
Abstract
In this brief report, we describe the feat of four men with type 1 diabetes mellitus (T1DM) who decided to take part in a mountain ultramarathon in Bieszczady, Poland on May 27, 2016. Before participating in the competition, they asked two diabetologists for a consultation and to assist in diabetic control during the marathon. The aim of the study was to assess the metabolic safety in people with T1DM during extreme physical exertion in a mountain ultramarathon. All subjects were treated with continuous subcutaneous insulin infusion. The marathon route was 82 km, and the sum of the climbs and descents was 3235 and 3055 m, respectively. Diabetologists controlled glucose levels using a glucometer, plasma lactate levels, and ketones in the capillary blood. In addition, they monitored the intake of carbohydrates and fluids. Clinical tests were performed at the three checkpoints (at 32, 49, and 66 km) during the race and after completing the race (at 82 km). This study shows that extreme physical exertion by a person with type 1 diabetes is possible. All subjects avoided severe hypoglycemia by significantly reducing their insulin dose and consuming additional carbohydrates. Such actions, despite the occurrence of hyperglycemia >250 mg/dL did not result in ketoacidosis. Safe participation in mountain ultramarathons by people with type 1 diabetes can be achieved if they undertake appropriate physical and diabetologic preparation.
Introduction
D
With the currently available therapies and recommendations, it is now possible for people with T1DM to play extreme sports and make physical efforts of a very high intensity. Indeed, professional athletes with T1DM have been shown to win Olympic medals or World Championships. 6 These athletes usually work closely with diabetologists and diabetes management is an important part of their training and daily work. 7 However, little data exists in the literature on extreme physical efforts in people with T1DM practicing amateur sport. 8 Such extreme feats include marathon running, the ironman competition, or mountain climbing.
In this brief report, we describe the feat of four men with T1DM who, on their own initiative, decided to take part in a mountain ultramarathon. The aim of the study was to assess the metabolic safety in people with T1DM during extreme physical exertion in a mountain ultramarathon.
Materials and Methods
This study included four men with T1DM who participated in the mountain ultramarathon in Bieszczady, Poland on May 27, 2016. Written informed consent was obtained from the participants. The study was approved by the Ethics Committee of the Poznan University of Medical Sciences. All subjects were treated with continuous subcutaneous insulin infusion (CSII). Subject 1 was using Medtronic's MiniMed 640G pump system (Medtronic, Northridge, CA), subjects 2 and 4 were using Medtronic's Paradigm 715 pump system (Medtronic), and subject 3 was using the Accu-Chek Combo insulin pump (Roche Diagnostics, Mannheim, Germany). All subjects were under permanent diabetic care, educated in the procedures to be undertaken during the exercise, and had not required hospitalization for decompensation of diabetes in the last few years. The subjects had no other diseases apart from diabetes and no chronic complications of diabetes. In the last few years before participation in the ultramarathon, all subjects had completed traditional marathons (distances of 42 km and 195 m in elevation) several times, and all played sports regularly. Subject 1 had previously reached the Aconcagua summit (6962 m above sea level) in 2016. 9
Ultramarathon performance details
The marathon route was 82 km, and the sum of the climbs and descents was 3235 and 3055 m, respectively. The rules for the mountain ultramarathon required that all participants completed the marathon in pairs for security reasons; subjects 1 and 2 were pair I, and subjects 3 and 4 were pair II. The race began at 3:00 AM. Subjects' care during the marathon was provided by two diabetologists, who controlled glucose levels using a glucometer (Contour Plus; Ascensia Diabetes Care), plasma lactate levels (Lactate Scout; EKF-Diagnostics), and ketones in the capillary blood (Optium Xido Neo; Abbott Diabetes Care, Alameda, CA). In addition, the diabetologists monitored the intake of carbohydrates and fluids. These clinical tests were performed at the three checkpoints (at 32, 49, and 66 km) during the race and after completing the race (at 82 km). The fluid intake and carbohydrates consumed in the form of bars, energy gels, and isotonic drinks were evaluated throughout the race. The subjects also made decisions on insulin dosing and carbohydrate intake during the race on the basis of their continuous glucose monitoring (CGM) or flash glucose monitoring systems: subject 1 was using the SmartGuard MiniMed 640G system (Medtronic), while subjects 2, 3, and 4 used the FreeStyle Libre technology (Abbott Diabetes Care). CGM data from patient 2, 3, and 4 were collected with iPro2 (Medtronic). The race rules required competitors to complete the whole distance within 16 h. Adverse metabolic events were those of hypoglycemia, defined as blood glucose <70 mg/dL, hyperglycemia >250 mg/dL, and ketonemia >0.6 mmol/L.
