
Abstract
The aim of this study was to determine the role of polymorphic variants of apolipoprotein E (APOE) and peroxisome proliferator-activated receptor delta (PPARD) genes in the development of coronary heart disease (CHD), and the PPARD and APOE gene–gene interaction in a Turkish population. This study was carried out using a sample of 223 patients with CHD (103 with diabetes and 120 without diabetes) and 101 controls. PPARD +294T/C and APOE genotypes were determined by polymerase chain reaction–restriction fragment length polymorphism technique. The PPARD and APOE genotype distributions were the same between study groups (p>0.05). In the nondiabetic CHD patients, the PPARD +294 C allele showed higher serum low-density lipoprotein cholesterol (LDL-C) level than the common +294 TT homozygote genotype (3.83±1.01 vs. 3.33±1.14, p=0.015). In addition, a significant association between APOE 4 and PPARD +294 C alleles was detected based on their effects on LDL-C in the nondiabetic CHD patients (+294 C/APOE4: 4.43±0.88 vs. +294 TT/nonAPOE 4: 3.48±1.09, p=0.009). This association indicated the interaction of two genes on plasma LDL-C levels ascended in the order +294 T<+294 T-APOE 4<+294 C<APOE 4<+294 C-APOE 4. The PPARD +294 C allele was associated with higher incidence of left ventricular hypertrophy (LVH) in all male patients with body mass index >27. In addition, the CHD patients who were +294 C allele carriers had a 2.48-fold higher risk of LVH than subjects homozygous for the T allele. An increasing effect of the PPARD +294 C allele was shown on serum LDL-C levels in nondiabetic CHD patients. In addition, the results suggested that the +294 C allele might be associated with an increased LVH risk especially in male CHD patients. Furthermore, gene–gene interaction between the PPARD +294T/C and the APOE polymorphisms was observed regarding LDL-C concentrations.
Introduction
Peroxisome proliferator-activated receptors (PPARs), a member of the nuclear receptor superfamily located on chromosome 3p25, are transcription factors that control various important metabolic pathways such as glucose homeostasis, lipoprotein metabolism, fatty acid catabolism, adipogenesis, vascular homeostasis as well as suppression of inflammation, free radical generation, smooth muscle cell growth, and atherosclerosis (Duval et al., 2002; Balakumar et al., 2007; Libby and Plutzky, 2007). To date, three isoforms of PPAR (PPAR-alpha, -delta, and -gamma), encoded by separate genes and expressed by different tissues, have been identified (Duval et al., 2002; Marx et al., 2004; Kota et al., 2005; Tesse et al., 2009). Although PPAR-alpha and PPAR-gamma have been widely studied, the functional identification of PPAR-delta remains unclear. PPAR-delta is ubiquitously expressed (Kota et al., 2005) and has a pivotal role in the regulation of apoptosis, cell proliferation, and fatty acid catabolism (Tesse et al., 2009). Recent studies reported that beneficial metabolic effects of PPAR-delta agonists on lipid profile, atherosclerosis, obesity, and insulin resistance may be a result of increased fatty acid catabolism, cholesterol efflux, energy expenditure, and oxidative capability in the muscle (Dressel et al., 2003; Tanaka et al., 2003).
A common T294C polymorphism has been identified at position +294 in the 5′-UTR of PPAR-delta gene (PPARD) (Skogsberg et al., 2003a). Previous studies showed an association between the rare +294 C allele and cardiovascular risk factors such as increased low-density lipoprotein cholesterol (LDL-C) levels, elevated apolipoprotein B levels, body mass index (BMI), and decreased serum levels of high-density lipoprotein cholesterol (HDL-C) (Skogsberg et al., 2003b; Chen et al., 2004; Aberle et al., 2006a; Aberle et al., 2006b; Nikitin et al., 2010). However, some studies have yielded conflicting results (Skogsberg et al., 2003b; Gouni-Berthold et al., 2005; Robitaille et al., 2007; Jguirim-Souissi et al., 2010).
