
Abstract
Background:
A variety of prescriptions and over-the-counter medications interfere with transcutaneous continuous glucose monitoring (CGM) sensors. This study characterized the interference profile of the Eversense® CGM System (Senseonics, Inc., Germantown, MD), which has a different mechanism of glucose detection than other CGM systems.
Materials and Methods:
Sensor bias (sensor glucose concentration measurement – plasma glucose concentration measured by a reference test) was measured in vitro against 41 different substances at supratherapeutic/supraphysiologic plasma concentrations. Testing was performed using a paired-sample method adapted from the Clinical and Laboratory Standards Institute guidance document EP7-A2. Any substance producing sensor bias that exceeded the International Organization for Standardization (ISO) document 15197:2013 limits was then tested using an in vitro dose–response method to determine whether the concentration producing a significant sensor bias was within physiologic/therapeutic concentration ranges.
Results:
Eight of 41 substances produced a sensor bias that exceeded ISO 15197:2013 limits when tested in vitro at supratherapeutic/supraphysiologic plasma concentrations. Only two of these substances (tetracycline and mannitol) exceeded bias limits within therapeutic concentration ranges. Notably, neither acetaminophen nor ascorbic acid, which are substances reported to interfere with other CGM systems, produced sensor bias that exceeded ISO limits when used at physiologic concentrations.
Conclusions:
Although tetracycline and mannitol interfered with the Eversense sensor, substances frequently reported to interfere with enzymatic, electrochemical-based transcutaneous CGM systems, such as acetaminophen and ascorbic acid, did not affect Eversense readings.
Introduction
C
Studies have suggested that various substances including ascorbic acid (vitamin C), acetaminophen, dopamine, maltose, xylose, and mannitol may interfere with the function of electrochemical glucose sensors. 9 –12,15,16 Vitamin C and acetaminophen are of particular concern as they are very commonly used over-the-counter medications and hence may be taken without medical supervision. Furthermore, physicians are frequently unaware of their patients' nonprescription medication use, 17,18 and these substances are available as or incorporated into a variety of branded or combination product over-the-counter analgesics, cold remedies, or supplement formulations. Users may be unaware that they are ingesting the specific substances against which they may have been counseled 19 or that they may inadvertently take doses that exceed recommended amounts. 20
The novel Eversense® CGM System (Senseonics, Inc., Germantown, MD) utilizes a fully subcutaneously implantable glucose sensor (Fig. 1) whose accuracy and clinical utility for 90- and 180-day periods have been validated in prospective, multisite clinical trials. 21,22 Although substances such as ascorbic acid, acetaminophen, dopamine, maltose, xylose, and mannitol can interfere with CGM systems that use electrochemical- and enzymatic- (i.e., glucose oxidase and glucose dehydrogenase) based methods to measure glucose concentrations, 9,11,12,15,23 –25 the Eversense CGM sensor uses an abiotic (non–enzyme based), fluorescent glucose-indicating polymer to measure glucose 26 (Fig. 2) and, therefore, may have a different drug interference profile. Electrochemical enzymatic-based sensors are potentially subject to interference from substances (e.g., acetaminophen) that may electrochemically react at the sensor working electrode or that may exhibit cross-reactivity with the enzyme. The Eversense sensor does not contain an electrode or an enzyme and is, therefore, not subject to those specific interference mechanisms. Rather, substances that may bind to the Eversense sensor polymer or that may absorb or fluoresce light over the spectral operating range of the sensor could potentially interfere with sensor glucose readings. Therefore, the goal of this study was to use commonly accepted in vitro test methods 27 to assess the potential for various substances to interfere with Eversense CGM sensor glucose measurements.
