
Abstract
Recently, eotaxin–CCR3 was reported to play an important role in choroidal neovascularization (CNV) development and was documented to be superior than vascular endothelial growth factor-A treatment when tested in CNV animals. As eotaxin studies are lacking in the human age-related macular degeneration (AMD) patients, we sought to determine whether eotaxin-2 (CCL24) has any association with inflammatory processes that occur in CNV. CCL24 levels were determined by enzyme linked immunosorbant assay (ELISA) after normalization to total serum protein and levels of ELISA were correlated to various risk factors in about 133 AMD patients and 80 healthy controls. The CCL24 levels were significantly higher in wet AMD patients as compared with dry AMD and normal controls. There was a significant difference when compared among wet AMD patients (i.e., minimally classic, predominantly classic, and occult). We also report significant difference in the CCL24 levels of Avastin-treated and untreated AMD patients. This study shows that CCL24 levels were found to be significantly increased in AMD patients despite Avastin treatment as compared with normal controls and those without Avastin, indicating that CCL24 may have an association with CNV and may be an important target to validate future therapeutic approaches in AMD in tandem with Avastin treatment.
Introduction
We hypothesized that CCL24 is also involved in similar processes that result in chronic inflammation by sustained activation of complement system contributing to the pathogenesis of AMD. This CCL24 is located on human chromosome 7. Takeda et al. (2009) had recently shown that the CCL11 and CCL24 protein levels increased in wild-type mice after laser injury and the CCL11 and CCL24 neutralizing antibodies are more effective than VEGF-A neutralizing antibodies (68.63% vs. 57.64%) at inhibiting laser-induced CNV in mice, indicating their causal role in pathogenesis of AMD. They showed that eotaxin–CCR3 signaling has an active role in CNV: in vitro, eotaxin–CCR3 stimulates proliferation of human choroidal endothelial cells, and in a mouse model of CNV involving laser injury to the eye, intraocular administration of eotaxin and CCR3-specific neutralizing antibodies or a small inhibitor molecule reduces the laser-induced pathology. Further, genetically engineered mice that were deficient in eotaxin or its receptor CCR3 were also protected to some extent from the effect of laser injury on the choroidal vasculature. It was also reported that the mRNA for ligands of CCR3 (CCL11, CCL24, and CCL26) was increased in response to hydrogen peroxide challenge (Wang et al., 2011). Another contradictory report sought to dispel any association of AMD with CCR3. Li et al. (2011) provided evidence from animals that VEGF-A neutralizing antibodies significantly suppressed CNV as compared with CCR3, thus playing no significant role in CNV development. We therefore estimated the expression of CCL24 in the serum of human AMD patients which was previously shown as constitutively expressed eosinophil chemokine likely to be involved in homeostatic, allergen-induced, and IL-4-associated immune responses (Zimmermann et al., 2000).
Materials and Methods
Ethical clearance
Ethical clearance was obtained for this study by the Institute Ethics Committee, Postgraduate Institute of Medical Education and Research, Chandigarh, India (vide letter No. Micro/10/1411). Informed consent was obtained in the prescribed format endorsed by the Institute Ethical Committee.
Inclusion and exclusion criteria
Fifty years or older AMD patients with the diagnosis of advanced AMD as defined by geographic atrophy and/or CNV with drusen more than 5 in at least one eye were included in the study. The controls in the study included those above 50 years with no drusen and absence of other diagnostic criteria for AMD.
The exclusion criteria included the retinal diseases involving the photoreceptors and/or outer retinal layers other than AMD loss, such as high myopia, retinal dystrophies, central serous retinopathy, vein occlusion, diabetic retinopathy, uveitis or similar outer retinal diseases that have been present prior to the age of 50 and opacities of the ocular media, limitations of pupillary dilation, or other problems sufficient to preclude adequate stereo fundus photography. These conditions include occluded pupils due to synechia, cataracts, and opacities due to ocular diseases.
Ophthalmic examination
All the patients were examined by a retina specialist for best corrected visual acuity, slit lamp biomicroscopy of anterior segment, and dilated fundus examination. All AMD patients were subjected to fluorescein fundus angiography (FFA) and optical coherence tomography. The diagnosis of AMD was based on ophthalmoscopic and FFA findings. AMD patients were divided into wet and dry AMD patients. Wet AMD patients were further divided into minimally classic AMD, predominantly classic AMD, and occult AMD (Shah and Del Priore, 2009).
Serum separation
About 4.0 mL of blood sample was collected and left for 1 h at 37°C to allow it to clot and serum was subsequently separated in serum separator tube (BD Biosciences) after centrifugation at 3000 rpm for 30 min.
Total protein estimation
Total protein was estimated using Bradford assay. The estimation of total protein was performed according to manufacturer's recommendations. Briefly, serum samples were diluted 1500 times in double-distilled water. Bovine serum albumin (BSA) served as the standard. Diluted samples and BSA standard protein were mixed with coomassie brilliant blue G-250 dye (Bradford reagent) in 4:1 ratio followed by incubation at room temperature for 10–15 min. The absorbance was read at 595 nm in Microplate reader (680XR; BioRad). The standard curve of BSA was estimated with linear or quadratic fit models.
Eotaxin quantitation
The expression of CCL24 was analyzed using commercially available enzyme-linked immunosorbant assay (RayBio; Cat. No. ELH-Eotaxin2-001) as per manufacturer's protocol and absorbance was read at 450 nm using 680XR model of Microplate reader (BioRad). Sample assays were performed in duplicate. This assay recognizes recombinant and natural human CCL24 with detection range of 0.87–5.2 pg/mL. The linear regression analysis was used to generate the standard curve for CCL24 estimation in both patients and controls. All the values were normalized to total serum protein.
