5
3 Screen ELISA
ELISA plates were supplied coated with a mixture of highly purified recombinant GAD, IA-2, and ZnT8 (325 W/R dimer molecule). Biotin labeled GAD, IA-2, and ZnT8 were provided combined together in freeze-dried vials. In the ELISA, 25 μL of serum was incubated in the coated wells overnight at 2°C–8°C followed by aspiration, washing, and incubation with 100 μL of reconstituted antigen–biotin mixture at 2°C–8°C for 1 h. The assay was completed with incubations with streptavidin–peroxidase followed by tetramethylbenzidine and a stop solution. Reagents were provided in a kit format by RSR. Kit calibrators and controls were included in each assay. The ODs at 450 nm were measured. High concentrations of autoantibodies (>400 U/mL) were quantitated by measuring the ODs at 405 nm. All screening was performed in single wells.
Statistical analysis
Distributions of 3 Screen antibody values were compared between nonhemolyzed and hemolyzed samples by the Mann–Whitney U test.
Results
Sensitivity of 3 Screen in children with new-onset diabetes
The 98th and 99th centiles of 3 Screen ELISA measurements in venous serum samples from 686 islet autoantibody-negative first degree relatives of patients with type 1 diabetes were 19 and 43 U/mL, respectively (Fig. 1). All but 2 of 99 GADA, IA-2A, and/or ZnT8A-positive patients had 3 Screen ELISA values above 43 U/mL. One of these patients was positive for IA-2A and the other for ZnT8A. In addition, 12 (15.2%) of 79 beta cell autoantibody RBA-negative