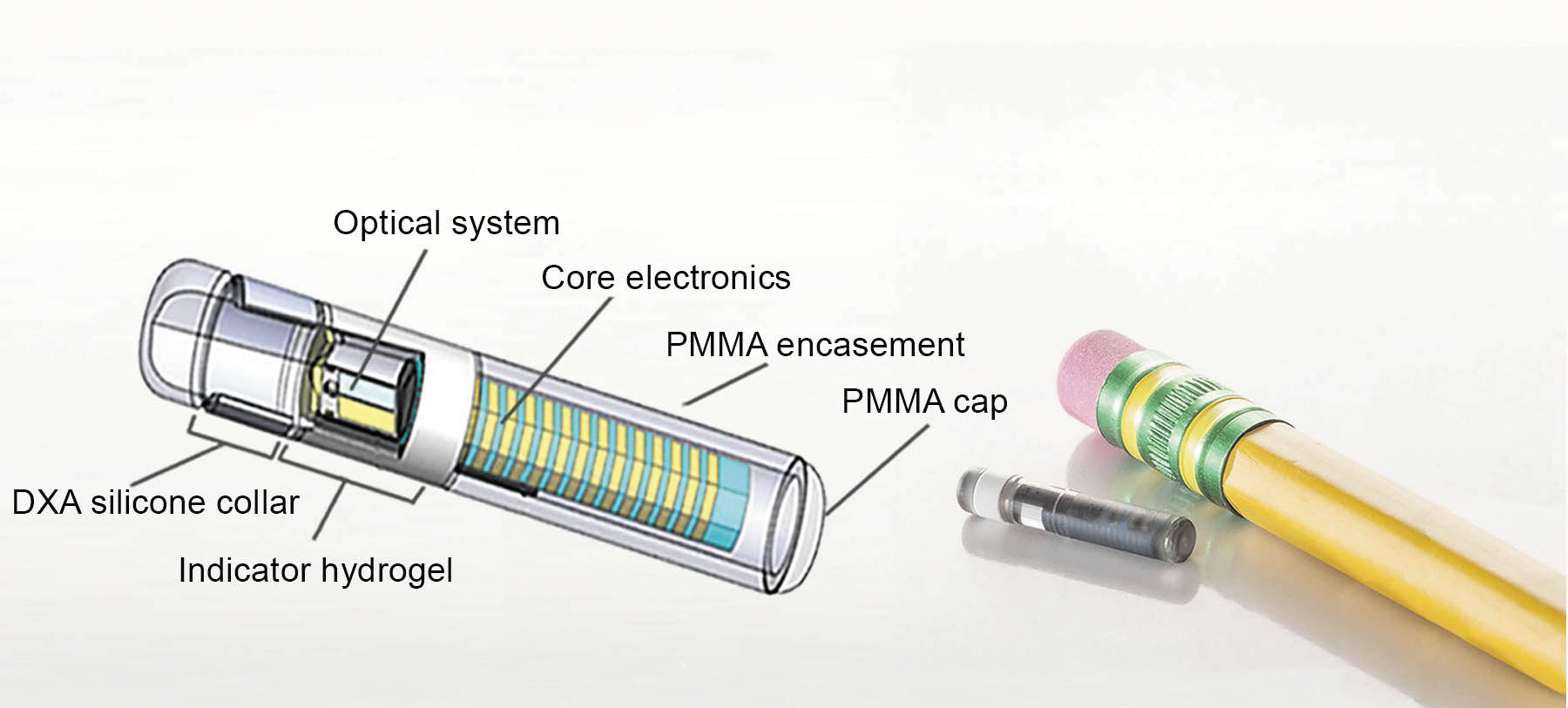
Eversense® implantable glucose sensor. DXA, dexamethasone acetate; PMMA, poly(methyl methacrylate).