Another well-known candidate gene for the development of CHD is APOE, which encodes apolipoprotein E (ApoE), the apoprotein of LDL and very low density lipoprotein (VLDL). ApoE is an important glycoprotein that removes remnants of chylomicron and VLDL in the plasma, which creates a direct impact on lipid metabolism (Mahley, 1988). The Epsilon (ɛ) polymorphism (ɛ3, ɛ2, and ɛ4) in the APOE gene results in three different alleles that encode the three isoforms of ApoE, that is, ApoE2 (Cys 112/Cys 158), ApoE3 (Cys 112/Arg 158), and ApoE4 (Arg 112/Arg 158). ApoE2, E3, and E4 have different affinities for LDL receptor thus resulting in different serum lipoprotein levels. Previous studies have shown that ɛ4 allele was associated with increased blood levels of LDL-C and triglyceride (TG) and therefore this allele seems to be a risk factor for atherosclerosis and CHD. In addition some reports revealed that the regulation of lipid metabolism by E4 allele might be modified by the other genes or environmental interactions (Ashavaid et al., 2003; Loew et al., 2005).
The focus of this study is to investigate the polymorphic variants of APOE and PPARD genes in the development of CHD, and to determine the PPARD and APOE gene–gene interaction.
Materials and Methods
Study participants and clinical investigation
The PPARD +294T/C and APOE gene polymorphisms were studied in 103 diabetic and 120 nondiabetic cases of CHD. Patients with severe coronary vascular disease were documented by angiography. The presence of CHD was estimated according to previous medical history, present symptoms of angina pectoris, and electrocardiogram (ECG) changes. Height and weight was measured and BMI was calculated; obesity was considered present if the BMI exceeds 26.7 in men or 27.3 in women (roughly 30% above ideal weight). Angiographic inclusion criteria were ≥50% stenosis of at least one major coronary vessel because of atherosclerosis, or a vascular event, defined as myocardial infarction, percutaneous transluminal coronary angioplasty, or coronary artery by-pass grafting. Clinical diagnoses of left ventricular hypertrophy (LVH) were based on echocardiographic and ECG criteria, according to the guidelines of the American Society of Echocardiography (Sahn et al., 1978). A total of 101 volunteers were used as controls. Healthy persons without any symptoms of both CHD diabetes mellitus, infectious disease, or any systemic disease were selected for the control group. Coronary angiography was not performed on these individuals, and therefore the presence of atherosclerotic coronary arteries could not be excluded. However, none of these individuals had a history of a vascular event.
The study protocol was approved by both the Ethical Committee of the Istanbul Faculty of Medicine and the Research Fund of Istanbul University. All participants in the study signed informed consent forms in accordance with ethics guidelines regarding the study.
Lipid measurement
Blood samples were drawn into plain tubes after the participants had fasted overnight. The samples were centrifuged for 10 min at 1500×g at room temperature and the serum was immediately removed and frozen at −20°C. Total-cholesterol levels were measured by cholesterol oxidase-peroxidase-aminoantipyrine (CHOD-PAP) enzymatic calorimetric test. Serum HDL-C levels were measured by CHOD-PAP test following precipitation of apolipoprotein B–containing lipoproteins with phosphotungstic acid and magnesium ions. The glycerol phosphate oxidase-peroxidase-aminoantipyrine enzymatic calorimetric test was used to measure serum TG levels. Serum LDL-C levels were calculated using the Friedewald formula.
Genotyping
Genomic DNA was extracted from human leukocyte nuclei isolated from whole blood by standard methods. Polymerase chain reaction–restriction fragment length polymorphism and agarose gel electrophoresis techniques were used to determine PPARD +294T/C and APOE (E3, E2, and E4). After amplification of the isolated DNA with PCR, the PPARD and APOE polymorphisms were detected by digesting the PCR product with the restriction endonucleases Bsl1 (MBI Fermentas) (Gouni-Berthold et al., 2005) and Hha1 (MBI Fermentas) (Kontula et al., 1990), respectively. The digested DNAs were separated on 3% agarose gel in 1X Tris borate EDTA buffer followed by staining with ethidium bromide solution. The genotypes were typed by visualization under ultraviolet light. Automated sequencing and real-time PCR were used to confirm the results of PPARD +294T/C and APOE polymorphisms for a subset of 20 representative samples, respectively. Results between PCR and DNA sequencing analysis were 100% concordant.
