
Abstract
Background and Aims:
The aim of this study was to evaluate the incidence rates of diabetic ketoacidosis (DKA) according to treatment modality in patients with type 1 diabetes (T1D) in Denmark, either multiple daily injections (MDI) or continuous subcutaneous insulin infusion (CSII).
Materials and Methods:
A total of 20,902 T1D registered in the Danish Adult Diabetes Database were followed for an average of 5.4 years. Poisson regression analyses with risk time as offset were used to compare differences in rates of DKA between CSII and MDI. Model was adjusted for age, sex, diabetes duration, previous DKA events, and hemoglobin A1 c (HbA1 c). A modifying effect of number of CSII patients on the DKA rates was tested.
Results:
During 113,731 person-years, 3100 DKA events were registered (53 among CSII). CSII patients were younger (42.3 vs. 47.9 years), a larger proportion was female (59% vs. 43%), had a shorter diabetes duration (19 vs. 21 years), and a lower HbA1c (61.9 vs. 66.6 mmol/mol). There was no significant difference in the incidence rate of DKA between CSII and MDI (rate ratio: 1.30, 95% confidence interval: 0.97–1.76). However, in clinics with at least 250 CSII patients, rates of DKA events were lower among CSII users, while the opposite was true for the smaller clinics (P = 0.016).
Conclusions:
Delivery of CSII in large diabetes clinics with sufficient support and patient education may ensure that CSII treatment does not lead to an increased risk of DKA.
Introduction
T
CSII has apparent advantages of insulin delivery for a wide age range of T1D patients, as it is adaptable to various daily activities and does not require scheduled times for insulin injection or nutritional intake. CSII users show a high degree of satisfaction and report increased lifestyle flexibility and improvement in quality of life. 4 –7 Many studies have shown decreased HbA1 c, 8 –10 reduced or at least not increased incidence of severe hypoglycemia, 11 –13 and reduction of insulin doses 9 among CSII users when treatment is changed from MDI.
There is still debate on whether CSII has advantages over MDI with regard to reduction of diabetic ketoacidosis (DKA). DKA caused by hyperglycemia and/or lack of insulin is an important acute complication of T1D, which often results in hospital admission. It is a dangerous condition and a leading cause of diabetes-related mortality in young people with T1D, 14 and results in a significant increase in medical costs. 15,16 Some studies have shown no increase in DKA 11,17 with CSII, and the rate of DKA was lower over 3 years with CSII compared to MDI, 18 while another study in children showed DKA frequency was significantly more common in CSII compared to MDI. 19 However, available data on the risk of DKA among CSII users are characterized by being predominantly in young patients, in patients with short duration of diabetes, short follow-up time, and with few incidents of DKA. However, in a meta-analysis on the incidence of DKA in CSII compared to MDI, few or no DKA episodes occurred in both groups, 20 and another pooled analysis of RCT showed no difference in DKA comparing CSII and MDI. 21
The European Association for the Study of Diabetes (EASD) and the American Diabetes Association (ADA) have joined forces to review CSII therapy, suggesting that the majority of adverse events are induced by human factors or user error rather than technical pump malfunction. 22 Furthermore, they have advocated for the necessity of education and training of pump users and healthcare professionals. It is likely that in a clinic with a large volume of CSII patients, the healthcare providers will have more experience in handling CSII patients. It was reported that an increasing number of patients and high value of experience with CSII showed a decline in DKA rates. 23 Therefore, we hypothesized that large-volume CSII clinics might have lower rates of DKA compared with small clinics.
The aim of this study was to evaluate the incidence rates of DKA according to treatment with CSII and MDI and by clinic size in patients with T1D in Denmark.
Materials and Methods
Study population
The Danish Adults Diabetes Database (DADD) is one of several nationwide clinical quality registries financed and operated by the Danish regions. The aim of DADD is to monitor the quality of diabetes care among adults in Denmark. The DADD was established in 2005. All diabetes patients of at least 17 years of age who have had contact with a hospital outpatient clinic or with a general physician in Denmark are eligible for inclusion in the DADD. Information on >90% of all assessments of hemoglobin A1c (HbA1c), blood pressure, lipid status, and urinary albumin creatinine, in addition to current treatment, smoking, body mass index (BMI), and date and result of complication screening (nephropathy, neuropathy, and retinopathy), is submitted annually. The ascertainment rate has been estimated to be >95%. 24 In Denmark, all CSII and the vast majority of all MDI patients (99%) are treated in hospital outpatient clinics.
