
Abstract
Aim:
To assess the efficacy of ambulatory glucose profiling (AGP) generated by FreeStyle LibrePro™ flash glucose monitoring (FCGM) on glycemic control in patients with uncontrolled type 1 diabetes (T1D) and type 2 diabetes (T2D).
Methods:
Clinical and biochemical data were obtained from 5072 patients with diabetes who had an A1c ≥7% (2536 who had been initiated on FCGM-based AGP between March 2015 and October 2016 [cases] and 2536 age-, gender-, A1c-, site- and time-matched controls who were not initiated on AGP) across seven diabetes clinics in India. Anthropometric and clinical measurements were obtained through standardized techniques. Fasting and postprandial plasma glucose and glycated hemoglobin(A1c) were estimated before and after initiation of AGP.
Results:
Overall, there was a significant decrease in A1c both in cases and controls; however, the magnitude of reduction was higher among cases (1% vs.0.7%; P < 0.001).The overall reduction in A1c among cases was higher in T2D (9.2% to 8.3%) compared with T1D (9.6% to 9.4%); however, the absolute difference in A1c reduction between cases and controls was higher among T1D (0.5% vs. 0.2%) patients. The reduction in glycemic parameters was irrespective of age or gender (P for trend <0.001) across all study sites. The greatest reductions in A1c were noted within 6 months of AGP initiation. Multiple logistic regression showed that those who did not use AGP had a 1.42 higher risk (95% CI: 1.24–1.64) of not achieving even 0.1% reduction in A1c compared with those who were initiated on AGP even after adjusting for age, gender, body–mass index, systolic blood pressure, time to follow-up A1c, and medication use.
Conclusions:
This study shows that FCGM-based AGP with FreeStyle LibrePro is associated with significant reductions in A1c levels in both T1D and T2D. In addition, improvement in A1c levels was maintained across all age groups and in patients enrolled at different diabetes clinics in India.
Introduction
S
These issues have led investigators to look at devices that continuously monitor a patient's glucose levels over prolonged periods of time. However, the continuous glucose monitoring (CGM) devices available thus far suffer from a number of shortcomings that minimize their appeal to patients and clinicians. They are uncomfortable to wear, require frequent calibration with finger-stick glucose, and do not measure glycemic profiles beyond 6 days. Cost is also a major limiting factor in developing countries such as India where over a period of nearly 20 years, these CGM devices have failed to take off in clinical practice. A recently launched flash glucose monitoring (FCGM) system, the FreeStyle LibrePro™ ambulatory glucose profile (AGP), overcomes these shortcomings to a large extent by being relatively easy to use, not requiring calibration, and being relatively affordable. Hence, there has been widespread use of this system in India as it was one of the first countries where it was launched.
While earlier studies have shown that FCGM is a feasible method of assessing glycemic control over a 2-week period, there are as yet little data on the efficacy of this technology in improving A1c levels and no data comparing its effects separately in patients with type 1 diabetes (T1D) and type 2 diabetes (T2D). 3 –9 In this article, we tried to assess the efficacy of FCGM-based AGP in improving glycemic control in patients with uncontrolled T1D and T2D from seven diabetes clinics in India.
Methods
From the electronic medical records of seven diabetes clinics in India (located in Chennai, Madurai, Hyderabad, Belgaum, Trivandrum, Mumbai, and Coimbatore), we extracted data of 5785 patients who had been initiated on AGP between March 2015 and October 2016. After excluding 2833 patients whose post-AGP A1c was yet to be done, 355 with A1c<7%, and 61 with types of diabetes other than T1D and T2D, data from 2536 patients (197 with T1D and 2339 with T2D, cases) were available for analysis (Fig. 1). For comparison, age-, gender-, baseline A1c-, site-, and time-matched controls were selected from the electronic records of the seven diabetes clinics (n = 2536). Thus, the data of 5072 patients with diabetes are presented here (Fig. 1). Of the seven diabetes clinics in the study, four clinics are part of a single network comprising a chain of diabetes clinics across India, These clinics are connected through a single electronic database. Data from the centers in Belgaum, Trivandrum, and Mumbai were sent to the nodal center in Chennai, where all the data were collated and analyzed. All the centers followed standardized methodology, which was comparable across sites.

Flowchart of the retrospective study. AGP, ambulatory glucose profile; A1c, glycated hemoglobin.