Statistical methods
Statistical analysis was performed by using SPSS software package program (revision 11.5; SPSS, Inc.). Clinical laboratory data are expressed as mean±SD. Mean values were compared between patients and controls by unpaired Student's t-test. Differences in the distribution of genotypes and alleles between cases and controls were tested using the chi-square statistic. Allele frequencies were estimated by gene counting methods. Values of p<0.05 were considered statistically significant. Statistical power calculations were performed with PS software, version 3.0 (Dupont and Plummer, 2009).
Results
Clinical investigation
Demographic, biochemical, and clinical characteristics are summarized in Table 1. There were no significant differences between the patients with or without diabetes and control groups, when age distributions were analyzed.
DM (+) CHD, coronary heart disease (CHD) patients with diabetes; DM (−) CHD, CHD patients without diabetes; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; LVH, left ventricular hypertrophy; n, number of individuals; p1, control versus DM (−) CHD; p2, control versus DM (+) CHD; p3, DM (−) CHD versus DM (+) CHD.
As expected, patients showed a significantly higher prevalence of traditional cardiovascular risk factors with respect to healthy subjects. Total-cholesterol (p<0.01), BMI (p<0.05), systolic blood pressure (SBP) (p<0.05) and diastolic blood pressure (DBP (p<0.05), and smoking (p<0.001) were found to be higher in nondiabetic CHD patient group than the controls, while HDL-C level (p=0.01) was found to be lower in nondiabetic CHD patient group than the controls.
In diabetic CHD patient group when compared with controls, a higher prevalence of conventional risk factors for CHD was observed, including high levels of SBP, DBP, VLDL-C, and lower levels of HDL and smoking (p<0.05). On the other hand, TG, LDL-C levels, obesity, and family history were not significantly different (p>0.05).
However, a higher ratio of male gender (p<0.01), total-cholesterol (p<0.01), LDL-C (p<0.01), HDL-C (p<0.05), smoking (p<0.001), and a lower mean age (p<0.01) in nondiabetic CHD patient group was found when compared with the diabetic CHD patient group.
PPARD +294T/C and APOE genotypes and allele distribution
The allelic and genotypic frequencies of PPARD +294T/C and APOE polymorphisms were not significantly different between the study groups (p>0.05) (Table 2). The frequency of all alleles and genotypes in the study groups was distributed according to Hardy–Weinberg equilibrium (p>0.05).
DM (+) CHD, diabetic CHD group; DM (−) CHD, nondiabetic CHD group; p1, control versus DM (+) CHD; p2, control versus DM (−) CHD; p3, control versus total patient; p4, DM (+) CHD versus DM (−) CHD; FE, Fisher's exact test.
The frequencies of PPARD +294 TT, CC, and TC genotypes among the diabetic CHD patients were 0.553, 0.068, and 0.379, respectively; among the nondiabetic CHD patients the frequencies were 0.525, 0.083, and 0.392, respectively, and among the control subjects, they were 0.554, 0.03, and 0.416, respectively (p>0.05).
The frequencies of APOE alleles E2, E3, and E4 among the diabetic CHD patients were 0.0582, 0.849, and 0.092, respectively; among the nondiabetic CHD patients the frequencies were 0.0583, 0.837, and 0.104, respectively, and among the control subjects, they were 0.049, 0.876, and 0.072, respectively (p>0.05).
Association of the PPARD +294T/C and APOE polymorphisms with lipid and metabolic parameters
To assess whether these polymorphisms had any effect on lipid and metabolic parameters, the baseline characteristics among the genotype groups in the controls and patients with or without diabetes were compared (Table 3). The serum TG level in controls carrying ApoE 2 allele was found to be higher (p=0.011). However, this association was not observed in the other study groups (p>0.05). In the nondiabetic CHD patients, subjects with the PPARD +294 C allele (CC+CT genotypes) showed a higher serum LDL-C concentrations than with the PPARD +294 TT homozygote genotype (3.83±1.01 vs. 3.33±1.14, p=0.015). Power analysis for association of PPARD +294 polymorphism and serum LDL-C levels was calculated to be 96.2% in nondiabetic CHD group. These findings supported the hypothesis of the PPARD +294 C allele having a detrimental effect on the serum lipid profile in patients with CHD.
