
Abstract
Background:
Hypoglycemia is a major concern in older adults with type 1 diabetes (T1D) and there is limited knowledge in this population. We examined data from 199 adults, ≥60 years of age, who participated in a T1D Exchange study assessing factors associated with severe hypoglycemia (SH) in older adults with T1D: 100 with SH in the prior year and 99 with no SH in prior 3 years (mean age 68; mean diabetes duration 40 years; 47% female; 92% non-Hispanic white). Hypoglycemia was assessed with up to 14 days of blinded continuous glucose monitoring (CGM). Linear regression models were performed to assess the association between biochemical hypoglycemia [defined as percentage of time below specific cutoffs (<70/60/50 mg/dL)] and various factors.
Results:
Overall, participants had CGM values <70 mg/dL for a median of 91 min per day. On 53% of days, glucose levels continuously were <70 mg/dL for ≥20 min. Hypoglycemia was found to be strongly associated with glucose variability (r = 0.76; P < 0.001). Time spent in hypoglycemia was greater in those who were younger (P = 0.004), had shorter diabetes duration (P = 0.008), lower HbA1c (P < 0.001), and undetectable C-peptide (P = 0.001), but did not differ by insulin method, education level, number of blood glucose checks per day, cognition, activities of daily living, or fear of hypoglycemia.
Innovation:
This study adds valuable data on the frequency of hypoglycemia in older adults with T1D.
Conclusion:
Future studies need to focus on how to prevent hypoglycemia in this vulnerable population of older adults with long-standing T1D.
Introduction
H
There is limited knowledge regarding hypoglycemia in older adults with long-standing T1D, an understudied population. T1D Exchange data indicate that one or more hypoglycemic events resulting in seizure or loss of consciousness were reported within the prior year by 18.6% of participants with ≥40-year duration of T1D. 3 Recent reports have identified a high frequency of insulin-induced hypoglycemia, resulting in emergency room visits 4 and hospitalizations 5 in Medicare patients with diabetes. However, the studies do not differentiate type 1 from type 2 diabetes, so the actual frequency and costs of this acute complication for older adults with T1D are not known. Despite recommendations to treat older adults with T1D to more conservative glycemic targets, higher HbA1c levels do not protect from severe hypoglycemia (SH). 3
To better understand factors associated with SH in older adults, the T1D Exchange conducted a case–control study of individuals ≥60 years old with T1D for ≥20 years comparing individuals who had at least one severe hypoglycemic event in the prior 12 months (cases) with controls who had no SH in the prior 3 years. No difference was found between the cases and controls in HbA1c levels, but substantially more frequent hypoglycemia unawareness and a trend toward more biochemical hypoglycemia measured with blinded continuous glucose monitoring (CGM) in cases than controls were found. 6 What was noteworthy was the amount of hypoglycemia per day in both cases and controls.
In this article, we combine cases and controls to further describe CGM-measured hypoglycemia in this cohort of older adults with long-standing T1D and assess the association of various factors with the frequency of hypoglycemia.
Methods
The study was conducted at 18 diabetes centers in the T1D Exchange Clinic Network. 7 The protocol was approved by the respective multiple institutional review boards, and study participants provided written informed consent. Study methods were described previously 6 and only pertinent aspects are detailed here.
Participants were non-CGM users who had a clinical diagnosis of T1D, were ≥60 years old, had diabetes duration ≥20 years, and did not have chronic kidney disease stage 4 or 5 (glomerular filtration rate <30 mL/min/1.73 m2 [if known]), moderate or advanced dementia, or a history of pancreatic transplant. There were 101 participants who had at least one severe hypoglycemic event (defined as an event requiring assistance of another person, as a result of altered consciousness or confusion, to administer carbohydrate, glucagon, or other resuscitative actions) in the prior 12 months and 100 participants, matched on age, who had no SH in the prior 3 years.
A CGM sensor (Dexcom™ SEVEN® PLUS; Dexcom, Inc., San Diego, CA) was used to collect glucose data for up to 14 days. This sensor measures interstitial glucose concentrations every 5 min for up to 7 days. The device was set such that the participant could not see the glucose measurements (referred to as blinded). After 7 days, the participant returned to the clinic to have the sensor replaced.