Height was measured in centimeters using a stadiometer. Patients were requested to stand upright without shoes with their back against the wall, heels together, and eyes directed forward. Weight was measured with an electronic weighing scale that was kept on a firm horizontal surface. Patients were asked to wear light clothing and weight was recorded to the nearest 0.5 kg. 10 Body–mass index (BMI) was calculated using the formula: weight (Kg)/(height in m) 2 .
Waist circumference was measured using a nonstretchable measuring tape. Patients were asked to stand erect with both feet together on a flat surface; one layer of clothing was accepted. Waist circumference was measured as the smallest horizontal girth between the costal margins and the iliac crests at minimal respiration. Blood pressure was recorded in the sitting position in the right arm with a mercury sphygmomanometer and rounded off to the nearest 2 mmHg. Two readings were taken 5 min apart and the mean of two readings was taken as the blood pressure. 10
Fasting plasma glucose and postprandial plasma glucose (hexokinase method) were measured on Beckman Coulter AU2700 (Fullerton, CA) using kits supplied by Beckman. Glycated hemoglobin (A1C) was estimated by high-pressure liquid chromatography (Bio-Rad, Hercules, CA). In Chennai, the intra-assay coefficient of variation (CV) for glucose was ≤1.2% and an interassay CV was ≤2.1%. For A1c, the intra-assay CV was ≤0.7% and interassay CV was ≤1.4%. The CV for glucose and A1c in other centers were as follows: <5.5% and <3% in Belgaum; <3% and <2.5% in Coimbatore; <1% and <2.5% in Trivandrum; <3% and <2% in Madurai; <2.5% and <2.5% in Hyderabad; and <2% and <3% in Mumbai, respectively.
The FreeStyle LibrePro FCGM system for AGP consists of a coin-sized sensor that is inserted into the outer aspect of the upper arm. This single-use on-body sensor uses wired enzyme technology (osmium mediator and glucose oxidase enzyme coimmobilized on an electrochemical sensor) to continuously measure the interstitial fluid glucose every 15 min. It has a reader that downloads the data collected by the sensor and a proprietary software that uses these data to prepare graphs depicting the mean glucose values as well as glycemic variability at different times of the day during a period of 14 days. 11 It also provides daily glucose charts to enable evaluation of day-to-day glycemic control.
AGP reports were analyzed by the respective clinician in charge of the patients at each center, and modifications were made to the antidiabetic drug regimen wherever necessary based on the AGP sensor readings. Dose titration was carried out based on the guidelines proposed by the Research Society for the Study of Diabetes in India (RSSDI). 12 Glycemic parameters (fasting and postprandial glucose and A1c) were repeated after a mean time interval of 3 months from the baseline estimation.
Written informed consent was obtained from all study patients to use their anonymized medical data, and approval was obtained from the Institutional Ethics Committee.
Statistical analyses
Statistical analyses were performed using SPSS statistical package (version 20.0, Chicago, IL). Estimates are expressed as mean ± standard deviation. One-way analysis of variance (with post hoc Tukey's analysis) or Student's t test was used to compare groups for continuous variables, and chi-square test was used to compare proportions between two groups. Logistic regression analysis was performed using patients who did not achieve A1c reduction of even 0.1% as the dependent variable and using AGP, age, gender, BMI, duration of diabetes, time to follow-up A1c, systolic blood pressure, and medication use (insulin, oral hypoglycemic agents [OHAs], or insulin + OHA) as independent variables. P value <0.05 was considered significant.
Results
Cases (n = 2536) wore the FCGM sensor for a duration of 14 days. The vast majority of patients were comfortable with the sensor and reported no adverse effects. However, the sensor had to be reinserted in 36 patients in whom the original sensor failed. Three patients reported itching and allergy, 12 patients reported pain, and 5 patients reported excessive sweating at the site, none of which necessitated removal of the sensor.
Table 1 shows the baseline characteristics of the study population split by diabetes type. Controls were matched with cases with respect to age, gender, baseline A1c, site, and time period of study. Patients with T1D who were initiated on AGP were significantly taller and had significantly higher postprandial glucose levels compared with those not initiated on AGP. Among patients with T2D, those who were initiated on AGP had significantly higher diastolic blood pressure, fasting and postprandial plasma glucose, and duration of diabetes and were more likely to be on insulin compared with those not initiated on AGP. Median time to follow-up did not differ significantly between cases and controls among either type of diabetes.
P < 0.05 compared with controls.
P < 0.001.