DM (+), CHD patients with diabetes; DM (−) CHD, CHD patients without diabetes; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; TG, triglyceride. The results are shown as mean±SD.
p<0.05.
The nondiabetic CHD patients were divided into two allele combination groups according to the presence of APOE 4 and PPARD +294 C and the mean values of the serum lipids were compared. In the nondiabetic CHD patients, serum LDL-C levels of the PPARD +294 C/APOE 4 subgroup were significantly higher than the PPARD +294 TT/nonAPOE 4 subgroup (4.43±0.88 vs. 3.48±1.09, p=0.009) (Fig. 1). Also, the findings of this study have showed that both polymorphisms were associated with the serum LDL-C levels, which were increased in the order of +294 T<+294 T/APOE 4<+294 C<APOE 4<+294 C/APOE 4 (for LDL-C levels, +294 T: 3.51±1.08; +294 T/APOE 4: 3.82±1.30; +294 C: 3.83±1.01; APOE 4: 3.89±1.26; +294 C/APOE 4: 4.43±0.88) in the nondiabetic CHD patients. There was no significant difference in the remaining lipid parameters among the APOE4-PPARD +294T/C allele combinations in both patient groups (with and without diabetes). The increasing effect of the +294 C allele on serum LDL-C levels was observed in nondiabetic CHD patients and this effect was strengthened with the presence of APOE 4 allele (+294 C allele: 3.83±1.01→+294 C/APOE 4: 4.43±0.88).
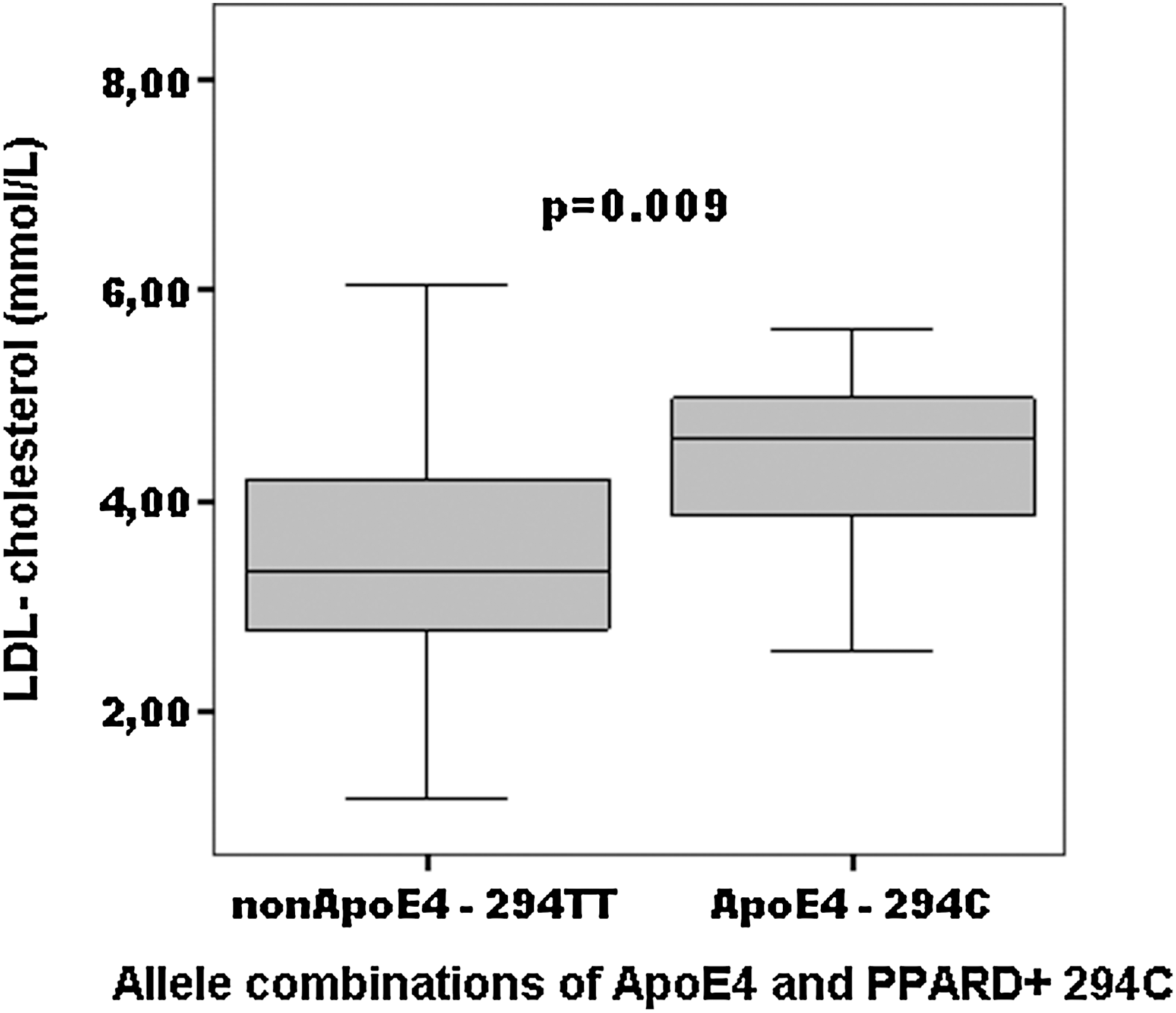
Mean values for serum LDL-C levels according to allele combinations of Apolipoprotein E4 and PPARD +294C in the CHD patients without diabetes. Serum LDL-C levels of the ApoE 4-294 C subgroup was significantly higher than the nonApoE 4-294TT subgroup (p=0.009).
As shown in Table 4, the effects of the interaction of PPARD +294T/C and the APOE polymorphisms on serum lipid levels in CHD patients with and without diabetes mellitus in different sex groups were investigated. The serum LDL-C level was found to be higher in nondiabetic CHD female patients carrying both +294 C and APOE 4 alleles than nondiabetic female patients in the +294 TT/nonAPOE 