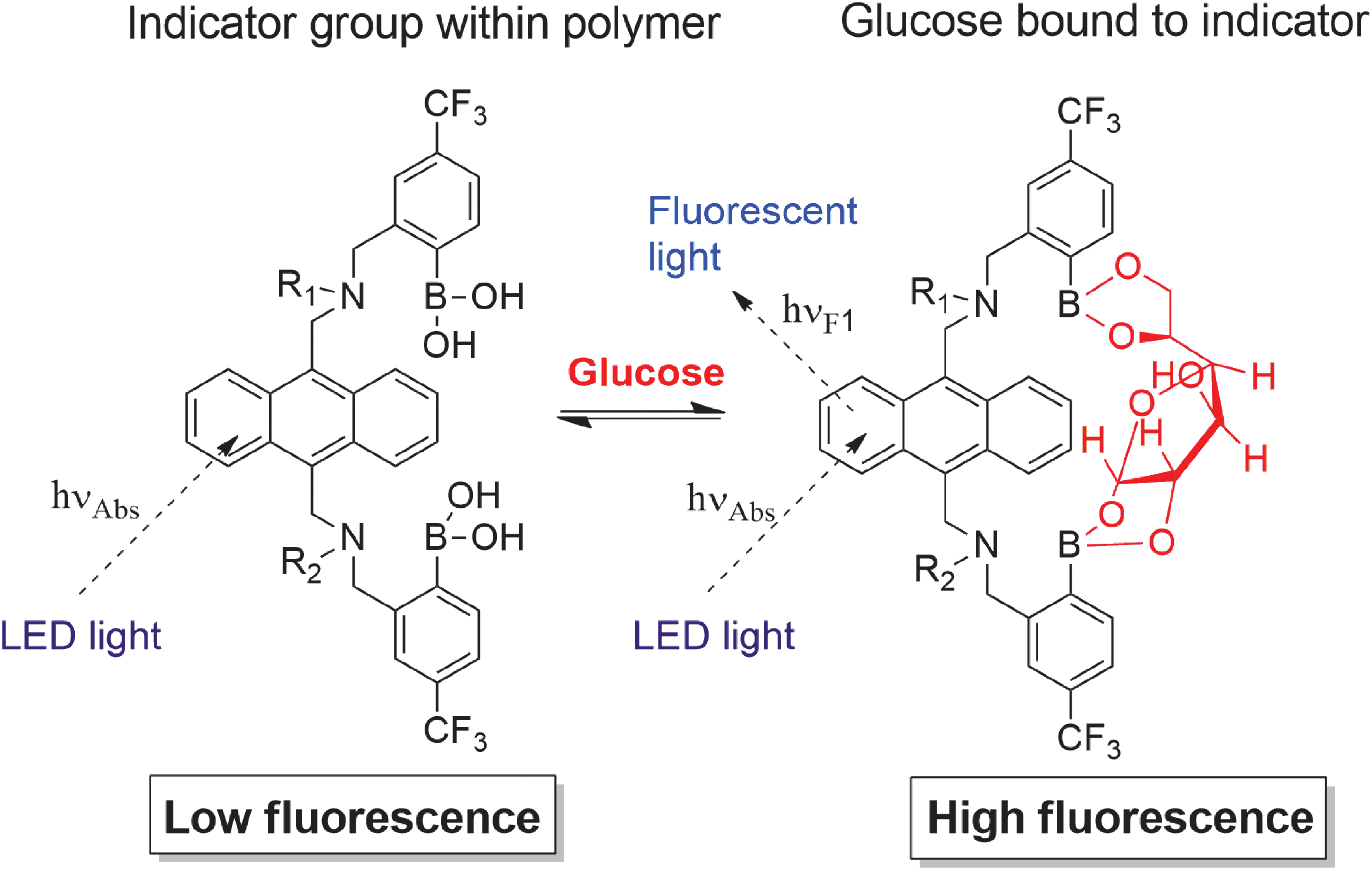
Equilibrium binding of glucose to the glucose indicating polymer and effects on fluorescence. R2 denotes connectivity to the indicator polymer backbone. 26 LED, light-emitting diode.
Materials and Methods
An in vitro screening study was performed to assess the potential for various endogenous and exogenous substances to interfere with the accuracy of the Eversense CGM sensor.
Selection of substances for in vitro interference testing
The Eversense CGM sensor uses an abiotic, fluorescent glucose-indicating polymer (a hydrogel) that is formed onto the surface of the sensor housing (Fig. 1) to measure glucose concentrations. 26 The fundamental recognition reaction is a reversible condensation of the cis-diol groups of glucose with the bis-boronate moieties of the indicator polymer. Glucose binding at the boronic acids disrupts intramolecular fluorescence quenching (from the indicator amine groups), resulting in an increase in fluorescence intensity without chemically altering the indicator molecule. This photo-induced electron transfer quenching transduction mechanism has been described in other reports. 26,28 The boronic acids groups are spatially placed to form a glucose-sized binding cleft 28 (Fig. 2). Vicinal diol (two adjacent hydroxyl groups)-containing molecules, particularly those structurally related to glucose, have the highest likelihood of exhibiting cross-reactivity, 28 and, therefore, substances from the various classes of vicinal diols (i.e., monosaccharides, disaccharides, polysaccharides, sugar alcohols, catechols, alpha-hydroxy carboxylic acids, and aminosugars) were selected for interference testing (Table 1).
Rows highlighted in gray are substances that exceeded interference test bias limits.
Obtained from EP7-A2 unless otherwise indicated by reference.
Bias reported as percentage at glucose test concentrations >100 mg/dL (5.5 mmol/L).