A1c, glycated hemoglobin; AGP, ambulatory glucose profiling; BMI, body–mass index; OHA, oral hypoglycemic agent.
Figure 2 shows the change in A1c among cases and controls split by diabetes type and gender. Overall, there was a significant decrease in A1c both in cases and controls; however, the magnitude of reduction was significantly higher among cases (1% vs.0.7%; P < 0.001). Among cases, the magnitude of reduction was higher in T2D (Before-AGP vs. Post-AGP: 9.2% vs. 8.3%, P < 0.001) compared with T1D (Before-AGP vs. Post-AGP: 9.6% vs. 8.9%, P < 0.001). However, the absolute difference in A1c reduction between cases and controls among T2D patients was only 0.2%, whereas among T1D patients, it was higher (0.5%). The magnitude of A1c reduction among cases was similar in both genders.
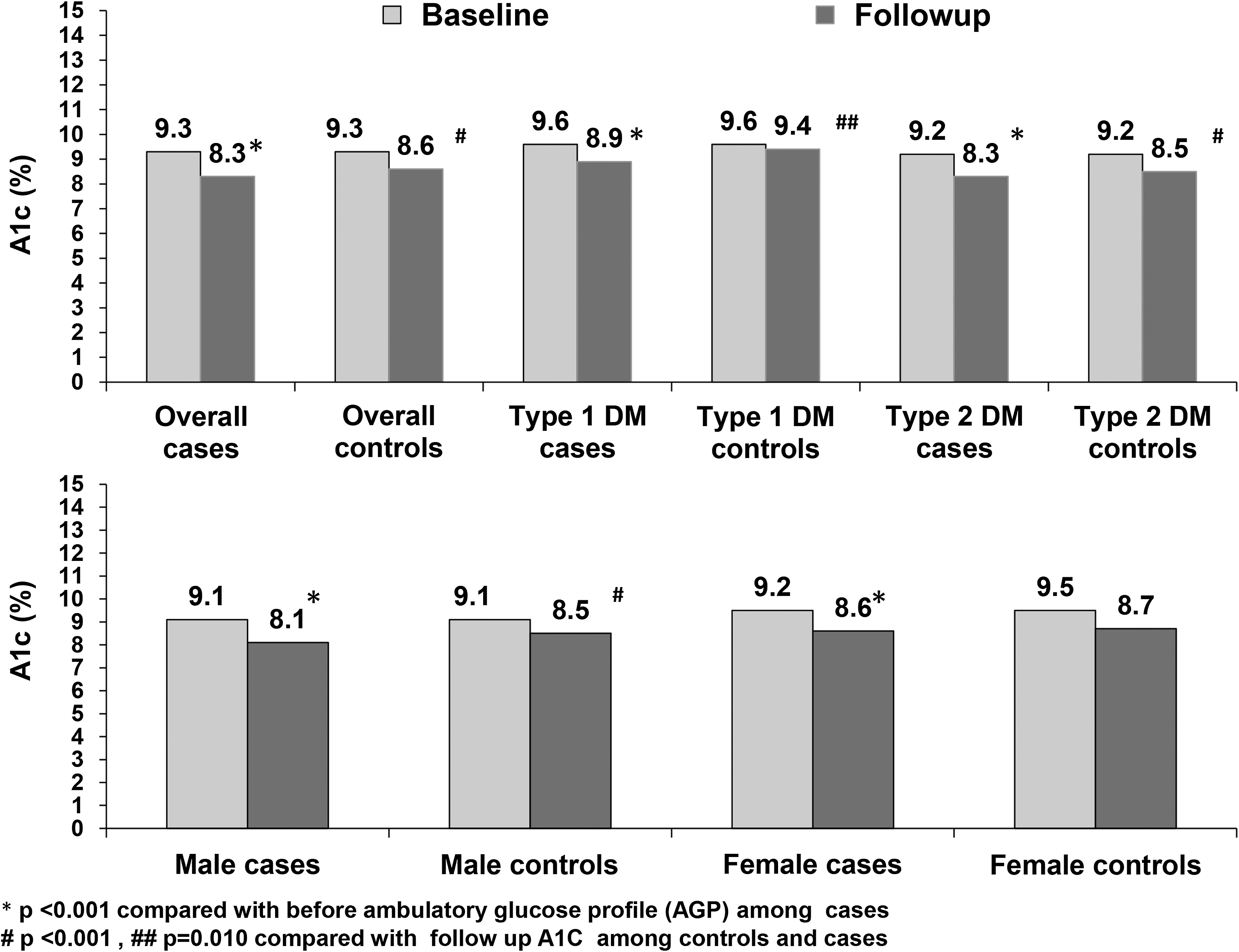
Comparison of mean glycated hemoglobin at baseline and follow-up in cases and controls stratified by type of diabetes and gender.