4 genotype subgroup (5.03±0.43 vs. 3.49±0.18, p=0.002). This combined effect of PPARD +294 C allele and APOE 4 allele on serum LDL-C levels was not found in male nondiabetic CHD patients (p>0.05). However, in male nondiabetic CHD patients, subjects with the rare PPARD +294 CC homozygote genotype showed higher serum LDL-C concentrations than with the wild type PPARD +294 T allele (TT and CT genotypes; p=0.051). Also, the +294 C allele was associated with increased serum LDL-C levels compared with wild type +294 TT homozygote genotype in the CHD male patients without diabetes (p=0.052).
For bold values:
a APOE 4-294 C versus nonAPOE 4-294 TT, p=0.002.
+294 CC+TC versus +294 TT, p=0.052.
+294 CC versus +294 TT+TC, p=0.051.
When the effects of the PPARD +294T/C genotypes on presence of LVH in total CHD patients (diabetics and nondiabetics) with BMI ≥27 were examined, the incidence of LVH was found to be higher in the male patients with the +294 C allele (CC+CT genotypes) as compared with TT genotypes. The +294 C allele significantly increased the risk of LVH when compared with the TT genotype carriers in CHD patients (with and without diabetes) (OR=2.48, 95%CI: 0.917–6.751, p=0.021, statistical power=78%; Table 5).
Statistical analysis was performed using chi-square test. The results are shown as n, %. LVH (+), presence of left ventricular hypertrophy; LVH (−), absence of left ventricular hypertrophy; n, is number of individuals.
p=0.021, χ 2=5.29, OR=2.48 (95% CI: 0.917–6.751).
Discussion
Hyperlipidemia is the primary risk factor of atherosclerosis and CHD (Marenberg et al., 1994; Wilson et al., 1998). In the past 20 years, extensive studies have been conducted on the genes that coordinate cholesterol levels. PPARs are transcriptional factors that regulate fatty acid and carbohydrate metabolisms and are dietary lipid sensors. PPAR-delta plays a role in lipid metabolism by stimulating fatty acid oxidation in heart and skeletal muscle cells (Gilde et al., 2003; Yilmaz-Aydogan et al., 2011).