Results
The characteristics of the four subjects participating in the mountain ultramarathon are shown in Table 1. The race was completed by both pairs of subjects within the required time limit: pair I achieved a total time of 13 h 32 min and the pair II, 15 h 42 min. Subjects 2 and 4 had episodes of mild hypoglycemia. In subjects 2 and 3, much higher glucose levels than those recommended were reported during the race, but no dangerous ketonemia was observed (the maximum observed value was 1.5 mmol/L). Subjects 1 and 4 did not experience any episodes of hyperglycemia >250 mg/dL during the long effort. Although all subjects significantly reduced their insulin dose and far exceeded daily carbohydrate intake, glycemia levels remained close to 100 mg/dL (Table 1). The personal insulin pump infusion system did not detach in any subject. In subjects 2 and 3, sensors slid out of the subcutaneous tissue as a result of increased sweating just before the end of the marathon.
Mean ± standard deviation.
BMI, body mass index; ND, not determined; TDID, total daily insulin dose (based on 30 days data before the marathon).
Marathon details in respect to glycemia, carbohydrate consumption, and insulin adjustment
Subject 1
This subject gave one insulin bolus before a meal preceding the marathon. No additional insulin boluses were administered during the race (Fig. 1A). Throughout the marathon, the SmartGuard MiniMed 640G insulin pump stopped the supply of basic insulin infusion four times to prevent hypoglycemia (the Suspend Before Low setting was 70 mg/dL). This subject consumed 490 g of carbohydrates, and no events of hyperglycemia were observed throughout the race.
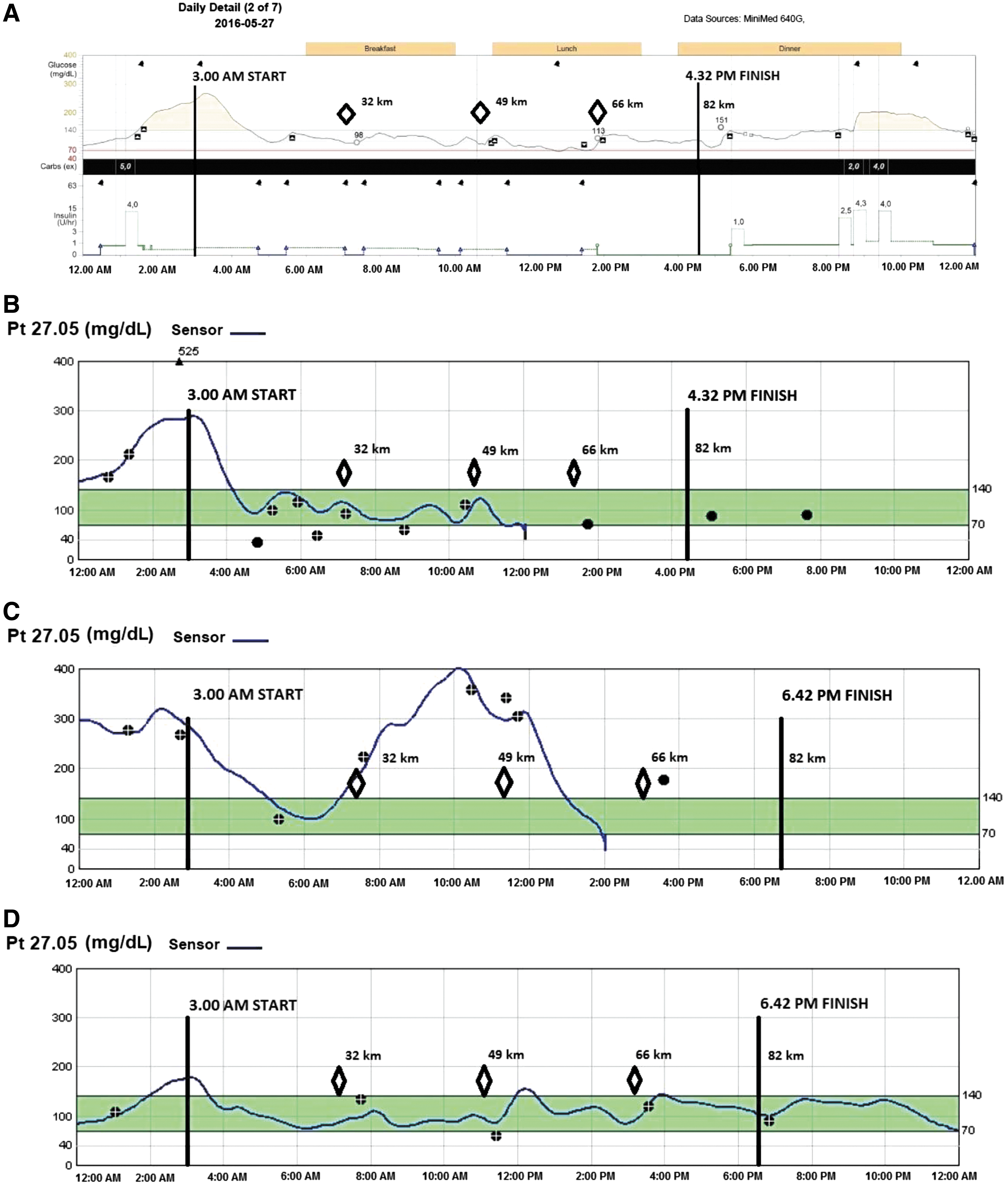
Blood glucose fluctuations during ultramarathon in T1DM subjects—personal reports.