CGM data were obtained and analyzable from 199 of the 201 participants (median of 286 h of glucose data). CGM hypoglycemic metrics were computed overall (24-h day) and separately for daytime (6 a.m. to midnight) and nighttime (midnight to 6 a.m.). The calculation of proportion of days/nights with at least one CGM hypoglycemic event (defined as at least 20 min with CGM glucose values <70/60/50 mg/dL) was limited to participants with at least 7 full days/nights of data. The 24-h period and 18-h daytime period both required a minimum of 6 h of data to be considered an analyzable day and the 6-h night required a minimum of 3 h of data to be considered an analyzable night. Glucose variability was assessed with the coefficient of variation (standard deviation/mean of glucose).
Overall cognition (Montreal Cognitive Assessment [MoCA] 8 ) and instrumental activities of daily living (Functional Activities Questionnaire [FAQ] 9 ) were assessed. Diabetes-related questionnaires included diabetes numeracy (Diabetes Numeracy Test-15 question [DNT] 10 ), hypoglycemia unawareness (Clarke Hypoglycemia Unawareness Questionnaire 11 ), hypoglycemia fear (Hypoglycemia Fear Survey 12 ), and hyperglycemia fear (Preferring Hypoglycemia Scale [W.H. Polonsky, personal communication]). Measurements of HbA1c and random C-peptide were performed at a central laboratory where the minimum detectable level was 0.017 nmol/L.
Linear regression models were performed to assess the association between biochemical hypoglycemia [defined as percentage of time below specific cutoffs (<70/60/50 mg/dL)] and various factors. The model assessing the association between HbA1c and hypoglycemia was adjusted for age, diabetes duration, average number of blood glucose checks per day, socioeconomic status, and pump use. The model assessing the association between C-peptide level and hypoglycemia was adjusted for diabetes duration and diagnosis age. All other clinical and diabetes factors were first assessed with univariate analyses. Due to a non-normal distribution of biochemical hypoglycemia, a rank transformation (van der Waerden scores) was used in the models. Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC) and all P-values are two-sided. In view of the multiple comparisons, only P-values ≤0.01 were considered statistically significant.
Results
The 199 participants were 47% female and 92% white; mean age was 68.3 ± 6.2 years and diabetes duration 39.9 ± 11.7 years. Additional characteristics are shown in Table 1.
SD, standard deviation.
CGM-measured glucose concentrations were <70 mg/dL for a median of 91 min per 24-h day (interquartile range 40 − 152), <60 mg/dL for 55 (21 − 102) min per day, and <50 mg/dL for 31 (9 − 65) min per day. Median time below 70 mg/dL appeared slightly higher overnight (12 midnight to 6 a.m.) than during the day (6 a.m. to 12 midnight), but median time <60 and <50 mg/dL was similar between nighttime and daytime (Table 2).
Unless otherwise indicated, all values are medians (25th, 75th percentile).
To convert to minutes per 24 h, multiply percentage of time by 1440 (24 h/day × 60 min/h).
Event defined as at least 20 min below 60 mg/dL.
Additional CGM data missing for three participants due to not having the minimum requirement of at least 7 full days of data (at least 6 full hours per 24-h day).
To convert to minutes per daytime period, multiply percentage of time by 1080 (18 daytime hours/day × 60 min/h).
Additional CGM data missing for six participants due to not having the minimum requirement of at least 7 full days of data (at least 6 full hours per 18-h day).
To convert to minutes per nighttime period, multiply percentage of time by 360 (6 nighttime hours/day × 60 min/h). Additional CGM data missing for six participants due to less than 24 h of nighttime CGM readings available.
Additional CGM data missing for 15 participants due to not having the minimum requirement of at least 7 full nights of data (at least 3 full hours per 6-h night).
CGM, continuous glucose monitoring; hypo, hypoglycemic.
Glucose concentrations were <70 mg/dL continuously for ≥20 min on 53% of 24-h days, <60 mg/dL for ≥20 min on 38%, and <50 mg/dL for ≥20 min on 27% of 24-h days. The percentages of nighttime periods with at least 20 continuous minutes of time <70, <60, and <50 mg/dL were 56%, 41%, and 27%, respectively, and percentages of daytime periods were 57%, 38%, and 29%, respectively.