We included 20.902 people with T1D in DADD with data available on the use of CSII or MDI. Patients with a previous DKA event at entry in DADD and pregnant women using CSII were included. Thirty-eight patients had received CSII therapy at entry in DADD. No minimum duration of CSII was defined for inclusion in the analysis. The diagnosis of T1D in DADD is based on the clinical definition according to national guidelines provided by the reporting specialist clinic.
Measurements
Clinical characteristics at baseline for each group included age, height, weight, HbA1c, blood pressure, total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglyceride in fasting state. BMI was calculated as weight/height.2 Other variables reported to DADD include type of insulin delivery (MDI/CSII), number of DKA, smoking status, diabetic duration, urinary albumin creatinine ratio (ACR), and clinic size. All parameters were reported annually. The initiation date of CSII or MDI and potential discontinuation date of CSII or MDI were reported.
Clinic size was classified into two groups as <250 patients on CSII (small clinics) and ≥250 patients on CSII (large clinics). We defined 250 patients with CSII as a cutoff because it discerns between university hospitals and regional hospitals.
All patients were classified into two groups according to use of CSII and MDI. DKA was diagnosed by ICD10 (E10.1, E11.1, E13.1, or E14.1) and included the criteria for the main or secondary diagnosis related to hospitalization. The mean follow-up period was 5.4 years, with a total of 113.731 person-years (py). A total of 5516 patients (33.089 py) were seen in large clinics on CSII clinics and 15.386 (80.642 py) in small clinics.
Statistical analyses
Patient characteristics at baseline are presented as mean and standard deviation (normal distribution) or median and interquartile range (non-normal distribution). Proportions indicated as percentages. Follow-up time was expressed as number of py. Differences in characteristics between groups of patients were tested using t-test for continuous variables and chi-square test for proportions.
Incidence rates of DKA events were modeled using Poisson regression analysis with log of the risk time as offset. To obtain a complete split between exposed and nonexposed patients, we first split the follow-up time according to pump status as no pump, on pump, and off pump. Second, the follow-up time was split at time of ketoacidosis event and third according to diabetes duration. Diabetes duration was the underlying time variable. Because the number of patients not treated with CSII was <1% of the total patient population, patients were censored at the time they went off pump treatment.
Two models were analyzed: model 1 was unadjusted, whereas model 2 was adjusted for age, sex, diabetic duration, previous DKA event (yes/no), and HbA1c at baseline. In model 1, we tested for a modifying effect of clinic size on pump treatment.
Results were presented as incident rate ratios (RRs) with 95% confidence intervals (CIs). All reported P-values were two sided, and P < 0.05 was considered statistically significant.
Data analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC) and R version 3.2.1 (the R Foundation for Statistical Computing).
Results
Baseline characteristics
During 113.731 py of follow-up (1.568 py among CSII patients), 3.100 DKA events were registered (53 events among CSII patients). Patients on CSII were typically younger (42.3-year olds on CSII vs. 47.9-year olds on MDI, P < 0.0001), a smaller proportion was male (41% vs. 57%, P < 0.0001), had a slightly longer duration of diabetes (21 vs. 19 years, P < 0.0001), a lower HbA1c (61.9 vs. 66.6 mmol/mol, P < 0.0001), lower systolic blood pressure, slightly lower lipid status (total LDL, HDL cholesterol, and triglycerides), and had higher levels of albuminuria than patients on MDI (Table 1).
Data are means (SD), medians (IQR), or proportions (95% CI).
ACR, albumin creatinine ratio; BMI, body mass index; BP, blood pressure; CI, confidence interval; CSII, continuous subcutaneous insulin infusion; HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein; MDI, multiple daily injections; SD, standard deviation.
In CSII users, 36 episodes of DKA occurred within 1 year after start of CSII, 15 episodes of DKA occurred in the second year after CSII initiation, and only two episodes of DKA occurred after the third year.
The incidence rate of DKA
In this study, the overall incidence rate of DKA per 1000 py was 27.3 (95% CI: 26.3–28.2). There was a significantly higher DKA incidence among females (31.9 [30.3–33.5]) compared to males (23.8 [22.7–25.0]), P < 0.001. For both females and males, the age group below 40 years had the highest mean incidence rate of DKA compared with older age groups (P < 0.001; Fig. 1A). In general, incidence rates of DKA seemed to decrease with age, although females experienced a significant increase in incidence rate from age 60 to 69 to the oldest age group of ≥70 years (P < 0.001). Except for the age group 50–69 years, females had significantly higher DKA incidence rates than males (P < 0.001). A decrease in DKA rate was also found with longer diabetes duration in both males and females (Fig. 1B). Moreover, DKA incidence rates increased with increasing HbA1c (Fig. 1C), with similar rates for females and males for HbA1c levels up to 96 mmol/mol. For HbA1c levels above 96 mmol/mol, there was a significantly higher increase in incidence among females (P < 0.001).