Figure 3 shows the changes in fasting plasma glucose (3A), postprandial plasma glucose (3B), and A1c (3C) across different age groups in those who were initiated on AGP. There was a clear separation of the lines indicating significant reductions in all three glycemic parameters, irrespective of age (P for trend <0.001).

Age-wise distribution of fasting plasma glucose (FPG)
Figure 4 shows the site-wise change in A1c among patients who were initiated on AGP. While there was a significant drop in A1c at all the sites, the most dramatic differences were noted in participants from Mumbai, Madurai, and Trivandrum.
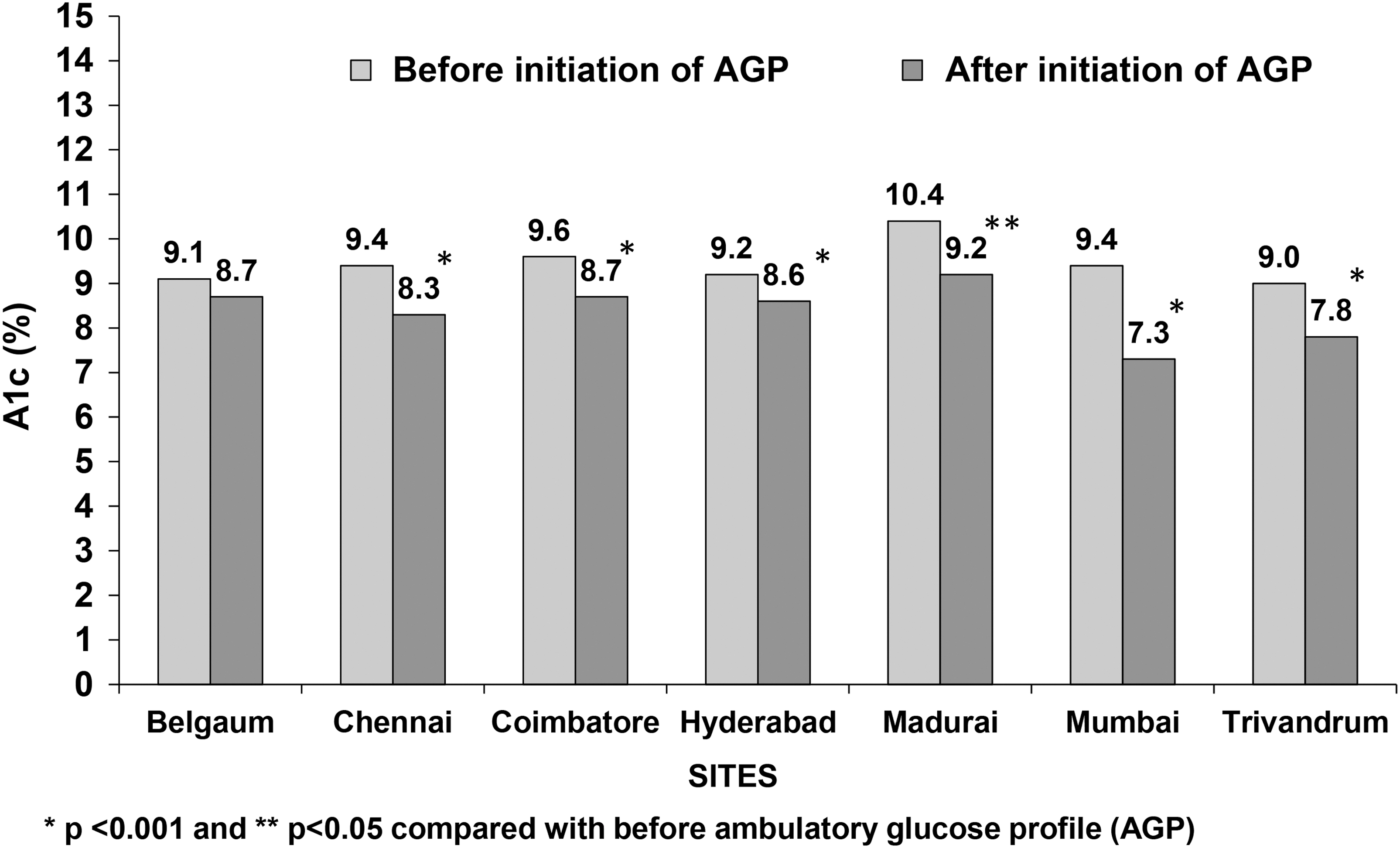
Site-wise distribution of glycated hemoglobin before and after AGP (FreeStyle LibrePro) initiation.