Demographic characterization
A trained staff interviewed all subjects using a standardized risk factor questionnaire. A written informed consent form signed by each participant, which included the written risk factor questionnaire, was taken from each participant. The risk factor questionnaire included information about demographic characteristics, cigarette smoking, alcohol intake, and others. Smokers were defined as having smoked at least one cigarette per day for at least 6 months and segregated into smokers and nonsmokers. Hypertension was defined as systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg at examination, or diagnosed by a physician previously and self-reported by the participant's responses to whether a physician had ever informed them of this diagnosis and whether they had ever taken medications for this condition. Similar protocols have been used earlier in previous studies (Tin et al., 2002). Subjects were also asked to report any prior diagnosis of stroke, use of antihypertensive medications, diabetes, migraine, and history of heart diseases.
Statistical analysis
The study was analyzed in three phases. In the first phase, 79 subjects were recruited during the year of 2008–2009 for preliminary study, which included 47 AMD patients (32 wet and 15 dry patients) and 32 controls. Later, the second phase of the study was initiated by including additional 134 subjects during the year of 2009–2011; this included 86 AMD patients (23 dry AMD and 63 wet AMD) and 48 healthy controls. Out of 86 AMD and 48 control samples, about 4 samples were destroyed due to unforeseen reasons, including handling or delayed refrigeration.
The statistical analysis for this study was executed at three stages. First stage or Phase I stage analysis was mainly confined to assess the significant variation of the eotaxin-2 levels between AMD and control subjects along with the role of hypertension in moderating eotaxin-2 levels. The data were thus analyzed using independent t-test and analysis of variance (ANOVA) with post hoc analysis at 5% level of significance under the pretext objectives, whereas descriptive statistics was represented by scatter diagram and table. Second stage or Phase II analysis was also conducted in a similar fashion. However, the final analysis was based on complete data of 213 observations that included 38 dry AMD, 95 wet AMD, and 80 healthy controls. The final analysis included 184 observations, because 29 observations had to be abandoned as one or more observations of particular variables were missing. Under this study, almost all probable risk factors of AMD were recorded for each patient/control, which has been included in the extended analysis. Descriptive study in the final analysis is presented using tabular and graphical methods using appropriate measures of central tendency/dispersion based on the nature of variables. To obtain the most significant factor that influenced the CCL24 levels, a linear model was applied using CCL24 as dependent variable and other factors as independent variables. All statistical analyses were performed in R version 2.13.0 (2011-04-13).
Results
Phase I study was performed to validate the hypothesis whether levels of CCL24 are associated with AMD pathogenesis in patients of Indian origin. The outcome of the study endorsed the hypothesis at 5% level of significance. Hence, the study was extended in Phase II and Phase III including additional patients and controls. Therefore, the study was conducted in three phases in order to validate the new findings and accord significance to the results. The demographic details of all AMD patients and controls are reproduced in Table 1.
Age, age of onset; values are mean±SD or (percentage). AMD subjects were asked to provide all clinical and demographic details at the age of disease onset.
Duration of disease is the interval between appearance of first symptom of AMD and collection of sample.
Unpaired, independent 2-tailed Student's t-test analysis showed that mean age differs significantly among the groups (p=0.02).
AMD, age-related macular degeneration.
Levels of CCL24 in AMD and controls
The role of CCL24 in pathogenesis of AMD patients became apparent after completion of all phases of analysis. ANOVA followed by Fisher's least significant difference post hoc analysis showed that CCL24 levels were significantly elevated in wet AMD (0.0236 pg/μg) patients as compared with the dry AMD (0.0167 pg/μg) and controls (0.0130 pg/μg) (Table 2; Fig. 1A–C and Fig. 3; p=0.02 and p=0.0001, respectively). Parametric unpaired, independent 2-tailed Student's t-test revealed significant difference in CCL24 levels between AMD patients (0.0216 pg/μg) and controls (0.0130 pg/μg) (Table 2; Fig. 2; p=0.0001). In all three phases, the levels of CCL24 were found to be increased in AMD patients. Further, the difference was significant when compared between the wet AMD patients. The levels were significantly elevated in the occult (0.026 pg/μg) and predominantly classic AMD (0.021 pg/μg) as compared with minimally classic AMD (0.009 pg/μg) (Fig. 4). CCL24 levels were significantly increased in the individuals with one eye (0.0201 pg/μg) or both eyes affected (0.0226 pg/μg) as compared with normal controls (Fig. 5).