Tested at the concentration specified by FDA Guidance document for Blood Glucose Monitoring Test Systems.
See the Discussion section for discussion of mannitol tests.
CGM, continuous glucose monitoring; EDTA, ethylenediaminetetraacetic acid; FDA, U.S. Food and Drug Administration; NA, not available.
Furthermore, glucose binding results in an increase in fluorescence intensity from the glucose-indicating polymer anthracene moieties. 26 The sensor contains a light-emitting diode as indicator excitation source and two filtered photodiodes to measure fluorescence intensity (Fig. 1). 26 Therefore, representative substances (e.g., levofloxacin, piroxicam, tetracycline, and quinidine) that absorb or fluoresce light over wavelength ranges that overlap with anthracene absorption or fluorescence were also selected for interference testing. 29
The remaining substances selected for interference testing included several common medications prescribed for the treatment of diabetes, 30 substances examined in prior studies of glucose interference testing, 12,23 –25,31 and those outlined in International Organization for Standardization (ISO) document 15197:2013 (“In vitro diagnostic test systems—requirements for blood glucose monitoring systems for self-testing in managing diabetes mellitus”) 32 or U.S. Food and Drug Administration (FDA) Guidance Document for Blood Glucose Monitoring Test Systems. 10 Because the Eversense CGM sensor is inserted in the subcutaneous space, endogenous species that remain intracellularly localized to blood cells and that do not enter the interstitial space, such as hemoglobin, were not tested as potential interferents.
A full list of the 41 substances (23 exogenous substances, 18 endogenous substances) that were tested is included in Table 1.
In vitro interference testing
The Eversense CGM sensor measures glucose in aqueous media (ISF) when inserted in subcutaneous tissue. 22,26,33,34 In vitro tests were performed in model solutions composed of phosphate-buffered saline (10 mM phosphate buffer solution, NaH2PO4-H2O = 1.90 mM, Na2HPO4-12H2O = 8.10 mM, NaCl = 138 mM, KCl = 2.7 mM, and ethylenediaminetetraacetic acid = 1 mM adjusted to pH 7.4 with HCl or NaOH) and bovine serum albumin (22 mg/mL) that mimic the salt and protein concentrations typical of subcutaneous ISF. 35,36 All tests were performed at two different glucose concentrations (∼77 and 321 mg/dL), except for the sugar alcohols, which were tested at three different concentrations (54, 108, and 270 mg/dL) in response to the recently released FDA Guidance Document for Blood Glucose Monitoring Test Systems. 10 A YSI 2300 STAT Plus glucose analyzer (YSI Life Sciences, Yellow Springs, OH) was used to obtain reference glucose measurements. Tests were conducted in the presence and absence of the potential interfering substance. The concentration at which each added substance was tested for having an interfering effect was based on the guidelines provided in the Clinical and Laboratory Standards Institute (CLSI) document EP7-A2 section 5.5 “Interferent Test Concentrations”; these recommended concentrations vary according to the specific substance, but all substances were tested at a concentration above the highest plasma concentration expected in the intended patient population. 27
Custom test fixtures, each containing a 500-mL fluid reservoir (maintained at 37°C) and capable of measuring data from up to 25 sensors at a time, were used. A paired-sample test design was used in which measurements obtained for each sensor in solutions without potential interferent (“control solution”) were compared with measurements obtained in solutions with the potential interferent (“test solution”). Sensors were equilibrated in each solution for 30–60 min at 37 ± 1°C before sensor data collection.
CGM sensor and YSI reference glucose measurements were obtained for each test condition (i.e., substance and glucose concentration). Data were calculated using the mean of a minimum of 40 sensors (from at least three sensor lots) based on an average of seven readings for each sensor in each test condition. Results at each test concentration were averaged. A test substance was considered to have an interfering effect if test samples met either of the following performance criteria as defined by ISO 15197:2013: (1) for solution glucose concentrations < 5.55 mmol/L (< 100 mg/dL), the average difference in sensor glucose measurements between the test sample and the control sample (“sensor bias”) exceeded 0.55 mmol/L (10 mg/dL); or (2) for solution glucose concentrations ≥ 5.55 mmol/L (≥ 100 mg/dL), the average difference in sensor glucose measurements between the test sample and the control sample exceeded 10%.
