
Abstract
Continuous subcutaneous insulin infusion (CSII) is a widely used treatment for diabetes patients. Insulin infusion sets (CSII-catheters) are continuously optimized regarding size, handling and safety, but recurring dysfunction (kinking or occlusion), due to different user situations, behavior or chain of events, demand new ways to improve the functionality and safety in patients experiencing these issues. A novel CSII-catheter design (Lantern) features additional lateral perforations, which guarantee functionality even in case of kinking or occlusion. This study aimed to compare functionality, insulin distribution, and failure rate of Lantern and standard catheters using excised human adipose tissue samples. Novel Lantern CSII-catheters (open and artificially occluded) and commercially available standard CSII-catheters were inserted into adipose tissue samples. A mixture of insulin and contrast agent was infused as single bolus (7 IU) with an insulin infusion pump at highest flow rate (1 IU/s). Microtomography images and surface-to-volume ratios were used to assess insulin distribution and depot volume indicating the functionality of CSII-catheters. Failure rate was measured by flow-stop alerts of the pump. We found no difference in the volume of insulin depots compared with the nominal volume of 70 μL. Surface-to-volume ratios showed no significant difference among CSII-catheters. None of the catheters triggered any flow-stop alarm. The novel Lantern CSII-catheter design achieved similar insulin distribution as commercially available CSII-catheters. Moreover, functionality of Lantern CSII-catheters was guaranteed during occlusion, which is an improvement compared with standard CSII-catheters. We conclude that the novel CSII-catheter design has the potential to provide a valuable contribution to patient well-being and safety.
Background
Continuous subcutaneous insulin infusion (CSII) therapy using insulin infusion pumps and insulin infusion sets (CSII-catheters) is now common practice for many type 1 and type 2 diabetes patients. 1 –5 CSII-catheters directly connect the infusion pump, which holds an insulin reservoir, to the subcutaneous tissue allowing insulin infusion throughout the day in a controlled way and adapted to the current needs of the patient (e.g., during exercise, at mealtime). The many advantages of CSII therapy include reduced discomfort due to less frequent needle insertion compared with multiple daily injections with insulin pens, and the improved integration into a sportive lifestyle by using short-acting instead of long-acting insulins.
Success of CSII therapy depends greatly on the delivery of the appropriate dose of insulin at the correct time and it is thus dependent on the reliable functionality of the equipment. However, several CSII-catheter–related failures have been discussed recently. 6 –10 One major problem is the occlusion of soft tube catheters by either kinking or crimping, pricking of subcutaneous tissue, and precipitation of insulin or fibrin formation at the catheter tip, 8,11 all of which can prevent the delivery of the correct insulin dose. Many insulin infusion pumps have an embedded alarm system that detects an interruption of insulin delivery when the CSII-catheter is completely blocked. If the CSII-catheter is only partially occluded, the alarm system may not respond, although an insufficient amount of insulin is infused leading to a hyperglycemic event. A partial obstruction of the CSII-catheter can thus lead to an undefined lag time of the insulin bolus delivery and may result in potentially dangerous situations under adverse circumstances. 6 A delayed occlusion alarm is also particularly relevant when only small amounts of insulin are infused as the delay might be far too long and become clinically relevant.
One limitation of currently used CSII-catheters is the single opening at the tip. Kinking and subsequent occlusion or partial occlusion at the opening can cause failure of the entire CSII system. Clogged catheters have to be replaced before the intended wear time of 3 days, leading to discomfort due to additional needle insertions, especially in younger patients.
Novel designs for CSII-catheters are intended to prevent full or partial obstruction of the insulin catheters. One possible design feature is the addition of longitudinal perforations around the circumference of the catheter shaft (Lantern design; Unomedical a/s, Denmark). These perforations provide multiple pathways for the infused insulin in case of kinking or clogging in use situations and thus reduce the need for premature CSII-catheter change, which can substantially contribute to patients' well-being.
In this study, we aimed to compare standard CSII-catheters with Lantern design CSII-catheters regarding failure rate, functionality, and distribution of insulin.
Materials and Methods
Human tissue samples were collected from nine female donors (age 32–57 years) during abdominoplastic surgery. Each donor gave informed consent before surgery. Tissue samples were transferred to our laboratory within 1 h and work on tissue samples started at the latest 4 h postsurgery. Tissue samples were at least 2.5 cm thick to ensure reliable catheter insertion and continuous insulin infusion and to avoid leakage of the infused solution to the bottom of the tissue sample. In total, the study was done using 30 tissue test sections (each 10 × 15 cm).