Animal studies have shown that PPAR-delta functions in cholesterol metabolism in which selective PPAR-delta agonist decreases plasma TG concentrations and the fraction of LDL-C, and increases HDL-C in obese rhesus monkeys (Leibowitz et al., 2000; Dressel et al., 2003; Gilde et al., 2003). Thus PPAR-delta agonists have been defined as a therapeutic target for obesity, insulin resistance, and dyslipidemia.
Recently, a common T294C polymorphism has been identified at position +294 in the 5′-UTR exon 4 of the PPAR-delta gene (PPARD) influencing the expression of PPAR-delta by changing the sequence of the DNA binding site for transcription factor Sp-1. Transient transfection assays revealed that the +294 C allele has higher transcription activity suggesting a greater PPAR-delta activity (Skogsberg et al., 2003a).
This study is the first one conducted on the Turkish population that shows the association between PPARD +294 T gene polymorphism and the risk of CHD development. In this study, individual allele and genotype frequencies of PPARD +294T/C and APOE polymorphisms were not significantly different between the study groups. However, serum TG levels were significantly higher in control subjects with the APOE 2 allele than those with the nonAPOE E2 (2.53±1.63 vs. 1.55±0.76, p<0.05). With respect to the effect of PPARD +294 polymorphism on serum lipids, the most important finding was that the rare PPARD +294 C allele may cause an increase on the LDL-C levels in nondiabetic CHD patients. The effect of the +294 C allele on serum LDL-C concentrations was much stronger in men (p=0.052), although females showed a similar nonsignificant trend (p=0.167), and was significant in the whole nondiabetic CHD group, when men and women were combined (p=0.015).
These results of the effects of PPARD +294T/C polymorphism on the distribution of lipid/lipoprotein profiles, particularly on LDL-C, were in accordance with Skogsberg et al. (2003a), Chen et al. (2004), Aberle et al. (2006a), Aberle et al. (2006b), and Nikitin et al. (2010), but not Skogsberg et al. (2003b), Gouni-Berthold et al. (2005), Robitaille et al. (2007), and Jguirim-Souissi et al. (2010). Little is known about the association of the PPARD +294T/C polymorphism with the serum lipids and the results are controversial. Aberle et al. (2006a) reported a trend toward higher VLDL-C and LDL-C levels in female +294 C allele carriers. They reported a significant relationship between low plasma concentrations of HDL-C and the rare +294 C allele. In addition, they found a significant association between the +294 C allele and elevated BMI values in CHD patients. The investigators have also shown that higher cardiovascular risk was mediated by impaired lipid metabolism and hyperlipidemia, and concluded in their study that this polymorphism was associated with lipid profiles in CHD females (Aberle et al., 2006a). In another study of Aberle et al. (2006b) it was suggested that PPARD had an involvement in the regulation of BMI. In the current study, no association was observed between the alleles of PPARD and BMI.
Skogsberg et al. (2003a) previously reported the similar results with Aberle et al. (2006a) observed in men. Skogsberg et al. (2003a) reported higher plasma LDL-C concentrations in subjects carrying the C allele in human monocyte cell lines, while there were no associations with HDL-C levels. On the other hand, another study by Skogsberg et al. (2003b) reported the results of WOSCOPS trial that indicates that in Scottish men with normal BMI, the PPARD polymorphism had no effect on LDL-C concentrations but was associated with lower HDL-C levels. Chen et al. (2004) reported that PPARD +294T/C polymorphism might have deleterious effects on plasma lipid concentrations as well as coronary lesions.
Robitaille et al. (2007) demonstrated that female patients with metabolic syndrome (MS) and carrying the +294 C allele had higher plasma HDL-C levels and lower total-cholesterol/HDL-C ratio than those with homozygote for the common T allele. However, they could not find any association between PPARD +294T/C and serum lipoprotein levels in males (Robitaille et al., 2007).
Nikitin et al. (2010) reported that the C allele and CC genotype of the PPARD +294 polymorphism were associated with increased risk of coronary artery disease (CAD; OR of 2.12 and 2.78, respectively), while the +294 T variant of PPARD was related to reduced CAD risk (OR=0.47) in the Russian population. They also showed a relationship between the +294 C allele and increased LDL-C levels in controls (Nikitin et al., 2010).