patients and 13 (40.6%) of 32 patients who were insulin antibody positive but negative in RBAs for other beta cell autoantibodies had 3 Screen ELISA values above 43 U/mL. Thus, overall, the sensitivity of the 3 Screen ELISA for detecting autoantibody-positive patients at onset of type 1 diabetes was not inferior to separate RBAs for GADA, IA-2A, and ZnT8A.
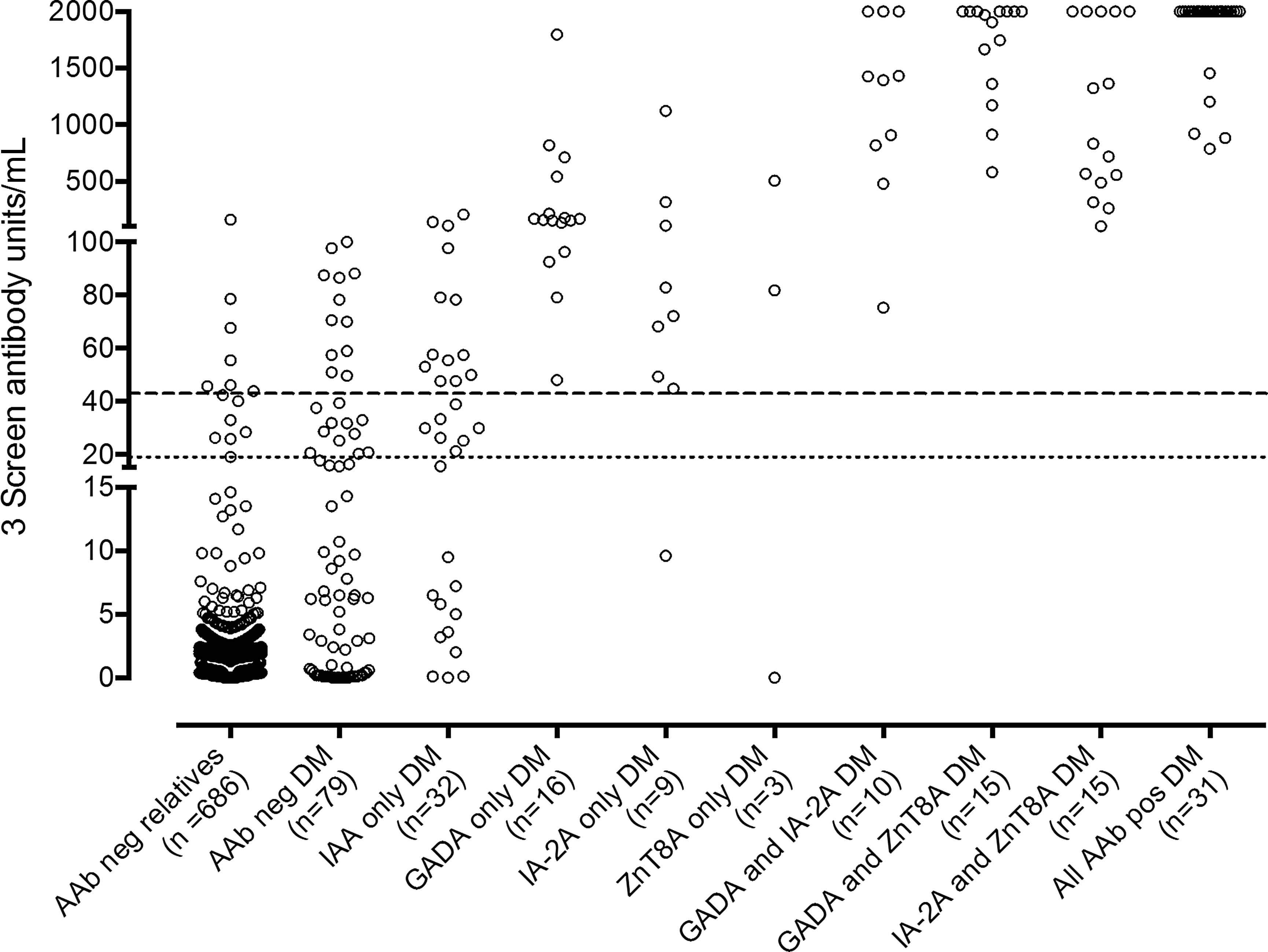
Values of 3 Screen ELISA (y-axis) in venous serum samples of children with new-onset diabetes (DM) relative to positivity in single RBA (x-axis). The 98th and 99th centiles (dashed lines) in the 3 Screen ELISA were calculated from measurements in 686 islet autoantibody-negative (AAb neg) first degree relatives of patients with type 1 diabetes (left). AAb, autoantibody; RBA, radiobinding assays.
Application of 3 Screen to general population screening in the Fr1da study
The Fr1da study uses capillary blood for first autoantibody measurements. There was a high correlation between venous and capillary serum measurements (R = 0.987; P < 0.0001) (Fig. 2). None of the samples used for the comparison had visible signs of hemolysis. However, around 30% of Fr1da capillary samples had visible hemolysis. The distribution of 3 Screen ELISA values was shifted to slightly higher values in the 9961 samples with visible hemolysis than the 23,678 samples without hemolysis (P < 0.0001; Fig. 3A).
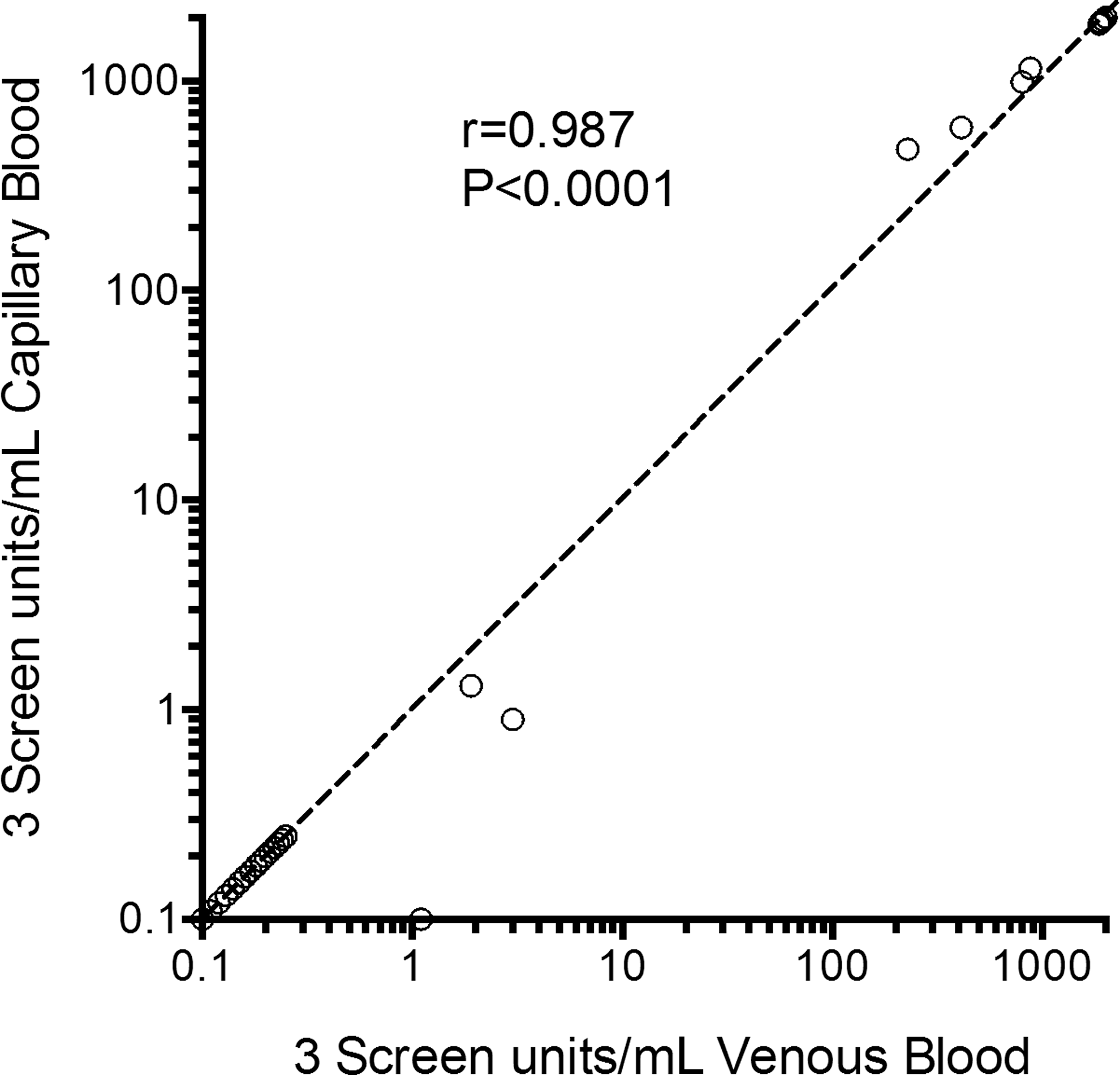
Correlation of venous (x-axis) and capillary (y-axis) serum 3 Screen ELISA measurements.