Subject 2
At the start of the marathon, an event of hyperglycemia (480 mg/dL) was recorded for this subject, which probably resulted from the excitement of the start of the competition (Fig. 1B). However, ketone levels were at a normal level (0.2 mmol/L) at the start of the race. Due to the well-being and negative ketones, the patient decided to continue running. The subject made decisions based on the FreeStyle Libre glucose monitoring system, and applied correction boluses at 3:00 and 3:50 AM, in conjunction with mild events of hypoglycemia caused by the intense physical effort. Glucose levels of 40 and 49 mg/dL were observed before reaching checkpoint 1, and a glucose level of 61 mg/dL was reached in the second stage of the race. The consumption of 640 g of carbohydrates, and stopping the basal infusion of insulin for a total time of 3 h, allowed this subject to maintain stable blood glucose levels until the completion of the race. Ketone levels of 1.1 and 1.5 mmol/L (at 65 and 82 km, respectively) were not accompanied by events of hyperglycemia.
Subject 3
For fear of hypoglycemia, this subject did not administer any insulin boluses before the race and reduced their basal insulin infusion by 80% (Fig. 1C). Blood glucose at the start of the race was at 290 mg/dL, with ketone levels of 0.0 mmol/L. Despite a significant reduction in the insulin dose, glucose levels decreased to normal values at around 6:00 AM. The subject applied the first insulin bolus of 1.0 U at 7:00 AM during the meal at checkpoint 1 (32 km). The ketone levels were at 0.9 mmol/L. The consumption of carbohydrates and reduction in insulin dose caused hyperglycemia in this subject. By 4:00 PM, the basal insulin infusion was reduced by 50%, but an additional 7.2 U of insulin was applied in seven small boluses. From 5:00 PM, a temporary basal insulin infusion dose equivalent to 150% was used.
Subject 4
During the entire race, this subject used reduced basal insulin infusion by 80% and applied seven insulin boluses ranging from 0.1 to 0.5 U (Fig. 1D). The lowest glucose level registered was 60 mg/dL at 11:25 AM during the test at checkpoint 2. The consumption of 565 g of carbohydrates did not cause hyperglycemia in this subject. Ketone levels of 1.3 and 1.2 mmol/L (at 49 and 82 km, respectively) were not accompanied by events of hyperglycemia.
Table 1 shows the total fluid and carbohydrate intake for each subject, as well as the glucose, lactate, and ketone levels at each checkpoint.
The glycemic control and insulin adjustment after the marathon
Subject 1
Due to SmartGuard technology, on the first day after the marathon, insulin delivery was stopped for 6 h 37 min. Patient did not reduce insulin doses in boluses. Patient did not experience any episodes of hypoglycemia. The next 24 h were not different from normal days.
Subject 2
In the first 24 h, patient experienced hypoglycemia 51 mg/dL at 9:15 AM and 52 mg/dL at 2:30 PM and consumed about 150 g carbohydrates without additional insulin boluses. In the next 24 h, he experienced hypoglycemia 56 mg/dL at 10:15 PM, but insulin doses were not reduced.
Subject 3
This patient did not reduce insulin doses and did not record hypoglycemia event on glucometer. On FreeStyle Libre, glycemia below 70 mg/dL was noticed as follows: at 6:30 AM 62 mg/dL, 8:30 AM 64 mg/dL, and at 12:30 PM 68 mg/dL on the first day after the run and at 7:30 AM 48 mg/dL the next day.