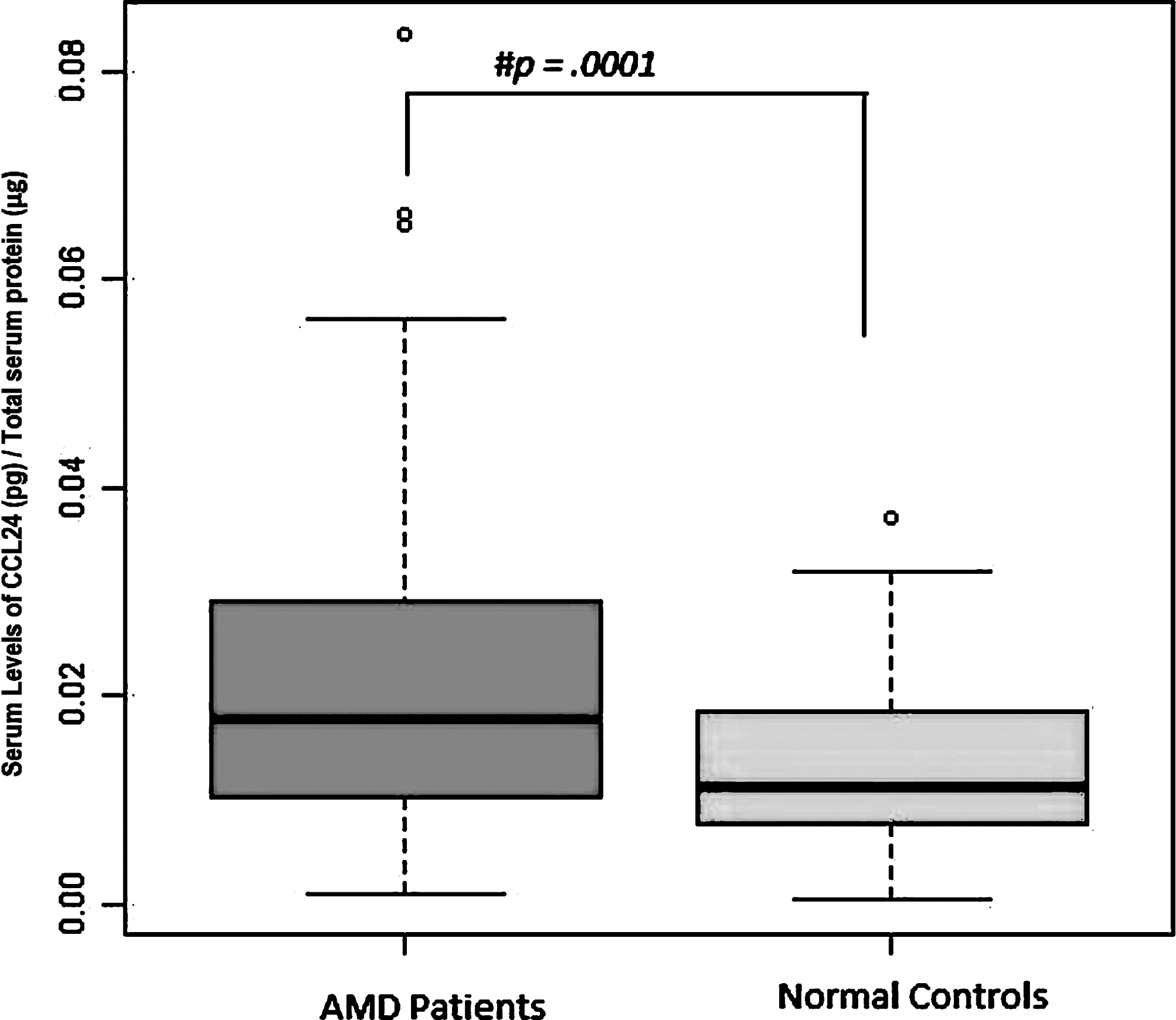
Serum levels of CCL24 in age-related macular degeneration (AMD) and normal controls. Boxes include values from first quartile (25th percentile) to third quartile (75th percentile). Lower and upper error bars refer to 10th and 90th percentile, respectively. The black horizontal line in the box represents median for each dataset. The symbol # indicates significant difference (p<0.05) between the given conditions. Levels of CCL24 were normalized to total protein. Outliers are shown in circles. Data were analyzed by parametric unpaired, independent 2-tailed Student's t-test. The symbol # indicates significant difference among the groups (p<0.05). pg, pictogram; μg, microgram.
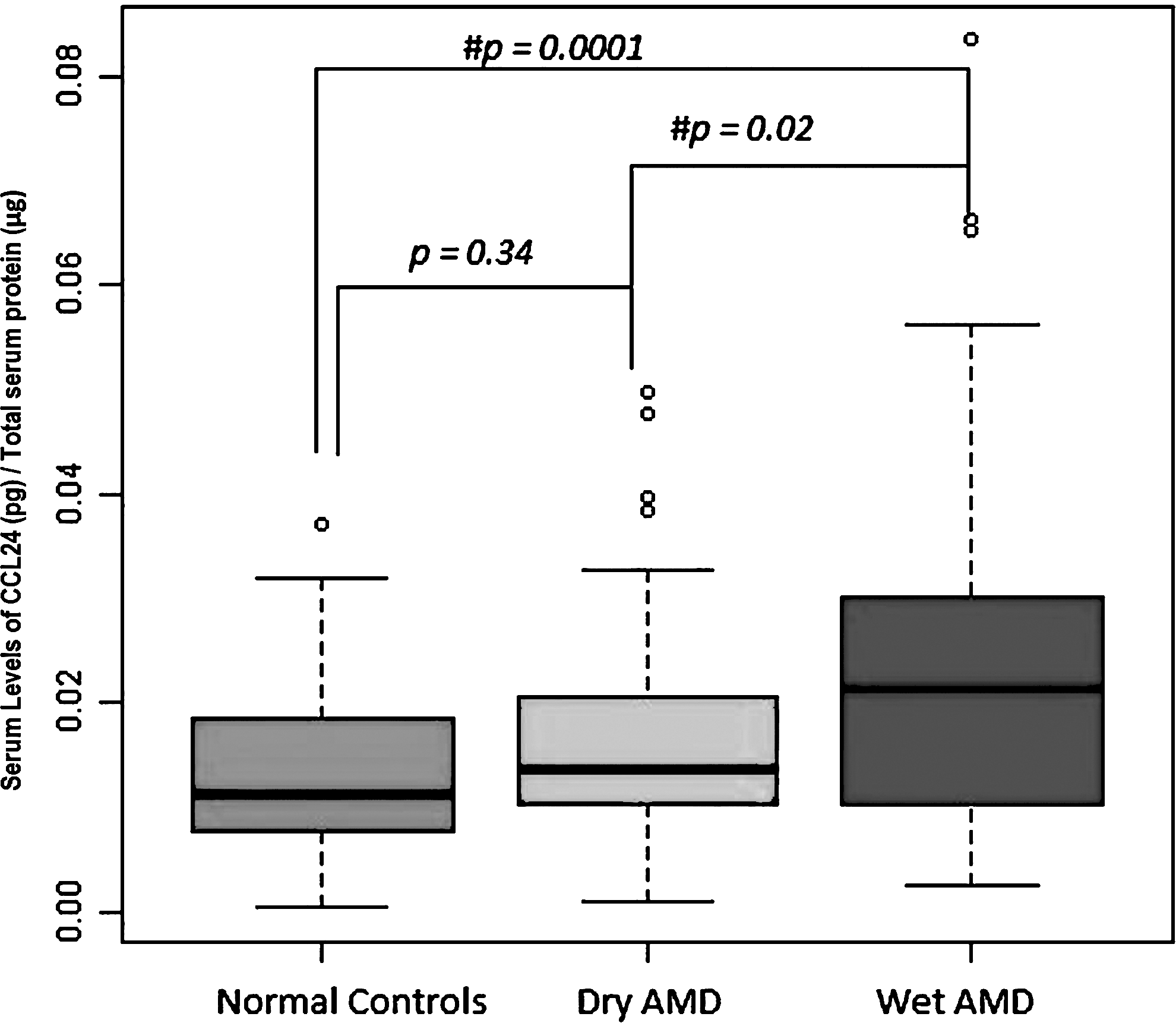
Serum levels of CCL24 in dry AMD, wet AMD, and normal controls. Boxes include values from first quartile (25th percentile) to third quartile (75th percentile). Lower and upper error bars refer to 10th and 90th percentile, respectively. The black horizontal line in the box represents median for each dataset. The symbol # indicates significant difference (p<0.05) between the given conditions. Levels of CCL24 were normalized to total protein. Outliers are shown in circles. Data were analyzed by analysis of variance (ANOVA) followed by Fisher's least significant difference (LSD) post hoc analysis among the groups. pg, pictogram; μg, microgram.
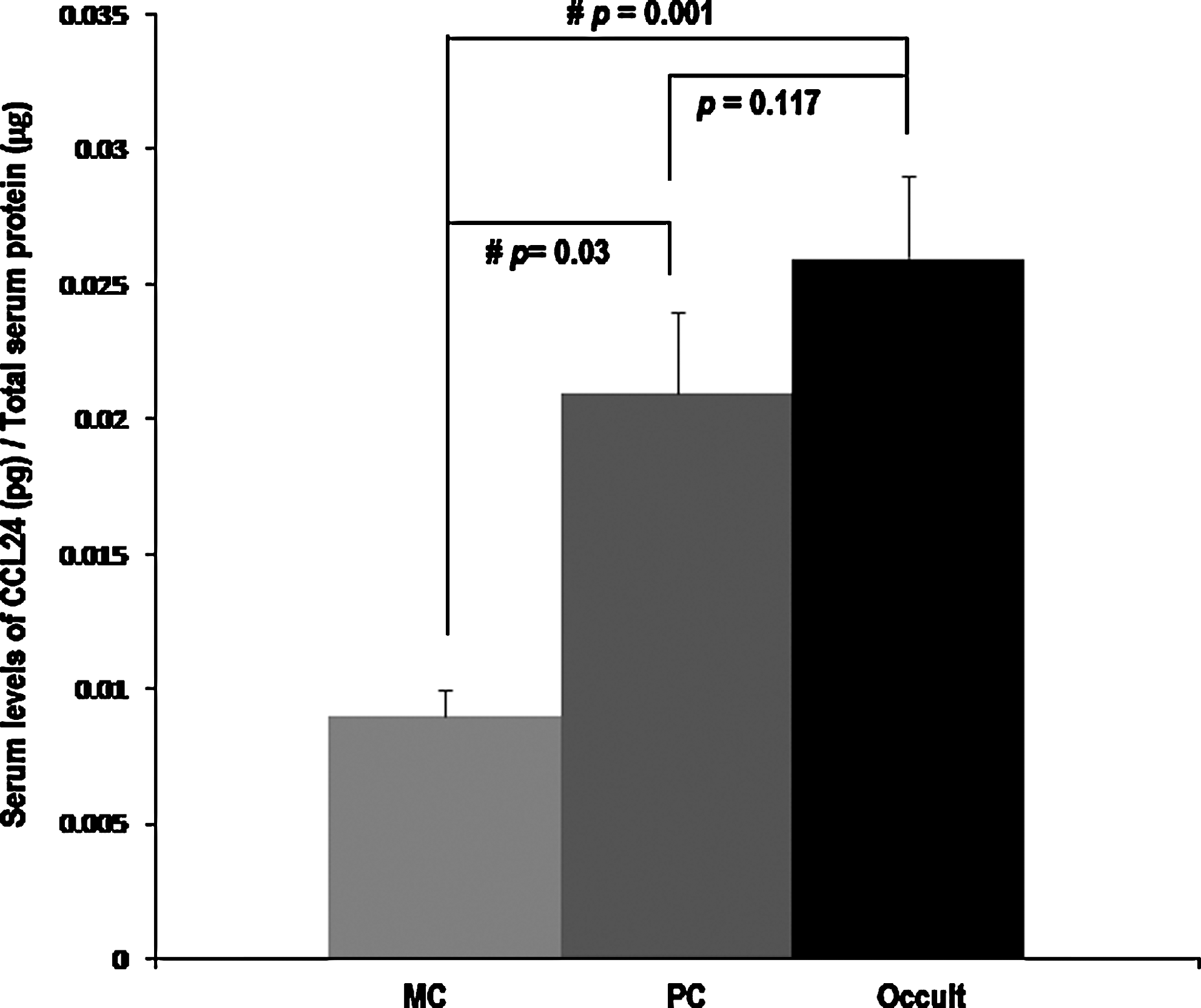
Serum levels of CCL24 in minimally classic (MC), predominantly classic (PC), and occult AMD patients. Values are plotted as mean±standard error in the bar diagram. Data were analyzed by unpaired, independent 2-tailed Student's t-test. The symbol # indicates significant difference among the groups (p<0.05). Levels of CCL24 were normalized to total protein.