The amount of hypoglycemia (<70, <60, and <50 mg/dL) varied with HbA1c level (adjusted P ≤ 0.004 for all three hypoglycemia levels, Figs. 1 and 2). As can be seen in the scatter plot, there was a wide range of HbA1c levels for a given amount of hypoglycemia, but when the amount of hypoglycemia exceeded 144 min per day, almost all of the HbA1c levels were below 8.0% and most below 7.0%. Hypoglycemia was found to be strongly associated with glucose variability (r = 0.76; P < 0.001).

Hypoglycemia by HbA1c level.
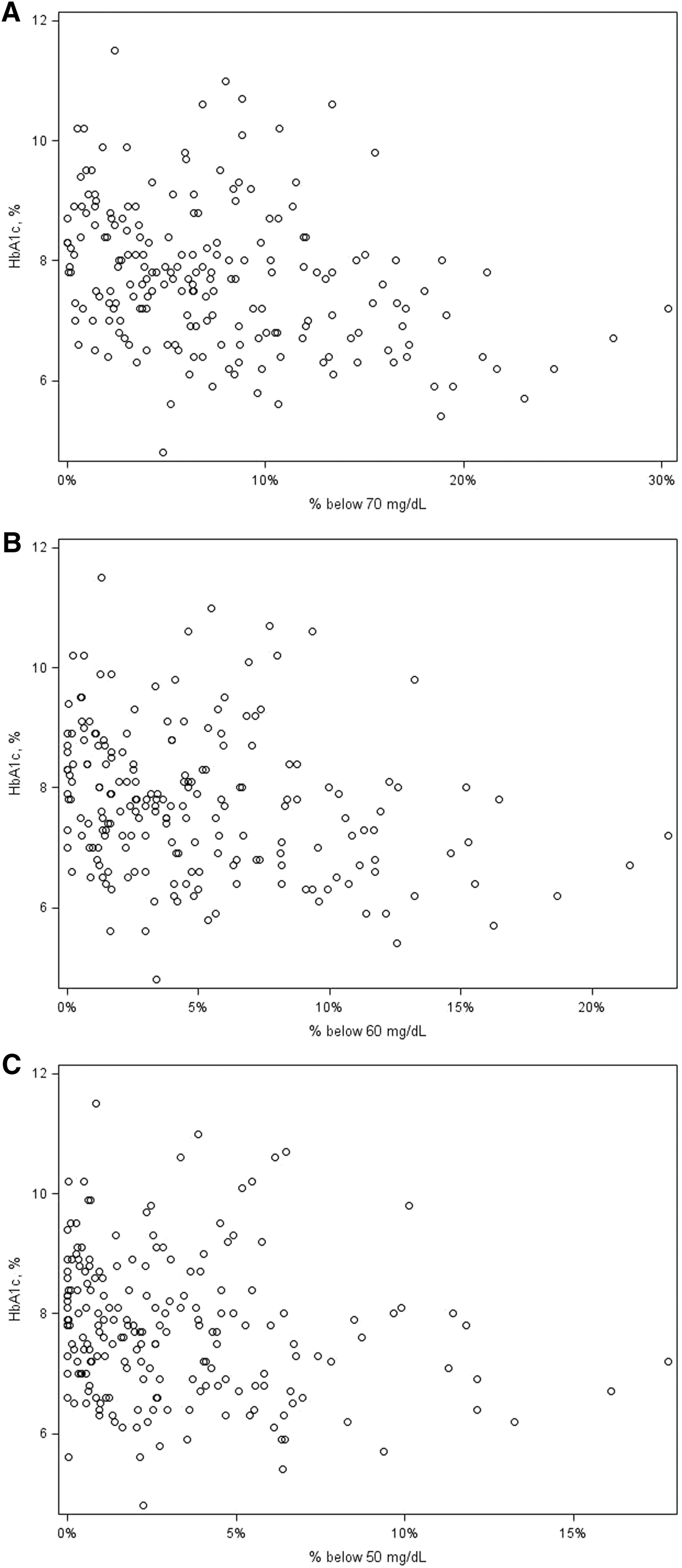
HbA1c and hypoglycemia scatter plots.