Subject 4
This patient did not significantly change insulin dosage and carbohydrate intake in the 2 consecutive days after the marathon.
Discussion
Our major finding is that extreme physical exercise during ultramarathon is possible and safe in type 1 diabetic patients, however, requires personal individual decision-making based on previous experience. Scientific diabetologic societies recommend physical activity for people with diabetes, as it is associated with numerous benefits for their physical health and psyche. 10 –12 However, these societies do not recommend physical activity for those with blood glucose levels >250 mg/dL coexisting with ketonemia, or blood glucose levels >300 mg/dL regardless of ketonemia. Several publications have determined the size of the insulin dose reduction required before and after exercise, and the amount of extra carbohydrates to be consumed, to achieve metabolic control in these individuals. 13 However, these recommendations for people with T1DM undergoing exercise do not take into account extreme situations, such as participation in mountain ultramarathons. Indeed, a race lasting several hours in difficult terrain and generating maximum fatigue is a big challenge even for healthy individuals and is certainly not regarded as a normal physical activity. Moreover, blood glucose fluctuations have previously been shown to occur in diabetic patients even during prolonged walking exercises of uniform moderate intensity. 14 Therefore, during intense physical activity (such as an ultramarathon), the use of new CGM systems may increase the security of athletes with diabetes, as shown previously. 15
Only single descriptions of extreme efforts made by people with T1DM have been described in the literature. 16,17 The current study is unique in that we observed four men with T1DM simultaneously, who were all amateur athletes. The results obtained in this study by race participants with T1DM indicate that what seems to be metabolically dangerous, 18 in fact, does not endanger the health and life. Indeed, all subjects successfully completed the ultramarathon despite having T1DM.
Even though all four men experienced the same external conditions, different glycemic phenomena were generated. Moreover, the responses of the four subjects differed based on their individual knowledge and experience. Each subject made their own decisions on carbohydrate and insulin intake between the checkpoints, without the participation of doctors. All subjects were advised to consume carbohydrates in accordance with the principle that for every hour of exercise, 0.3–0.5 g of carbohydrates per kg of body weight should be consumed. This carbohydrate intake only applies to the planned physical activity, when the insulin dose was reduced. In addition, all subjects replaced body fluids in adequate amounts required for an ultramarathon in extreme conditions.
It is worth noting that despite unacceptably high glucose levels in two of the subjects at the start of the race, all subjects completed the ultramarathon without any metabolic complications. Their sporting success, which can be described as a great feat, confirms progress in the field of diabetes therapy using CSII. Of interest, study participants reported neither substantial deterioration nor improvement of their glycemic control following the marathon. This may be due to the fact that their physical activity before and after the run was actually not substantially different from their high, routine activity. Generally, changes in lactate concentrations in the patients were similar to those observed in healthy subjects and indicate overwhelming predominance of aerobic exercise during the race. The single elevated lactate levels at each of the checkpoints are likely due to patients' acceleration at the end of the given ascending distance. Finally, significantly elevated blood ketone levels in two of the subjects should be noted. However, none of the results exceeds 1.5 mmol/L and is probably related to insufficient carbohydrate consumption. 19
Modern technologies, such as CSII and CGM, have made performing sports for T1DM patients much more effective and safer. 20 We also state that without such technologies the achievement that we describe in our article probably would not be possible or would be related to much higher risk.
In conclusion, this study shows that extreme physical exertion by a person with type 1 diabetes is possible. All subjects avoided severe hypoglycemia by significantly reducing their insulin dose and consuming additional carbohydrates. Such actions, despite the occurrence of hyperglycemia >250 mg/dL did not result in ketoacidosis. Treatment with a CSII system allows the person with diabetes to use a temporary basal rate of insulin, administer additional small boluses of insulin, or even to suspend the supply of insulin. 21 In conclusion, safe participation in mountain ultramarathons by people with type 1 diabetes can be achieved, if they undertake appropriate physical and diabetic preparation.
Footnotes
Author Disclosure Statement
A.G., M.T.M., and T.K. have received speaker's fees from Abbott Laboratories, Ascensia Diabetes Care, Medtronic MiniMed, Roche Diabetes Care. D.Z.-Z. have received speaker's fees from Medtronic MiniMed and Roche Diabetes Care. B.M. and J.H. have received speaker's fees from Ascensia Diabetes Care.