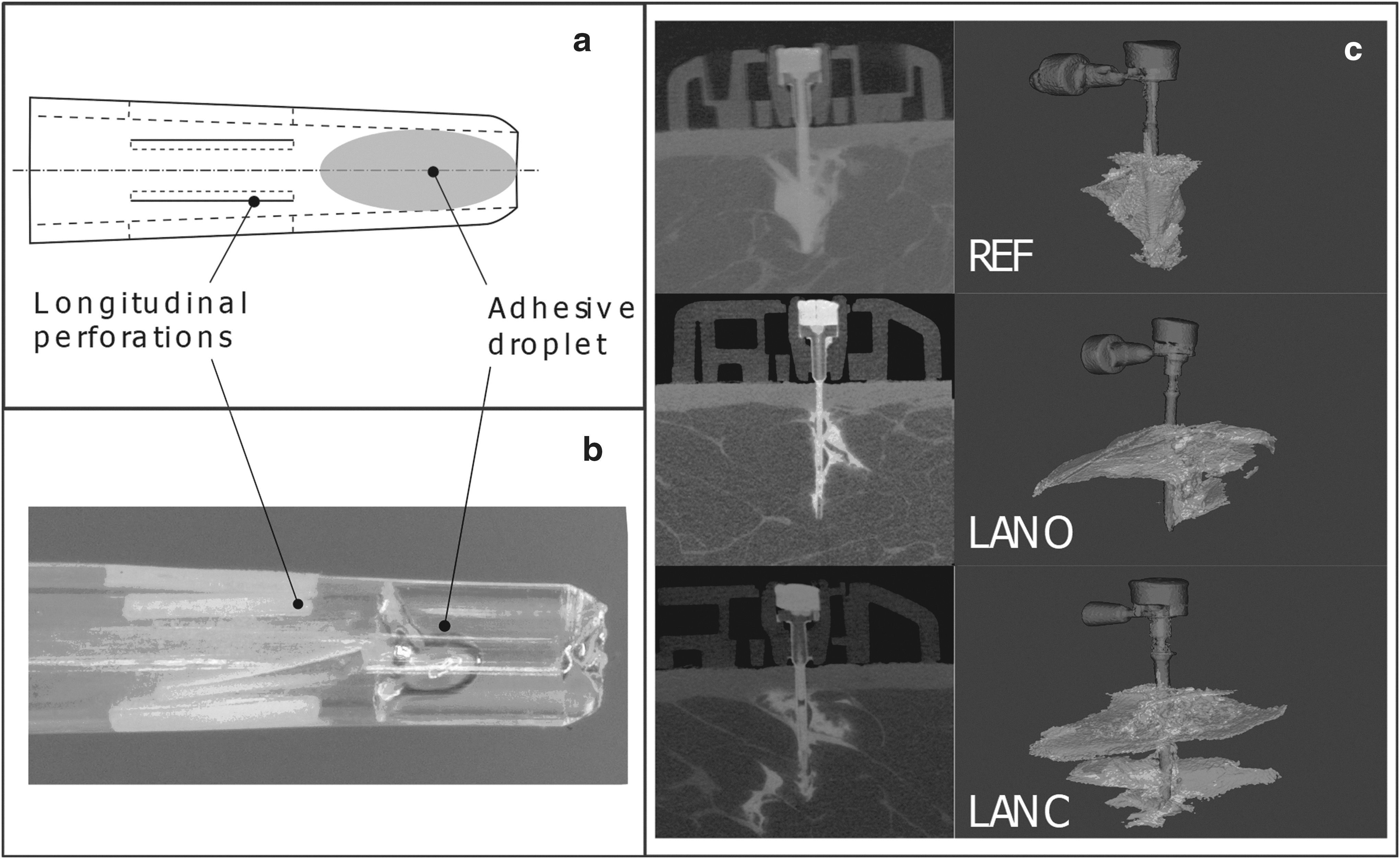
Three different soft CSII-catheters were used, with a length of 9 mm and a 90° angle. A standard catheter (REF, Inset® II catheter; Unomedical a/s) and two new Lantern design catheters (Unomedical a/s): open state (LANO) and clogged state (LANC). LANO has additional longitudinal perforations along the circumference compared with REF. The perforations have a length of 0.5 mm, starting 0.8 mm from the tip of the catheter.
To mimic a clogged catheter (LANC), the tip of a LANO was occluded with a droplet of cyanoacrylic adhesive (Loctite 4304; Henkel®, Austria) and the adhesive was cured by a UV light source (BlueWave 50; Dymax® Germany). We checked under a light microscope to ensure that the tip was fully closed and the adhesive did not occlude the longitudinal perforations of LANC (Fig. 1a, b).