Delta-A1c (follow-up A1c–baseline A1c) was also assessed before and after AGP initiation based on the timing of the repeat A1c estimation. Delta-A1c done after 2–3 months of initiation of AGP was −1.34%, after 3–6 months was −1.04%, and after 6 months was −0.68% after adjusting for age, gender, duration of diabetes, management of diabetes, and sites. This suggests that the greatest reductions in A1c were obtained when repeat estimation was carried out within 6 months of AGP initiation.
We also looked at the changes in treatment that were made following AGP. Among individuals with T1D, the total daily dose of insulin was unchanged in 18.5% and increased by <10 units in 29.7%, by 10–19 units in 13.3%, and by 20 units or more in 3.6%. It was of interest that 34.9% of patients were able to decrease their insulin doses (23.6% by <10 units, 7.7% by 10–19 units, and 3.6% by ≥20 units). Among individuals with T2D, 30.4% of patients had no dose adjustment in insulin, 21.2% had an increase of <10 units, 8.7% had an increase of 10–19 units, and 3.3% had an increase of 20 units or more. A decrease in dosage of insulin by <10 units, 10–19 units, and ≥20 units was noted in 19.7%, 10.6%, and 6.2%, respectively. The dose of OHA remained unchanged in the majority of patients (71.9%), while it was increased in 20.1% (sodium glucose transporter 2 [SGLT2] inhibitors in 34.0%, dipeptidyl peptidase-4 [DPP-4] inhibitors in 30.1%, alpha glucosidase inhibitors [AGIs] in 25.0%, sulfonylurea in 11.0%, metformin in 7.4%, and thaizolidinediones in 0.5%) and reduced in 8.0% (DPP-4 inhibitors in 42.8%, SGLT2 inhibitors and AGIs in 18.1% each, sulfonylurea in 17.5%, metformin in 12.7%, and thiazolidinediones in 3.0%).
Of the 5072 patients studied, there was no reduction in A1c levels (by even 0.1%) among 1620 patients (31.9%). Table 2 presents the risk factors associated with failure of A1c reduction (of at least 0.1%) in the study population. Multiple logistic regression showed that those who did not use AGP had a 1.42 higher risk (95% CI: 1.24–1.64, P < 0.001) of not achieving even 0.1% reduction in A1c compared with those who were initiated on AGP even after adjusting for age, gender, BMI, systolic blood pressure, time to follow-up A1c, and medication use.
Dependent variable (0 = A1c reduction achieved, 1 = A1c reduction not achieved during follow-up).
Discussion
In this multicenter real-life study of patients with T1D and T2D across seven clinics in India, we show that use of AGP generated by the FreeStyle LibrePro FCGM system is associated with significant reductions in A1c in both T2D and T1D with a quantitatively greater response among T2D patients. We also show that this improvement is present across all age groups, both genders, and in patients from different parts and clinics of India.
Earlier studies on the utility of FCGM-based AGP have been chiefly confined to developed nations. However, emerging data indicate that this technology may be useful in developing countries as well. In a multicenter prospective study of 45 individuals with diabetes from China, it was shown that FCGM worked well and was accurate and easy to wear and use. 5 Distiller et al. 8 evaluated FCGM in 50 South African patients and reported that use of this technology enabled evaluation of various glycemic characteristics within a short time with minimal patient and provider input. India is one of the first counties where the FreeStyle LibrePro FCGM system, which uses blinded retrospective data over a 2-week period, has been introduced, in contrast to the real-time model used in Europe. Use of AGP has been shown to be feasible and acceptable to children with T1D in India. 6
The use of CGM or FCGM devices helps clinicians and patients to better appreciate blood glucose patterns over a period of days or weeks, thereby enabling modification of the antidiabetic drug regimen and improvement in glycemic control without increase in hypoglycemic episodes. While there are several studies evaluating the efficacy of older CGM devices (including a few from India), 13 there are little data (and none from India) on the utility of FCGM-based AGP in this respect. In 25 patients with T1D seen at a clinic in Scotland, the use of FCGM was associated with significant reductions in A1c, hypoglycemic episodes, and disease distress scores. 14 A study from Israel found that the use of FCGM was associated with significant reductions in A1c and hypoglycemic events and high levels of patient and caregiver satisfaction when applied to a mixed patient population with T1D and T2D. 15 These results are in agreement with those of the present study, where a single use of AGP was associated with significant reductions in fasting and postprandial glucose and A1c levels in patients with both T1D and T2D. Moreover, the results from the logistic regression analysis further reiterate that the benefits might be independent of age, gender, BMI, duration of diabetes, and insulin and medication use.