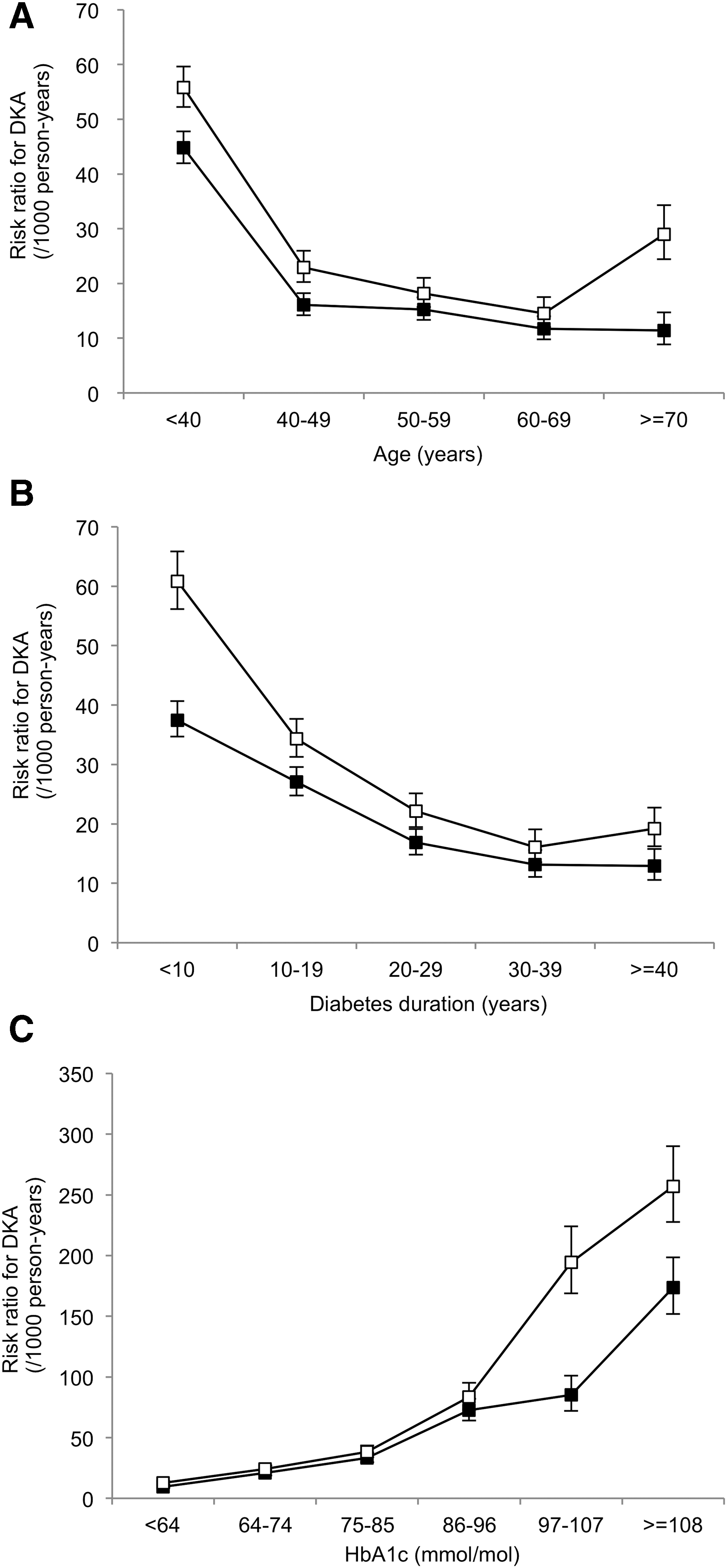
Mean incidence rates (per 1000 person-years) of DKA for male (black) and female (white) by groups of age
Furthermore, the incidences of DKA per 1000 py were 27.2 (26.2–28.1) on MDI and 33.8 (25.8–44.2) on CSII. There were no overall significant differences in the incidence rates of DKA between patients with CSII and patients with MDI in both models (model 1: RR: 1.23, 95% CI: 0.91–1.65, P = 0.178 and model 2: RR: 1.30, 95% CI: 0.97–1.76, P = 0.084; Fig. 2).