Jguirim-Souissi et al. (2010) found that the C allele was significantly more frequent in patients with CAD than in controls (p<0.001) in Tunisians. On the other hand, they found that the presence of the C allele had no effect on total-cholesterol, TG, HDL-C, LDL-C, and BMI levels, both in patient and control groups (Jguirim-Souissi et al., 2010). Also, Gouni-Berthold et al. (2005) analyzed PPARD +294T/C polymorphism in diabetic patients, and found no significant association with plasma lipoprotein levels (Loew et al., 2005).
Many studies assessing the role of APOE genetics on plasma lipid profiles have shown that the presence of the APOE4 allele is associated with elevations in plasma levels of LDL-C, which suggests a relationship with the development of CHD, while the presence of APOE 2 is associated with decreased levels of LDL-C (Wilson et al., 1996; Lahoz et al., 2001; Yilmaz et al., 2001; Ashavaid et al., 2003; Peng et al., 2003; Loew et al., 2005). Peng and Pederson suggested that the effect of APOE genotype on lipid metabolism might be subjected to further modifications caused by other genes (Pedersen and Berg, 1989; Peng et al., 2003). Peng et al. (2003) reported the gene–gene interaction effect of APOE 4 and PPAR-gamma CT loci on serum cholesterol and CHD.
In the current study, no association was observed between APOE polymorphism and risk of CHD development. In addition, no relation between APO alleles and serum lipoprotein levels was found in the CHD patients with or without diabetes. However, elevated plasma levels of LDL-C were observed in nondiabetic patients carrying both +294 C and APOE 4 alleles (p=0.009). These findings suggest that both polymorphisms are associated with the serum LDL-C levels, which are increased in the order +294 T<+29 4T/APOE 4<+294 C<APOE 4<+294 C/APOE 4 in nondiabetic CHD patients. In addition, this combined effect of the PPARD +294 C allele and APOE 4 allele on serum LDL-C levels was found in female CHD patients without diabetes. The interaction of PPARD and APOE genes on serum lipid levels was evaluated by Aberle et al. (2006a). The allelic variations of APOE were related with the plasma concentrations of total-cholesterol, LDL-C, and ApoB in both men and women. However, Aberle et al. (2006a, 2006b) have not shown the interaction between PPARD and APOE genes.
We observed that the PPARD +294 C allele is associated with higher incidence of LVH in male patients in the current study. In addition, for the whole CHD patient group (diabetics and nondiabetics), +294 C allele carriers had a 2.48-fold higher risk of LVH than subjects homozygous for T allele. Yan et al. (2005) previously investigated the relationship between PPARD +294T/C gene polymorphism and lipid profile, obesity, and LVH in patients with MS. They reported an association between +294 C allele and LVH in their MS group.
The findings in this study suggest that PPARD 294T/C polymorphism and the interaction of PPARD and APOE genes are associated with the risk of CHD development. This effect could be mediated through plasma lipid and lipoprotein levels, which may influence the atherosclerotic process through mechanisms involving foam cell formation. In this study, the statistical power for PPARD +294 polymorphism and serum LDL-C levels was calculated as 96.2% (α=0.05) in nondiabetic CHD group. The statistical power for the PPARD +294 C allele was 78.0% (α=0.05) in the BMI ≥27 subgroup of male CHD patients with LVH. Our findings are closely tied to an adequate statistical power. Therefore, we feel that an increase on the sample size may help to attain equivalent statistical power.
Conclusion
The current study is a preliminary study to establish whether PPARD and APOE polymorphisms have individual or mutual effects in the pathogenesis of CHD in the Turkish population. In this study, the PPARD +294 C allele was associated with increased serum LDL-C levels and an increased risk of LVH in nondiabetic CHD patients that might contribute to the development of CHD. In addition, a significant association between APOE 4 and PPARD +294 C alleles was detected with respect to their effects on CHD. This association indicated the interaction of two genes on plasma LDL-C levels. There was a gene–gene interaction between the PPARD +294T/C polymorphism and ApoE polymorphism in relation to LDL-C concentration.
Footnotes
Acknowledgment
The present work was supported by a grant from the Scientific Research Projects Coordination Unit of Istanbul University (Project No: 946).
Disclosure Statement
No competing financial interests exist.