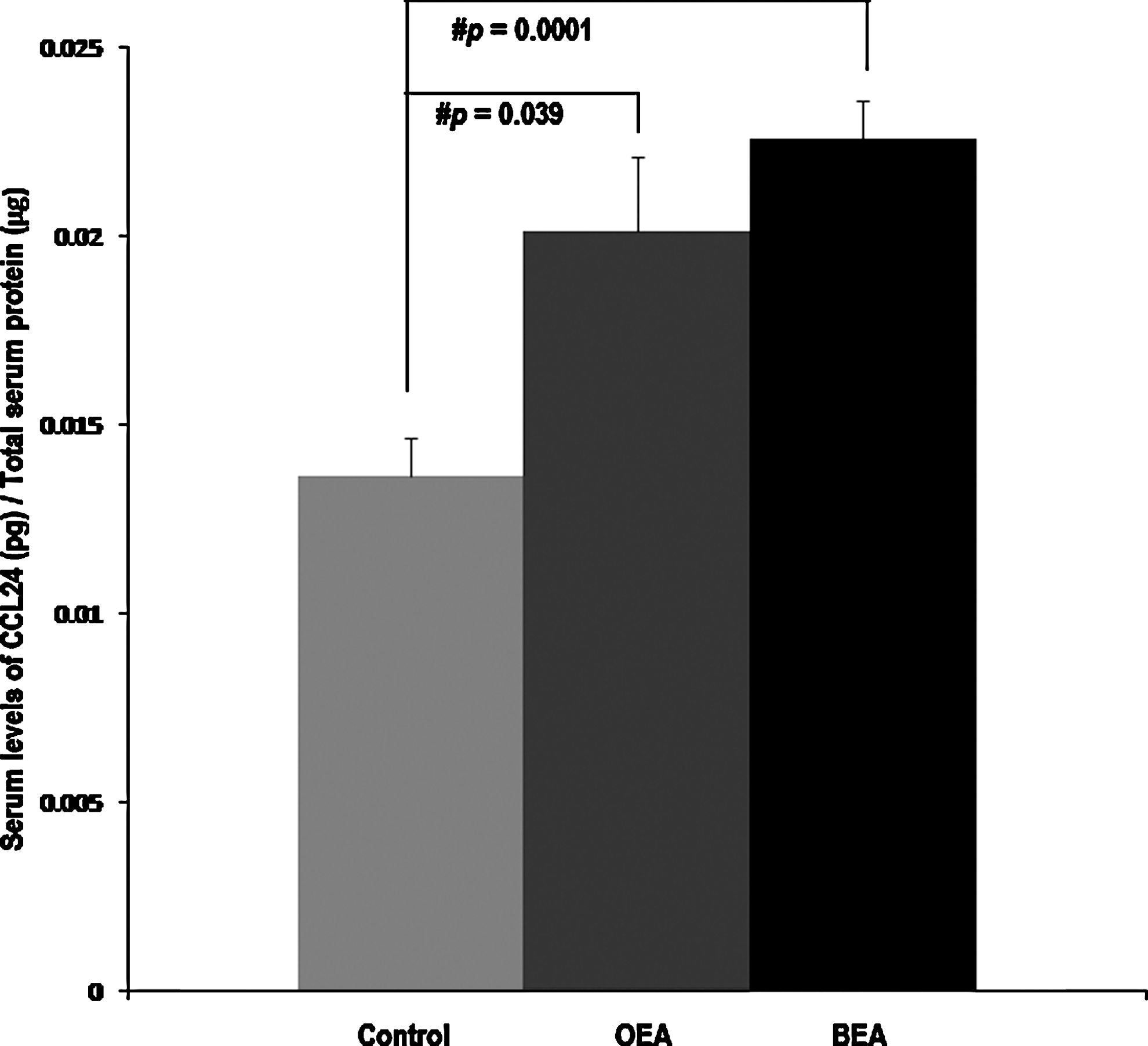
Serum levels of CCL24 in AMD patients in one eye affected (OEA), both eyes affected (BEA), and normal controls. Values are plotted as mean±standard error in the bar diagram. Data were analyzed by unpaired, independent 2-tailed Student's t-test. The symbol # indicates significant difference among the groups (p<0.05). Levels of CCL24 were normalized to total protein.
Effect of Avastin treatment on CCL24
CCL24 levels were also compared between wet variant of AMD patients who received single Avastin treatment (dose 1.25 mg in 0.05 mL) and those who did not (Table 3) in a final phase analysis. CCL24 levels were significantly elevated in the wet AMD patients (0.0273 pg/μg) who received Avastin treatment as compared with those wet AMD patients who did not receive Avastin treatment (0.0134 pg/μg) (p-value=0.0001 at α=0.05; Fig. 6).