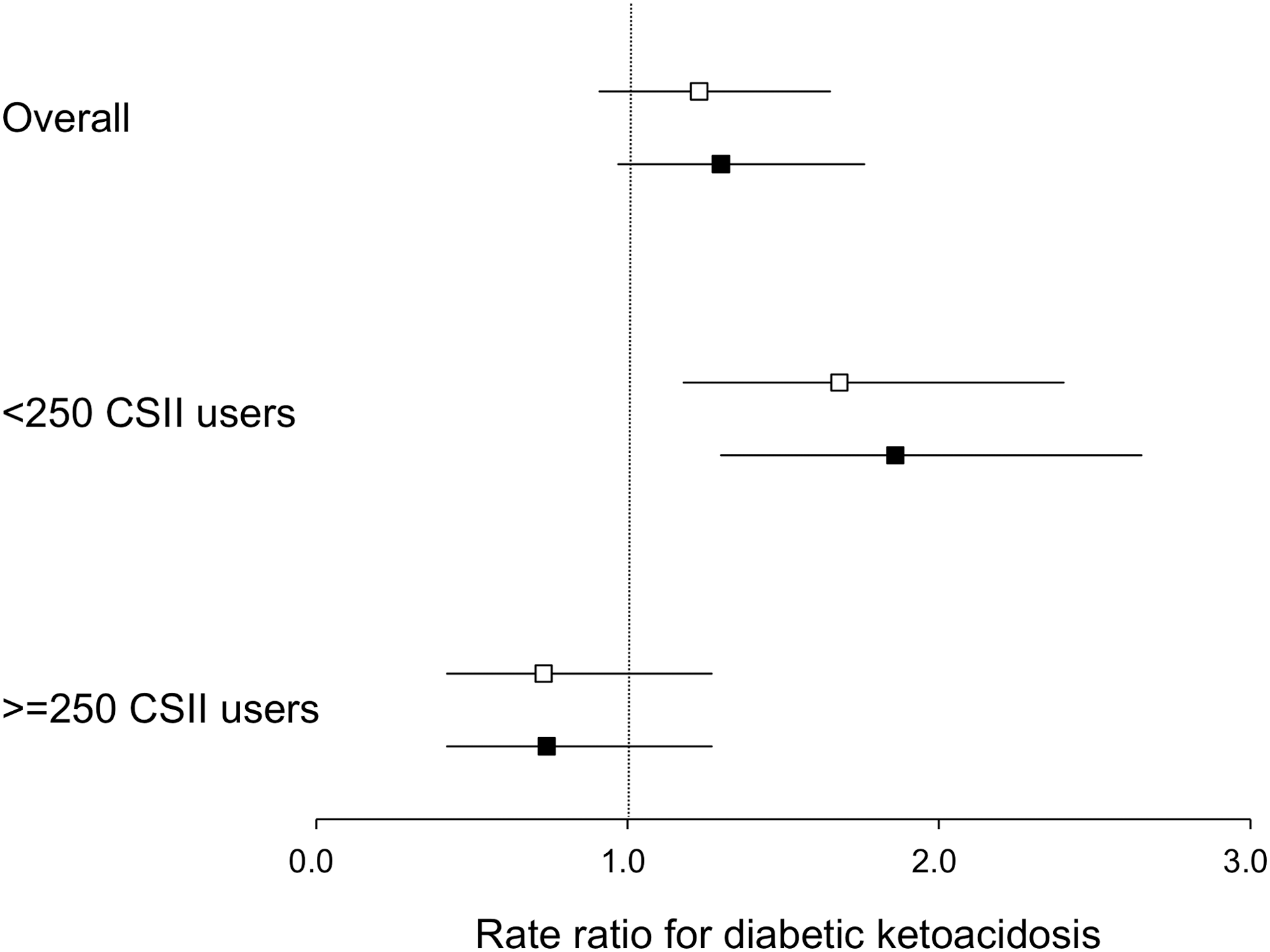
Estimated incidence rate ratios (with 95% CI) of DKA events with CSII therapy compared with MDI therapy overall and by two clinic size. Model 1 (white): unadjusted; Model 2 (black): adjusting for age, sex, diabetes duration, previous DKA events, and HbA1c.
However, there was a significant modifying effect of clinic size on the association between CSII therapy and DKA events (P = 0.016). In clinics with <250 T1D patients on CSII therapy, the rates of DKA were higher among CSII patients compared with MDI patients (model 1: RR: 1.68, 95% CI: 1.18–2.40, P = 0.004 and model 2: RR: 1.86, 95% CI: 1.30–2.65, P = 0.001; Fig. 2). In contrast, there was no significant difference in the incidence of DKA leading to hospital admissions in clinics with >250 CSII users.
Discussion
This study is the first to present nationwide population data that document the relationship between DKA and CSII in T1D patients in Denmark. There was no overall significant difference in the incidence rate of DKA between patients with CSII and patients with MDI. However, when stratifying for clinic size, we found that there was a decreased risk of DKA associated with CSII use in clinics with >250 CSII users.