Fresh human tissue samples were pinned on Styrofoam plates to simulate natural skin resistance during needle insertion. A 27 Ga hypodermic needle was used to place the insertion channel for the CSII-catheters. The insertion channel was placed manually by piercing the needle through the dermal layer at ∼3 mm/s. The insertion channel was 10 mm deep to mimic the length of the original needle on the insertion device. Immediately after the insertion channel was placed, we inserted one catheter of each type (REF, LANO, and LANC) into each of the 30 test sections (10 × 15 cm) with a speed of ∼3 mm/s and randomizing catheter placement among the test sections. Hence, each catheter type was tested 30 times. The catheters were then attached to the surface of the tissue sample by adhesive tape.
Each test section was scanned in a small animal computed tomography scanner (μCT; Siemens Inveon MultiModality, USA) using the following parameters: voltage 80 kV, projections 360, current 500 μA, binning 2 × 2, exposure time per projection 900 ms, field of view: 54 × 26 mm, slice thickness: 35 μm, and effective pixel size 35 μm.
An injectable insulin solution (ActRapid®, Novo Nordisk, Denmark) was mixed with a contrast agent (Xentix® 360, Guerbet, France 9 + 1 v/v) and filled into the pump cartridge of an insulin infusion pump (Vibe®, Animas, USA). Interconnecting tubing was prefilled with the infusion mixture. Pump mode of insulin infusion pump was set to standard bolus infusion with 7 IU (70 μL) at an infusion rate of 1 IU/s (10 μL/s). The insulin infusion pump was connected to the CSII-catheters through plastic tubing and infusion was started. Occlusion alerts are triggered when back pressure on the piston exceeds 15 psi (1.03 bar). Each CSII-catheter with a flow-stop alert was to be excluded from scanning and the number of alerts was counted.
Immediately after infusion of the 70 μL bolus, the plastic tubing was disconnected and the tissue sample was moved to the μCT for image acquisition, which took 11 min per catheter. The three CSII-catheters in all 30 test sites were infused and scanned successively to ensure the same amount of time for each infused insulin depot inside the tissue sample. Failure rate was assessed by counting the occlusion alerts of the insulin infusion pump, which uses a pressure sensor to detect occlusions. Images were visually inspected to identify leakage to the surface of the tissue sample. Catheters with leakage to the surface were to be excluded from analysis and the incidence was recorded.
Images were imported into 3D modeling software (Materialise Mimics®, Materialise, Belgium). For identification of infused insulin depot and calculation of surface area (S) and volume (V), attenuation thresholds to distinguish between tissue (−120 to −90 HU) 12 and infused solution were set to 443 HU (lower limit) and 1114 HU (upper limit).
Normal distribution of samples was shown by Shapiro–Wilk test. The surface area-to-volume ratio (SA:V) was calculated by dividing mean S by mean V for each CSII-catheter type (LANO, LANC, and REF). V or SA:V among the catheter types was compared by using a one-way analysis of variance (ANOVA) with significance P-values <0.05.
Results
There was no flow-stop alert of the insulin infusion pump and no leakage to the surface or the bottom of tissue sample when we tested 30 CSII-catheters of each type—90 infusions and μCT scans (Fig. 1c). The overall mean volume of the depot formed in subcutaneous adipose tissue was 68 ± 11 μL (mean ± standard deviation) and we found no significant difference in the mean volume of the insulin infusion mixture depot formed after infusion comparing REF, LANO, and LANC (P > 0.05, Table 1). Also, the overall mean SA:V ratio was 4.3 ± 0.9 with similar values for the three catheter types (P > 0.05, Table 1).
Mean Volume and Mean Surface-to-Volume Ratio of Calculated Depots After Infusion of 70 μL Infusion Mixture
Values are presented as mean and SD for either each CSII type (REF, LANO, or LANC; n = 30 for each type) and as a mean and SD for all CSII-catheters (n = 90).
CSII, continuous subcutaneous insulin infusion; SA:V, surface area-to-volume ratio; SD, standard deviation.
Discussion
In this study, we compared a novel CSII-catheter design (Lantern) with a commercially available CSII-catheter regarding failure rate, functionality and distribution of insulin in human subcutaneous adipose tissue samples. None of the 90 infusions using the tested three catheter types triggered any occlusion alert. However, during preliminary testing of the experimental setup, an occluded standard REF CSII-catheter had immediately triggered an occlusion alert (unpublished data).