In univariate and multivariate analyses, time below 70 mg/dL was inversely associated with age and duration (P = 0.004 and 0.008 in univariate analyses and 0.007 and 0.02 in the multivariate analyses, respectively; recognizing that all participants were at least 60 years old and minimum duration was 20 years), but not significantly associated with any of the other factors evaluated (Table 3). The association with age and duration remained present after adjusting for HbA1c, pump/injection usage, self-monitoring of blood glucose (SMBG) frequency, total daily insulin dose, hypoglycemia unawareness, and detectable C-peptide. Findings were similar for time <60 mg/dL and time <50 mg/dL, although there was more of a trend toward an association between hypoglycemia and female gender at the lower cutoffs (P = 0.03 for <60 mg/dL and P = 0.01 for <50 mg/dL).
Median percentage of time spent below 70 mg/dL from blinded CGM.
Multivariate model included variables with P-value <0.05 in univariate model.
P values were obtained using continuous variables; categories shown for display purposes.
Scoring details: MoCA cognitive test—lower scores indicate reduced capacity; FAQ—higher scores indicate less functional independence; DNT—lower scores represent diminished mathematical skills; Hypoglycemia Fear Survey—higher scores indicate more hypoglycemia fear. Additional scoring details listed in the Supplementary Data available at
DNT, Diabetes Numeracy Test-15 questions; FAQ, Functional Activities Questionnaire; MoCA, Montreal Cognitive Assessment; SMBG, self-monitoring of blood glucose; T1D, type 1 diabetes.
Hypoglycemia was lower among those with detectable C-peptide (<70 mg/dL for a median of 65 min/day; n = 45) versus those with undetectable C-peptide (<70 mg/dL for a median of 98 min/day; n = 152) (adjusted P = 0.001). Results were similar when only including participants with glucose in the range of 70–200 mg/dL (n = 108) at the time of the C-peptide test (data not shown). When assessing meaningful levels of C-peptide (≥0.2 mg/dL), hypoglycemia was lower among those with (<70 mg/dL for a median of 38 min/day; n = 13) versus those without (<70 mg/dL for a median of 92 min/day; n = 184; adjusted P = 0.001) a C-peptide level ≥0.2 mg/dL.
Discussion
This observational study found that about half of older adults with long-standing T1D spend at least an hour and a half a day below 70 mg/dL, with a quarter being below 70 mg/dL for at least 2.5 h a day. The amount of hypoglycemia was lower among those who were older, had longer diabetes duration, higher HbA1c, and detectable C-peptide levels.
The association between hypoglycemia and C-peptide suggests a protective effect from endogenous insulin secretion. While insulin doses were not different between those with and without detectable C-peptide levels (0.5 units/kg/day in both groups), it is plausible that endogenous insulin cushions the hypoglycemic nadirs by being suppressed at the appropriate time.
It should be noted that while the amount of hypoglycemia was higher among those with lower HbA1c levels, mean HbA1c was similar between those who had a severe hypoglycemic event in the prior year (defined as needing assistance of another person) and those who had not had a severe hypoglycemic event in the prior 3 years. 6 This indicates that HbA1c values are not a sensitive predictor of SH, but rather hypoglycemia itself leading to hypoglycemia-associated autonomic failure (HAAF) is a more important risk factor.
We found an inverse relationship between time below 70 mg/dL with age and duration of diabetes. One possible explanation is that some of the younger adults with more hypoglycemia may have higher mortality and thus do not survive to be in the much older age groups. Similarly, these patients could have greater morbidity and enter long-term care facilities, thus no longer being seen at a participating diabetes center. Another possible explanation, while speculative and will need to be reassessed with other populations of the same age and duration of diabetes to determine if it is true rather than a chance finding, is that the younger patients have central nervous system (CNS) adaptation to hypoglycemia (which may be adaptive or maladaptive given the dangers of hypoglycemia), 13 while the older patients do not have this adaptation. Although speculative, it is possible the normal CNS adaptation does not occur in our oldest patients due to neurologic dysfunction that occurs with aging. Our data suggest that this relationship with age and diabetes duration is more important than insulin method of delivery, frequency of SMBG, cognition, instrumental activities of daily living, diabetes numeracy, or even fear of hypoglycemia. Future studies need to address potential mechanisms of this CNS adaptation and potential structural changes, which could be identified radiographically.