3 Screen ELISA measurements in large-scale testing of capillary blood samples.
The 97.5th, 98th, 98.5th, and 99th centile corresponded to values of 16.6, 29.1, 45.8, and 82.6 U/mL for all 33,639 capillary samples. The thresholds of 10 U/mL (used to select samples for single autoantibody testing in the first 10,000 samples screened) and 20 U/mL (subsequently used to select samples for single autoantibody testing) corresponded to the 96.9th centile and 97.7th centile, respectively. A total of 1162 samples above these thresholds were measured with single autoantibody RBAs, including 602 nonhemolyzed and 557 hemolyzed samples (Table 1). Of those, 208 (34.2%) without hemolysis and 104 (18.7%) with hemolysis were confirmed positive for at least one autoantibody in the single RBAs (Fig. 3B, C), and 90 (14.9%) and 33 (5.9%) with multiple beta cell autoantibodies. In comparison, 409 capillary blood samples with 3 Screen ELISA values below 10 U/mL were tested in the single RBAs and none was positive for multiple beta cell autoantibodies, 4 (1%) had GAD autoantibodies above the 99th centile threshold, none had IA-2 autoantibodies above the 99th centile threshold, and 4 (1%) had ZnT8 autoantibodies above the 99th centile threshold.
Samples positive for GADA or IA-2A or ZnT8A.
Samples positive for IAA and one of the antibodies as above.
Samples positive for two AAb of GADA, IA-2A, or ZnT8A.
Samples positive for three AAb of IAA, GADA, IA-2A, or ZnT8A.
Samples positive for IAA, GADA, IA-2A, ZnT8A.
AAb, autoantibody; GADA, glutamic acid decarboxylase autoantibodies; IA-2A, insulinoma-associated antigen 2 autoantibodies; IAA, insulin autoantibodies; RBA, radiobinding assays; ZnT8-A, zinc transporter 8 autoantibodies.
Since the 3 Screen ELISA was used as a screening test, it was important that a threshold was selected to identify all multiple beta cell autoantibody-positive children. For both the nonhemolyzed (Fig. 3B) and hemolyzed (Fig. 3C) samples, a threshold corresponding to the 98th centile of all 33,639 samples (29.1 U/mL) was sufficient to identify all 90 (100%) multiple beta cell autoantibody-positive nonhemolyzed samples and 33 (100%) multiple beta cell autoantibody-positive hemolyzed samples found using the 10 and 20 U/mL thresholds. In addition, 3 Screen ELISA values above 29.1 U/mL were obtained in 58 (93.6%) of 62 nonhemolyzed and 30 (88.2%) of 34 hemolyzed capillary samples with single RBA-positive autoantibodies to GAD, IA-2, or ZnT8 that had been found with the lower 3 Screen thresholds. The 3 Screen ELISA values above 29.1 U/mL were observed in 58 (62.4%) of 93 capillary samples with IAA only (45 of 56 nonhemolyzed and 13 of 37 hemolyzed samples) and in 479 (56.5%) of 847 samples that did not have any beta cell antibodies by RBA (249 of 394 nonhemolyzed and 230 of 453 hemolyzed samples) (Table 1). Thus, at a threshold at which all of the known multiple beta cell autoantibody-positive children would be identified, the 3 Screen ELISA also identified 625 (1.86%) of 33,506 samples without multiple beta cell autoantibodies, of which 146 had one RBA-positive beta cell autoantibody (Table 1).