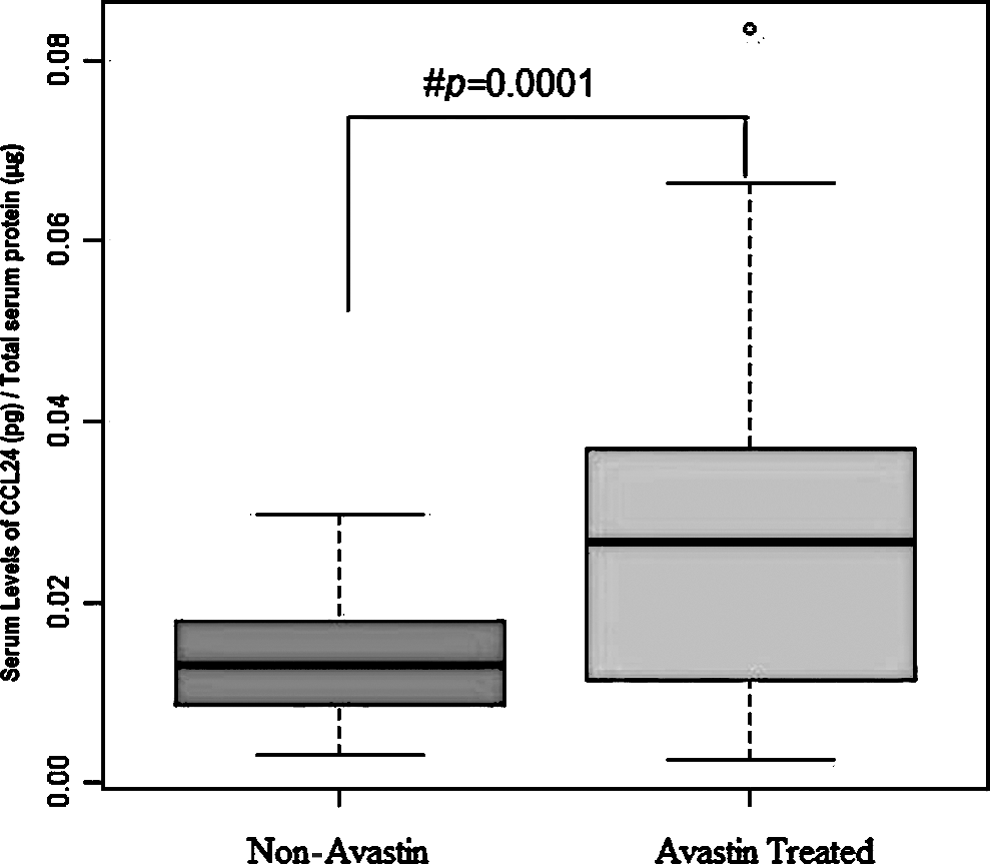
Serum levels of CCL24 in Avastin-treated and not treated wet AMD. Boxes include values from first quartile (25th percentile) to third quartile (75th percentile). Lower and upper error bars refer to 10th and 90th percentile, respectively. The black horizontal line in the box represents median for each dataset. The symbol # indicates significant difference (p<0.05) between the given conditions. Levels of CCL24 were normalized to total protein. Outliers are shown in circles. Data were analyzed by parametric unpaired, independent 2-tailed Student's t-test. The symbol # indicates significant difference among the groups (p<0.05). pg, pictogram; μg, microgram.
Risk factors associated with CCL24
A separate analysis was carried out while adjusting the risk factors to AMD. Important risk factors that induced alterations in CCL24 levels included smoking, alcohol, and hypertension. The results shown in Table 4 were obtained by segregating AMD patients and controls based on hypertension status, revealing that CCL24 levels vary significantly within hypertensive and nonhypertensive AMD patients. The CCL24 levels were also found significant when it was compared between hypertensive AMD patients and hypertensive healthy controls (Table 4; Fig. 7). We did not find any significant difference between smoker/nonsmoker and alcoholic/nonalcohlic AMD patients (Tables 5 and 6). However, when AMD smokers and control smokers were analyzed for CCL24 levels, it was found to be upregulated in the former; similar trends were seen when compared with alcohol consumer AMD and alcohol consumer controls (Tables 5 and 6; Figs. 8 and 9). But there was no significant difference between AMD smokers versus AMD nonsmokers and alcohol consumers versus nonconsumers, thus enhancing reliability of end points assessed. The variable selection tool utilizing the linear model was applied to uncover the association between risk factors and altered CCL24 levels suggesting hypertension to have etiopathological association with AMD. The data remained unchanged whether it was analyzed from two categories [AMD and control; Akaike information criteria (AIC)=−1588.1] or three categories (dry AMD, wet AMD, and healthy control; AIC=−1590.6) (AIC: whose lowest value provides best model fit among all possibilities). Further, multivariate analysis was applied using CCL24 as a dependent variable and diagnosis and hypertension as an independent variable, which revealed similar outcomes, that is, significant difference at α=0.05. However, hypertension was found to be significant at α=0.1. Box plots shown in Figures 2, 3, and 7 –9 depict the distribution of CCL24 levels varied by AMD and controls (Figs. 2 and 3) and the same has been stratified to see the impact of hypertension, smoking, and alcohol (Figs. 7 –9). In addition to the significant changes in CCL24 levels, these box plots also depict a few outliers.