The overall incidence of DKA in T1D diabetes patients was 27.3 per 1000 py in this study. Previous studies in adults have reported somewhat higher incidence of DKA, especially among patients who are not in excellent metabolic control. 25,26 Furthermore, in a Danish population study, the annual DKA incidence rate was 0.045 per diabetes patient in 1994. 27 Although not directly comparable to our findings because no CSII patients were included, the overall incidence of DKA may have decreased.
DKA events occurred less frequently with increasing age in our study, also seen in a previous study. 28 In addition, other studies have associated a higher frequency of DKA with female sex, lower socioeconomic status based on education level, income and insurance status, and the presence of psychiatric disorder. 1,28,29 In these studies, diabetes duration was not associated with the incidence of DKA.
Among CSII users, it was reported that the most common causes of DKA in children with CSII were missed insulin doses (48.6%), gastroenteritis (14.1%), pump problems (12.7%), infection (13.4%), and social problems causing insulin omission (1.4%), almost half the incidence of DKA related to human factors. 18
Moreover, it was reported that 42% of DKA episodes occurred due to insulin error or manipulation in young adults (<25 years). According to pediatric follow-up studies, the frequency of DKA was 3.2–6.6/100 py, 11,18 whereas in adult patients, the DKA frequency was 1.8/100 py with CSII in DCCT. 19 It is suggested that procedural problems are likely to be the major causes of ketoacidosis in young patients.
Also, more than three in four DKA events occurred within 1 year of initiating CSII during the 2-year follow-up, suggesting a reduced DKA incidence with increased patient experience. 18 Our study showed similar results: virtually all DKA events occurred within 2 years after CSII start.
A joint statement from EASD and ADA has pointed out that preventable human factors occur more commonly in nonspecialized practices. 22 In this study, we had no information on the reasons for DKA events, but we did find a higher rate of DKA among CSII users only in the smaller and possibly less specialized clinics.
This report highlights the differences in the incidence of DKA among T1D patients on CSII treatment in large CSII clinics compared with smaller clinics. These differences are unlikely to be related to the volume of the clinic per se, but possibly due to the improved skills and experience of the medical team (doctors, nurses, and others) seeing a larger volume of CSII patients. The ability to educate patients in the technical aspects of CSII usage and follow-up care may improve accordingly. One study reported a decrease in the rate of DKA after introducing a prevention program with increased symptom awareness, practical advice on early intervention including sick day guidelines, and 24-h access to the diabetes healthcare team. 30
Differences in the use of sensor-augmented pumps (SAPs) could also contribute to a reduced risk of DKA with CSII due to improvements in glycemic control. 31 There are large regional differences in the use of SAPs in Denmark. In the capital region, 6%–7% of the adult T1D population use sensors, whereas this is only the case for 1% of the adult T1D population in the neighboring region. 32 However, information on SAP use is not available in the present study.
The strengths of this study include a large number of adult participants with long duration of diabetes and a long follow-up time with measurements reported annually for the vast majority of patients. Each individual with T1D who was treated with CSII or MDI at registration was reported to a national clinical quality database (DADD). 33 Treatment costs are covered by healthcare providers in Denmark, so it is not necessary to pay additional costs for CSII for patients, and socioeconomic factors are thus unlikely to confound the observed associations.
There are some limitations to this study. First, no information on type of insulin among MDI users was available. Second, we do not know their history of CSII or MDI treatment before entry into DADD. Third, the value of HbA1c was reported only once a year in this study and the level of HbA1c may fluctuate during treatment. Fourth, the DADD holds no information regarding the use of SAPs or stand-alone CGM. In our clinical experience, relatively more CSII patients than MDI patients have their treatments supplemented with sensors.
The number of insulin pump users is expected to expand among all age groups in the future, and DKA may remain an important acute complication in T1D patients. To minimize the risk of DKA among CSII users, well-experienced and trained medical staff and adequate education for patients and their families in CSII usage are needed, not only at clinics with a large number of CSII users but also at smaller clinics.
Conclusions
Treatment with CSII in large diabetes clinics with sufficient support and education for patients may ensure that CSII treatment does not lead to an increased risk of DKA.
Footnotes
Acknowledgment
No funding was received for this study.
Author Disclosure Statement
G.S.A., M.E.J., D.V., and H.U.A. own shares in Novo Nordisk A/S. M.E.J. has received research grants from Astra Zeneca and from Amgen A/S. H.U.A. participates in advisory boards for Novo Nordisk A/S and Astra Zeneca.