Substances identified as having an interfering effect were further tested using an in vitro dose–response method derived from the CLSI document EP7-A2. 27 Dose–response testing typically used three times the therapeutic plasma concentration as the highest concentration tested and ∼0%, 25%, 50%, and 75% of that concentration as intermediate test points to generate a curve. The order at which these concentrations were tested was varied to avoid any confounding effects. Least squares regression was used to fit the data to a dose–response function and to determine the concentration at which the interferent exceeded the bias limits stated in ISO 15197:2013. 32 The Minitab 17 software package (Minitab, Inc., State College, PA) was used to process the data, plot curves with response functions, and calculate 95% confidence intervals around the means. A minimum of 30 sensors from at least three production lots were used for each test.
Results
In vitro screening study
Of the 41 substances tested, eight were identified as potential interferents (i.e., sensor bias exceeded the ISO bias limit) when tested at a concentration substantially more than the highest plasma concentration expected in the intended patient population (Table 1). Most of the exogenous interfering substances identified within this screening experiment were prescription medications (L-DOPA, piroxicam, pralidoxime iodide, and tetracycline), but one of the interferents, salicylic acid (aspirin), is widely available over the counter. The remainder of interferents comprised endogenous substances (i.e., ribose and lactate) and the nonglucose sugar, mannitol.
In vitro dose–response study
Because the screening experiment was performed with supratherapeutic or supraphysiologic plasma concentrations of the substances, the eight substances identified in the screening study were further assessed in an in vitro dose–response study to determine the substance concentration required to reach the sensor bias limit. This concentration was then compared with the maximum therapeutic/physiologic plasma concentration (or, when available in the published literature, the interstitial concentration reported from approved dosing regimens) to assess whether it could represent a clinically relevant sensor interferent. The Eversense sensor is designed for implantation in the subcutaneous space, just beneath the skin, and, therefore, interstitial concentrations, not plasma concentrations, are relevant to assessing potential user risk.
Of the eight substances tested (Table 2), two were shown to exceed the sensor bias limit at test concentrations that were equal to or less than literature-reported therapeutic concentrations, indicating that they might interfere with sensor readings when used at clinically relevant doses; these were tetracycline and mannitol (which exceeded the bias limit at the low but not the high glucose test concentration).
Test results at the high glucose concentration clearly established bias that exceeded within the therapeutic range; therefore, no further tests were conducted.
ISF, interstitial fluid; ISO, International Organization for Standardization.
Discussion
This study showed that among the 41 substances screened at supraphysiologic/supratherapeutic plasma levels in vitro, eight were identified as possible interferents for glucose measurements by the Eversense CGM sensor. A subsequent in vitro dose–response study showed that only two substances (tetracycline and mannitol) interfered when tested at plasma concentrations associated with therapeutic uses. Although the Eversense CGM sensor is implanted into subcutaneous tissue beneath the skin, and thus is exposed to ISF and not blood, specific ISF concentrations of tetracycline or mannitol have not been reported in the literature. Therefore, the literature-reported plasma values were used as exemplary maximum ISF concentrations. For exogenous compounds, interstitial concentrations are sometimes equal to but are most often less than those seen in the plasma. 37 Therefore, the use of reference plasma levels represents “worst case” values in the context of this study, and substances that do not interfere with sensor function when used at reference plasma levels are unlikely to interfere with sensor function in the interstitial space. Since the worst-case tetracycline level did afford significant bias in this study, Eversense CGM users should be cautioned against the use of tetracyclines and should consider other antibiotics instead.
Sugar alcohols (e.g., sorbitol, xylitol, and mannitol) are used as sweeteners in food products that are often targeted to people with diabetes, as their ingestion results in lower increases in serum glucose levels than the ingestion of conventional sweeteners. The FDA recommends testing of glucose measurement devices at sugar alcohol concentrations of 0.09 mg/dL 10 as these levels reflect those potentially resulting from normal dietary consumption of these food products. In this study, none of the sugar alcohols were identified as interferents when tested at that concentration. However, mannitol combined with sorbitol is also used as an irrigation solution during therapeutic transurethral procedures, and use of this solution has been clinically demonstrated to result in plasma concentrations significantly > 0.09 mg/dL. 38 The data in this study suggest that mannitol exceeds the ISO interference bias threshold at concentrations that may be achieved from therapeutic use of this irrigation solution. Given the structural similarity between sorbitol and mannitol, it is prudent to expect that sorbitol will have an interfering effect similar to mannitol. Therefore, Eversense CGM System users should be cautioned against therapeutic uses of irrigation solutions that contain either of those substances.