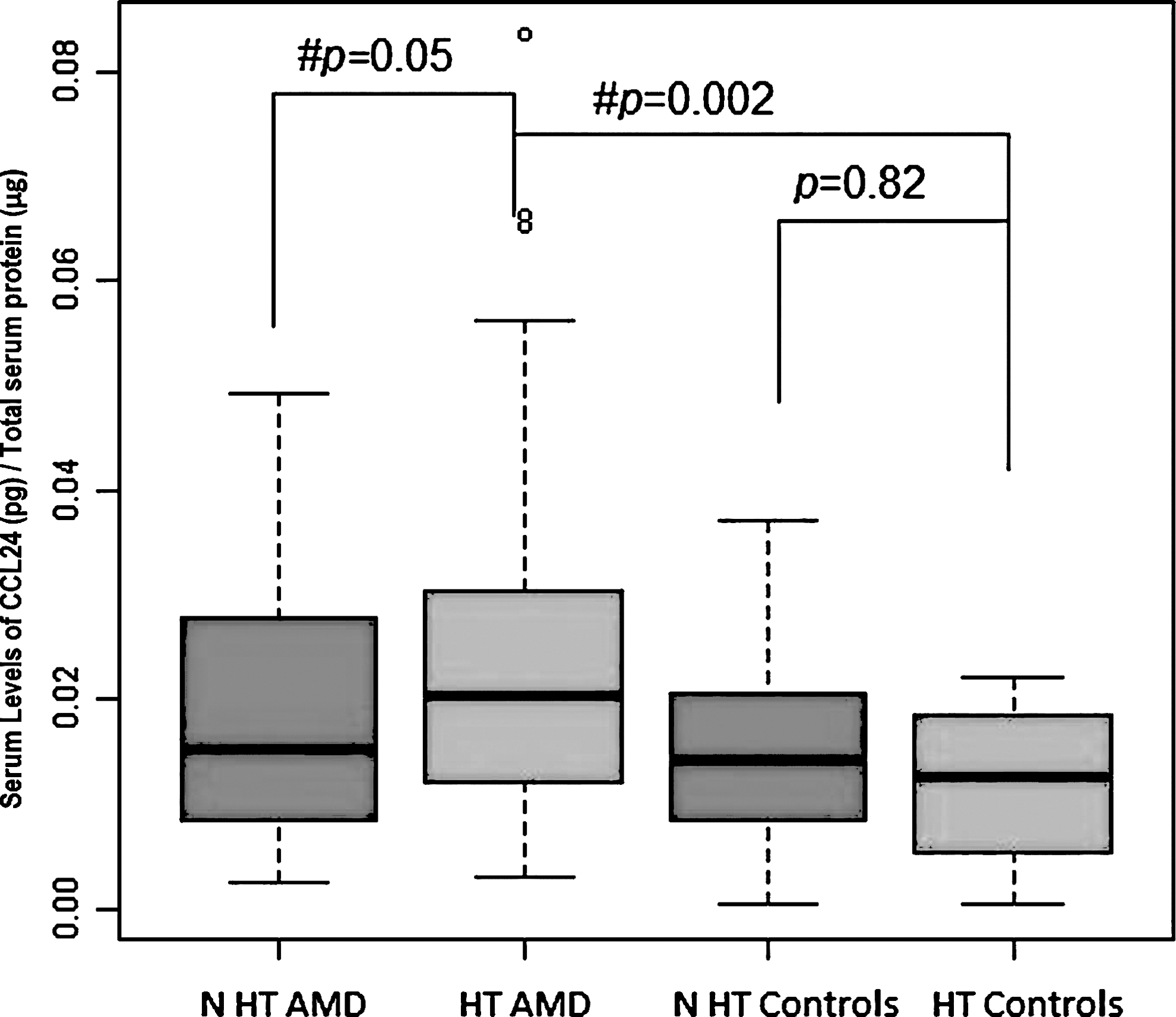
Serum levels of CCL24 in hypertensive and nonhypertensive AMD and normal controls. Boxes include values from first quartile (25th percentile) to third quartile (75th percentile). Lower and upper error bars refer to 10th and 90th percentile, respectively. The black horizontal line in the box represents median for each dataset. The symbol # indicates significant difference (p<0.05) between the given conditions. Levels of CCL24 were normalized to total protein. Outliers are shown in circles. Data were analyzed by ANOVA followed by Fisher's LSD post hoc analysis among the groups. pg, pictogram; μg, microgram; N HT AMD, nonhypertensive AMD; HT AMD, hypertensive AMD; N HT Controls, nonhypertensive controls; HT Controls, hypertensive controls.
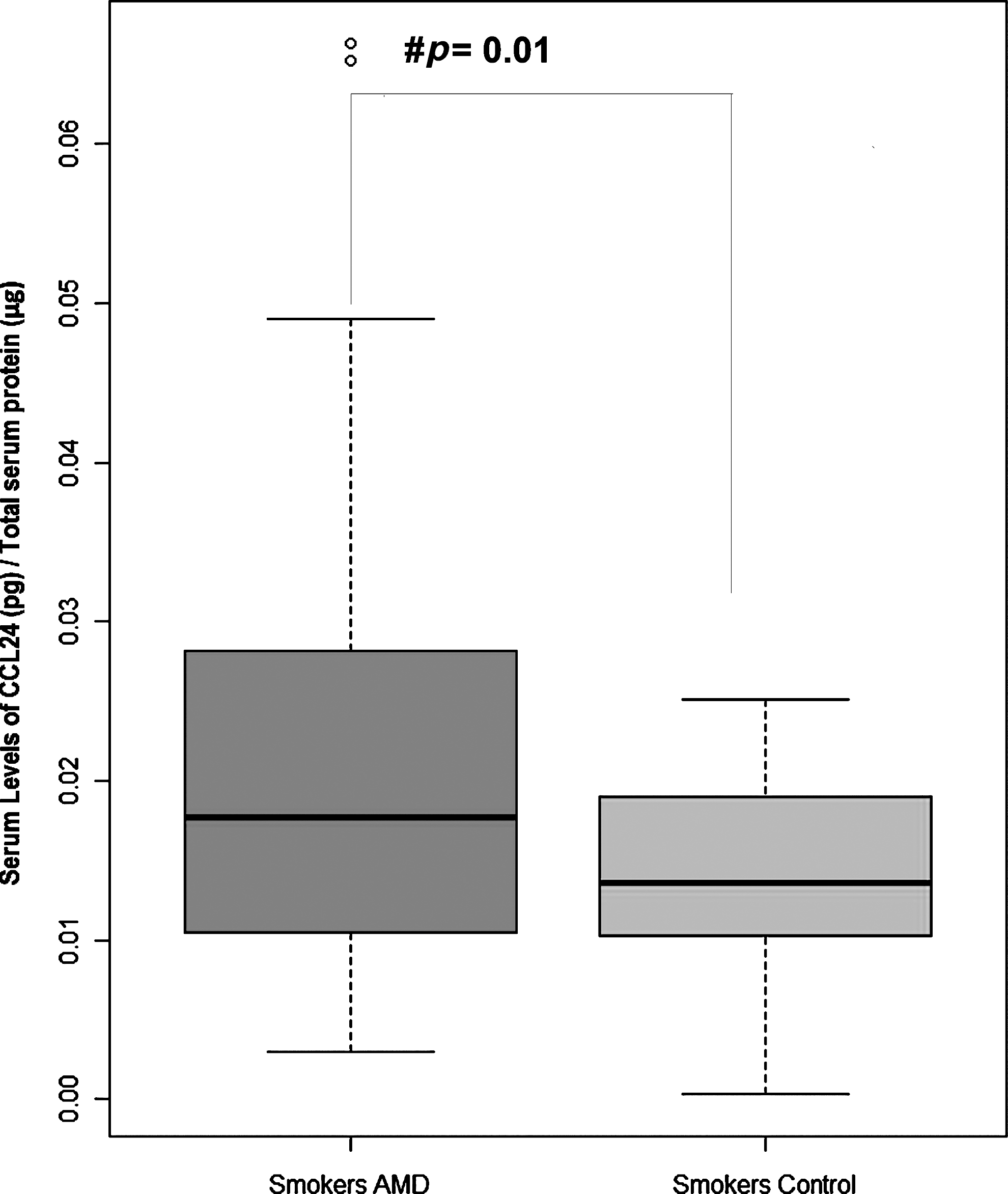
Serum levels of CCL24 in AMD smokers and control smokers. Boxes include values from first quartile (25th percentile) to third quartile (75th percentile). Lower and upper error bars refer to 10th and 90th percentile, respectively. The black horizontal line in the box represents median for each dataset. The symbol # indicates significant difference (p<0.05) between the given conditions. Levels of CCL24 were normalized to total protein. Outliers are shown in circles. Data were analyzed by parametric unpaired, independent 2-tailed Student's t-test. The symbol # indicates significant difference among the groups (p<0.05). pg, pictogram; μg, microgram.

Serum levels of CCL24 in alcohol consumer AMD and alcohol consumer controls. Boxes include values from first quartile (25th percentile) to third quartile (75th percentile). Lower and upper error bars refer to 10th and 90th percentile, respectively. The black horizontal line in the box represents median for each dataset. The symbol # indicates significant difference (p<0.05) between the given conditions. Levels of CCL24 were normalized to total protein. Outliers are shown in circles. Data were analyzed by parametric unpaired, independent 2-tailed Student's t-test. The symbol # indicates significant difference among the groups (p<0.05). pg, pictogram; μg, microgram.
HT, hypertensive; NHT, nonhypertensive.
Smk, smoker; N-Smk, nonsmoker.
Al, alcoholic; N-Al, nonalcoholic.
Discussion
AMD is one of the devastating disorders affecting central vision. Many studies have attempted to associate various biomarkers and candidate targets in the pathogenesis of AMD. Our earlier studies that showed that CCL2/CCR2-deficient mice exhibit features of AMD when combined with recent studies establishing CCL24 as an emerging candidate for AMD pathogenesis result in launching of CCL2 and CCL24 analysis in serum of AMD patients. The data presented here are limited to CCL24 analysis.