Discussion
We report a new 3 Screen ELISA for combined detection of autoantibodies against GAD, IA-2, and ZnT8. When applied to beta cell autoantibody-positive and autoantibody-negative patients with new-onset diabetes, the assay identified the majority of patients who had any of these autoantibodies determined positive by RBA. Importantly, at a threshold that corresponded to the 98th centile of over 30,000 capillary blood samples from children of the general population, the 3 Screen ELISA was sufficiently sensitive to recognize children with multiple beta cell autoantibodies, including children with IAA and one other antibody against GAD, IA-2, or ZnT8, and the majority of children with single GAD, IA-2, or ZnT8 autoantibodies.
The 3 Screen ELISA had several positive aspects. First, it was easy to operate and facilitated the high-throughput first line screening in the model Fr1da project. Second, it had similar performance in venous blood and capillary blood. The slight difference observed in the 99th centile determined in venous blood (43 U/mL) and capillary blood (82.6 U/mL) was likely due to the selection of RBA beta cell autoantibody-negative samples for the measurements in venous blood and the much lower number of venous blood samples tested. Nevertheless, it remains important to determine new thresholds if other sample types such as dried blood spot samples are used.
The assay also had a number of limitations. It was affected by hemolysis in the low range. This did not affect its sensitivity in identifying multiple beta cell autoantibody-positive children, but, nevertheless, slightly decreased specificity. Hemolysis was frequent in capillary samples obtained in the Fr1da study, something that may be unavoidable when collecting and shipping capillary blood on a daily basis. We have previously shown that also the IAA assay in capillary blood is affected by hemolysis. 1 We did not find differences between venous and capillary blood, but only tested a small number of samples. Assay performance may also be affected by lipemic or icteric samples. Improvements in sample processing or collection (e.g., dried blood spots) and assay development may overcome this shortcoming through hemolysis in the future. 15 –17
A second limitation is that we had to use a threshold corresponding to the 98th centile to achieve maximum sensitivity. Although this is similar or even higher than that which is obtained with other screening approaches in the general population, 18 –20 around two-thirds of the samples transferred to single RBA measurements were negative for all autoantibodies. We cannot exclude that some of these were true positives that were missed by the RBAs and could have been detected if ELISA format assays were also used for second line testing. Of interest, the 3 Screen ELISA was able to detect GAD, IA-2, and ZnT8 RBA autoantibody-negative children with new-onset diabetes, suggesting that it may have increased sensitivity compared to the RBA. Since not all capillary blood samples were tested in the single RBAs, it is also possible that multiple beta cell autoantibody children were missed in the 3 Screen assay. Discrepancies between the ELISA format and RBA assays for beta cell autoantibodies are known 21 and need further investigation. A logistic limitation was that, in its current format, the 3 Screen assay required 25 μL serum per well. In the Fr1da study, the majority of samples had sufficient blood volume to perform the 3 Screen assay and follow-up measurements. 1 However, this may become a limitation if other autoantibodies or other measurements are required. Finally, unlike otherwise reported assays, 17 the 3 Screen ELISA does not distinguish which of the three beta cell autoantibodies are present, nor does it detect insulin autoantibodies. However, such other assays even though they show promise have not been evaluated in a setting such as Fr1da to determine how they compare with 3 Screen.
In conclusion, we demonstrated that our strategy to use the 3 Screen ELISA for screening of beta cell autoantibodies in capillary blood in the Fr1da study was effective and identified children with multiple beta cell autoantibodies.
Footnotes
Acknowledgments
The Fr1da study is supported by grants from the LifeScience-Stiftung, JDRF (1-SRA-2014-310-M-R), the Bavarian State Ministry of Health and Care (Gesund.Leben.Bayern, LP00228), Deutsche Diabetes-Stiftung, Landesverband Bayern der Betriebskrankenkassen, B. Braun-Stiftung (BBST-D-15-00016), and Deutsche Diabetes-Hilfe. The work was supported by grants from the German Federal Ministry of Education and Research to the German Center for Diabetes Research (DZD e.V.).
Authors' Contributions
A.G.Z., E.B., and P.A. designed the study, researched the data, and wrote the article. F.H., M.S., K.W., S.W., S.L., C.M., C.G., S.R., A.B., S.Z., and C.W. researched the data and contributed to the writing of the article. E.B. and P.A. did the statistical analysis. M.A., R.C., M.P., J.F., and B.R.S. researched the data and contributed to the writing of the article. All authors reviewed the article for intellectual content.
Author Disclosure Statement
A.G.Z., F.H., M.S., K.W., S.W., S.L., C.M., C.G., S.R., A.B., S.Z., C.W., E.B., and P.A. have no competing financial interests. M.A., R.C., M.P., J.F., and B.R.S. are employees of RSR Ltd., a developer and manufacturer of diagnostic kits, including kits for measuring diabetes-associated autoantibodies.