Of note, acetaminophen and ascorbic acid did not appear to have any significant effect on Eversense CGM sensor bias within the in vitro screening study. This contrasts with the known effect of these substances on other commercially available sensors. Indeed, Basu et al. 39 reported for the Dexcom Seven Plus, Medtronic Diabetes Guardian, and Dexcom G4 Platinum CGM systems that a single 1-g dose of acetaminophen in participants who had plasma glucose levels of 90 mg/dL had sensor measurements that varied over a wide range (85–400 mg/dL). Similarly, FDA-approved package labeling indicates that acetaminophen affects the sensor accuracy of the Dexcom G5 Mobile CGM System, 40 whereas salicylic acid and ascorbic acid affect the sensor accuracy of the Freestyle Libre. 41 Investigators have suggested that acetaminophen and ascorbic acid likely interfere with the electrochemical detection elements (i.e., working electrodes) of those sensors—a mechanism that is qualitatively different from the abiotic, fluorescent glucose-indicating mechanism of the Eversense CGM sensor. Therefore, the lack of interference by these substances may provide an advantage offered by the Eversense CGM System when compared with electrochemical-based CGM systems.
In this study, compounds were selected so as to cover a range of structural classifications. Thus, levofloxacin, piroxicam, tetracycline, and quinidine were tested so as to span the range of wavelengths that may pose potential interference with the fluorescent Eversense sensor. Although it should be recognizable that their test results with these substances cannot be extrapolated to all drugs that fluoresce or that may interfere with signaling through other mechanisms (e.g., fluorescence quenching), these selected compounds were useful in identifying a potential risk area (i.e., compounds that may absorb or fluoresce light across the same wavelength range as tetracycline). Similarly, a wide range of compounds with vicinal diol moieties (i.e., monosaccharides, disaccharides, polysaccharides, sugar alcohols, catechols, alpha-hydroxy carboxylic acids, and aminosugars) were tested to assess the risks of cross-reactivity (vicinal diols are structurally related to glucose); testing revealed a potential risk of cross-reactivity from sugar alcohols at concentrations associated with use of intraoperative irrigation solutions but not at concentrations expected from dietary consumption of these substances. Other classes of compounds frequently prescribed to people with diabetes, such as antihypertensives (e.g., angiotensin-converting enzyme inhibitors, beta blockers, and diuretics) and hypoglycemics (e.g., sodium–glucose cotransporter 2 inhibitors and glucagon-like peptide-1 agonists), are examples of rational candidates for future interference tests.
A notable limitation inherent to an in vitro test of a sensor that is intended for subcutaneous implantation is the use of literature-reported plasma concentrations as representative of “worst-case” ISF concentrations for many of the compounds tested. As mentioned previously, this limitation stems from the absence of literature-reported ISF concentrations for those compounds. The actual concentration of a compound in the subdermal ISF relative to plasma is dependent on drug distribution to the subcutaneous tissue, which, in turn, varies according to the substance's water and lipid solubility and extent of protein binding. Furthermore, use of combinations of drugs that have synergistic or additive pharmacokinetic and/or interference effects may alter those concentrations and/or sensor function, respectively. Consequently, testing was performed at concentrations that are in excess (typically threefold) of maximum literature-reported plasma concentrations, as shown in Table 1, to increase the probability that the concentrations tested are beyond the maximum expected ISF concentrations.
Although in vitro interference tests, such as that used in this study, are not surrogates for in vivo (animal or clinical) investigations, they remain useful tools for the identification and assessment of potential risks and can help guide future studies and the design of new glucose sensors.
Conclusions
The interference profile of the Eversense CGM System is markedly different from enzymatic, electrochemical-based transcutaneous CGM systems. Several substances reported to interfere with those systems (i.e., ascorbic acid, acetaminophen, dopamine, maltose, and xylose) did not affect Eversense readings. However, mannitol and tetracycline exceeded interference test limits at therapeutic concentrations.
Footnotes
Acknowledgments
The authors thank Lynne Kelley, MD, FACS, for valuable discussions throughout the writing of this article. This study was funded by Senseonics, Inc. (Germantown, MD).
Author Disclosure Statement
All the authors are employees of Senseonics, Inc., and have stock options or own stock in the company.