During the course of the study, a significant drop in A1c was found among users as well as nonusers of AGP. This could be accounted for by the fact that all study participants undertook regular follow-up visits to the study centers, where appropriate treatment modifications were made by the treating physicians. We have earlier demonstrated the benefits of regular follow-up in reducing the glycemic burden in outpatients with diabetes. 16 However, even in this closely followed up cohort, the use of AGP was associated with significantly greater magnitude of A1c reduction among both T1D and T2D patients. This additional improvement in glycemic control is of considerable interest since even minimal reductions in A1c have been shown to be associated with lower risk of chronic vascular complications. 17
Earlier studies on AGP have been confined to individuals with T1D 14,18 or included only small numbers of patients with T2D. 15 Our results suggest that AGP might be equally, if not more, effective in patients with T2D. However, it should be noted that A1c improved significantly even in individuals with T2D who were not initiated on AGP; this is probably a reflection of the relative ease by which patients with T2D can improve their glycemic control compared with T1D, most likely on account of lower inherent glycemic variability.
It is also interesting to note that significant improvements in A1c were found following AGP across all the study centers located in different parts of India where huge sociocultural differences exist. This suggests that FCGM-based AGP can be a useful tool for patients with diabetes from varying socioeconomic groups with great diversity in terms of food habits and cultural practices.
We note that the best improvements in A1c were noted when the repeat measurement was carried out within 6 months. Similarly, in the study by Ish-Shalom et al., 15 improvements in glycemic control were maintained up to 24 weeks, but only in individuals who continued using the device. This indicates that the benefits of AGP (and the consequent modification of treatment regimen) decay over time unless regular follow-up and constant reinforcement are provided.
Following the use of FCGM, most of the study patients were advised to increase the dosage of insulin (and in some cases of T2D, OHAs as well). Utilizing the information provided by AGP, such intensification can be confidently made with minimal risk of hypoglycemia. It is also interesting that more than a third of patients were able to reduce their total daily doses of insulin following analysis of their AGP. This raises the possibility that recurrent hypoglycemic episodes, with consequent defensive eating, could have been the cause of high A1c originally noted in these patients.
While FCGM-based AGP offers significant cost advantages compared with older CGM devices, it still remains an expensive tool for many in the middle and lower socioeconomic groups, especially in developing nations. Even in the United Kingdom, it was observed that the use of FCGM-based AGP was confined to the most affluent sections of society. 18 This is likely to be a limiting factor to the widespread use of this technology in India, where most patients have to pay for treatment out of pocket.
Our study has several strengths. One of the strengths of our study lies in the use of electronic medical records, which is a valuable tool for research, where complete follow-up data are available, providing a wealth of information at a glance. Another strength of this study is the large sample size drawn from seven clinics in India in a real-life setting where specific protocols were followed or patient selection was done like for conducting a randomized clinical trial (RCT). Moreover, we have compared those who used FCGM with age-, gender-, A1c-, site-, and time-matched controls, making our estimates more robust. However, there are also several limitations to our study. Being a retrospective study, we only have data on patients who came back to the respective centers. The status of the other patients is unknown. The study was performed in an outpatient clinical setting and not in a research setting, making it difficult to obtain multiple samples to assess blood glucose and other parameters from the study participants, as is done in an RCT setting. Finally, there could be some referral bias in patients selected for AGP because of the cost factor. Hence, the generalizability of these results needs to be viewed in this light.
In conclusion, this large, retrospective real-life study done across seven sites in India shows that the use of AGP generated by the FreeStyle LibrePro FCGM system helps in improving A1c levels in patients with both T1D and T2D. Further studies are needed on the cost-effectiveness of using this modality of glycemic monitoring.
Footnotes
Author Disclosure Statement
No competing financial interests exist.