In this study, we found no significant difference in the mean insulin volume delivered with either an open or occluded Lantern design catheter compared with a standard REF CSII-catheter. The amount of insulin applied into subcutaneous adipose tissue at a specific time (e.g., before/after meal) is crucial for a successful therapy and thus patient safety. Significant deviations from the necessary dose can lead to life-threatening situations for the patient and can have long-term negative effects on the patient's health. All used catheters in our study showed a successful insulin depot formation after a 70 μL bolus infusion and can thus be described as fully functional. This shows that the occluded Lantern CSII-catheter keeps its functionality even when it is completely sealed at the tip. Furthermore, the spatial distribution of the formed insulin/contrast agent depot quantified by the SA:V ratio was similar among all used catheter types. Thus, the pharmacokinetics of insulin appear not to be influenced by the use of the new Lantern design CSII-catheters. Form and spatial distribution of the insulin depot are influencing the pharmacokinetics of insulin, where a larger surface leads to a faster uptake of insulin into circulation. 13 A significantly altered uptake behavior could influence the dosing regimen of available insulins or it would eventually be necessary to design new insulins with different pharmacokinetic characteristics.
Results of a patient survey showed that the most common reasons for premature CSII-catheter change include kinking (reported by 64.1% of all patients) and blockage (54.3%), which can be caused by a precipitation of insulin. 11 A laboratory study showed that occlusion is less likely within 72 h of CSII-catheter use but getting more frequent with longer wear time of CSII-catheters. 14 Our result clearly indicates that the new Lantern design could be useful in preventing life-threatening situations due to erroneous insulin delivery into tissue as it showed full functionality in human tissue even when catheter tip was artificially occluded. By providing continuously open perforations on the circumference of the catheter close to the tip, additional fluidic paths for the insulin are provided when the main opening is not available. These open perforations ensure distribution of insulin due to the increased back pressure as a result of the increased fluidic resistance when the catheter is kinked or occluded.
Our results with the occluded Lantern catheters showed that the necessary fluidic resistance to deliver insulin through the perforations is below the threshold of the occlusion alert of the insulin infusion pump of 15 psi, as no single alert was recorded. An additional benefit of multiple perforations appears when the catheter hits a solid structure such as the abdominal muscle during insertion or exercise. Lantern is designed to provide a predefined weak point where the catheter is more likely to kink, which automatically activates the perforations and thus a new fluidic path.
Other CSII-catheters with additional openings, such as FlowSmart™ (Becton-Dickinson) with just one single additional round opening, also showed reduced occlusion alerts. 15 This additional opening provides an exit for the infused solution in case of blockage at the catheter tip, presuming the additional opening is not occluded as well or CSII-catheter is not kinked above the additional opening. The advantage of the Lantern design lies in its multiple perforations, which provide additional openings when the catheter is kinked or the tip is occluded. Moreover, the longitudinal design of the additional openings and the fact that more than one opening is available in case of blockage increase the failure tolerance of the Lantern design, as it is highly unlikely that all perforations are blocked along their total length at the same time. As these perforations are normally closed, an ingrowth of tissue is also avoided and blockage by tissue is very unlikely.
Although our results are promising, the study is limited by the use of ex vivo human adipose tissue, which does not allow testing long-term infusion in case of basal rate administration or the influence of blood circulation.
Conclusion
The novel Lantern CSII-catheter is designed to enhance safety and comfort for diabetes patients using CSII therapy, as it provides excellent insulin distribution even when it is kinked or completely occluded at the tip. This should facilitate longer catheter wear time, which reduces discomfort for the user. In addition, the Lantern design could enhance the safety of the patient, as patients do not solely depend on the reliability of the pressure sensor in the insulin infusion pump. Based on our results, we conclude that the novel Lantern CSII-catheter has the potential to provide a valuable contribution to the well-being and safety of diabetes patients.
Footnotes
Acknowledgments
The authors thank Dr. Selma Mautner (Joanneum Research, Health—Institute for Biomedicine and Health Sciences, Graz, Austria, and Medical University of Graz, Division of Endocrinology and Diabetology, Graz, Austria) for critical review and editorial assistance with the article. Furthermore, the authors thank Dr. Johannes Eichler and Ines Anders (Medical University of Graz, Division for Biomedical Research) for their assistance on the μCT.
Author Disclosure Statement
T.A.-K., S.S., and T.B. received honoraria from Joanneum Research. F.S. received honoraria from Joanneum Research and Medical University of Graz. P.K.S. and M.H. received honoraria from Unomedical a/s.
Funding Information
The presented study was funded by Unomedical a/s.