Hypoglycemia in people with diabetes in this age group has been documented to result in increased falls, fractures, ER visits, hospitalizations, costs, and reduced quality of life. 14 However, most of the literature focuses on those with type 2 diabetes. Compared with a population of patients with type 2 diabetes, durations of diabetes (and time receiving insulin) tend to be longer and thus we might expect to see different CNS outcomes, but it is difficult to know what they would be.
One limitation of this study is that the vast majority of the sample was Caucasian and highly educated. As such, these results may not generalize to other demographic groups with T1D. Another potential limitation is the CGM device that was used to collect blinded data for this study, the Dexcom 7, is not as accurate as the current Dexcom system, especially at hypoglycemic levels. However, while this may affect the accuracy of individual readings, it is not expected to affect summary statistics over time since higher mean absolute relative differences would result in an equal probability of higher or lower CGM glucose measurements compared with a predefined level, such as 70 mg/dL. Therefore, we do not believe that this had a major influence on the results.
Although we did not find a statistically significant association between hypoglycemia awareness and biochemical hypoglycemia, it is well known that repeated hypoglycemia leads to HAAF. Therefore, the frequency of hypoglycemia in this cohort, while not vastly greater than other adults with T1D, 15 is alarming. Older adults are already at great risk for hypoglycemia unawareness, with 45% of this cohort reporting reduced hypoglycemia awareness. Furthermore, we know that hypoglycemia unawareness is a major risk factor for SH. 6 Thus, it is imperative to take measures to help prevent hypoglycemia in these vulnerable individuals.
Because hypoglycemia is a major problem in older adults with long-standing T1D, current guidelines suggest higher HbA1c goals for this population based on the assumption that this will lead to less hypoglycemia. While this may help reduce amount of time spent in hypoglycemia, this is not enough to prevent SH in this population. The results from this study highlight the need for further research of current technologies such as CGM and threshold suspend pumps in this population.
In conclusion, hypoglycemia is common in older adults with T1D. Endogenous C-peptide appears protective, while age and duration of diabetes are inversely proportional to the amount of time spent in hypoglycemia. This could be either adaptive or maladaptive. Further studies will need to focus on both the mechanisms of these findings and the use of real-time CGM to limit hypoglycemia and glycemic variability in this population.
Footnotes
Acknowledgments
Funding was provided by the Leona M. and Harry B. Helmsley Charitable Trust.
Authors’ Contributions
All authors contributed in study concept and design, acquisition of subjects and data, analysis and interpretation of data, and preparation of the manuscript. All authors have seen and approved the final version of this article.
Author Disclosure Statement
S.N.D., A.L.P., E.M.M., and I.B.H. have no conflicts of interest. R.S.W.’s nonprofit employer is the site for multicenter clinical trials sponsored by Medtronic, Inc., Intarcia, Novo Nordisk, Sanofi, Mylan, and Calibra Medical. R.W.B.’s nonprofit employer has received consultant payments on his behalf from Sanofi and Animas and a research grant from Novo Nordisk with no personal compensation to R.W.B. G.A. has received lecture fees from BRIOmed. R.M.B.’s nonprofit employer has received consultancy payments from Abbott Diabetes Care, Amylin, Bayer, Boehringer Ingelheim, Calibra, Eli Lilly, Halozyme, the Helmsley Trust, Hygieia, Johnson & Johnson, Medtronic, Novo Nordisk, ResMed, Roche, Sanofi, Takeda, and Valeritas and grants from Abbott Diabetes Care, Amylin, Bayer, Becton Dickinson, Boehringer Ingelheim, Calibra, Daiichi Sankyo, Inc., DecCom, Eli Lilly, Halozyme, Helmsley Trust, Hygieia, Intarcia, Intuity Medical, Johnson & Johnson, MannKind, Medtronic, Merck, NIH, Novo Nordisk, ResMed, Roche, Sanofi, and Takeda with no personal compensation to R.M.B.; R.M.B. receives royalties from the Betty Crocker Diabetes Cookbook and holds stock in Merck. H.R. has received payments as a board member for Eli Lilly, Merck, Novartis, and Sanofi, as well as consultancy payments from Roche Diagnostics. H.R.’s nonprofit employer has received grants from Bristol Meyers-Squibb, Daiichi Sankyo, Eli Lilly, Lexicon, Novartis, and Novo Nordisk with no personal compensation to H.R.