This study was conducted to determine whether differences in levels of serum CCL24 exist between patients with AMD and healthy controls. Our results indicate that the CCL24 expression level increased significantly in wet type of AMD patients as compared with dry type of AMD and normal controls. Within the wet AMD group, the levels were significantly higher in occult and predominantly classic AMD as compared with minimally classic AMD. This may be due to the increase in the inflammatory cells in occult and predominantly classic AMD because CCL24 is secreted by inflammatory cells such as macrophages and eosinophils. We believe these observations to have strong implications for evolving new strategies for targeting CCL24 in wet AMD. These results indirectly support the results of Takeda et al. (2009) who very recently showed that eotaxin and its receptor is a potential therapeutic agent as compared to others for treating wet AMD (Forssmann et al., 1997), indicating that CCL24 may impact the pathogenesis of the disease. CCL24 blockade had been shown to be more effective at inhibiting CNV development than VEGF-A neutralization. As anti-VEGF drugs, such as Lucentis and Avastin, are one of the most effective tools currently available to combat CNV. Many argue that unlike VEGF-A blockade, CCL24 blockade could be less toxic to the retina and holds potential for AMD treatment (Forssmann et al., 1997). The intravitreal injection of Avastin causes many problems, as it is associated with significant risk of acute intraocular inflammation that may result in significant visual loss (Wickremasinghe et al., 2008; Georgopoulos et al., 2009; Johnson et al., 2010) and increase the intraocular pressure (Good et al., 2011). For promoting inflammation, eotaxin–CCR3 interaction is likely to represent a major mechanism (Yawalkar et al., 1999). Our report provides evidence directly from human samples showing that CCL24 levels increase substantially in the Avastin-treated patients as compared with the untreated AMD patients. With this background it is important to review our knowledge about eotaxins that are of three types, namely, eotaxin-1/CCL11 (Ponath et al., 1996), eotaxin-2/CCL24 (Forssmann et al., 1997), and eotaxin-3/CCL26 (Kitaura et al., 1999). All of these activate the C-C chemokine receptor-3 and share (Daugherty et al., 1996; Kitaura et al., 1996) several functions like eosinophil chemoattraction and activation (Luster and Rothenberg, 1997; Rothenberg, 1999; Shahabuddin et al., 2000). Eotaxin-2, also known as myeloid progenitor inhibitory factor-2, is a member of the CC chemokine subfamily and is designated as CCL24. Further, it is also known that lipopolysaccharide and Interleukin-4 (IL-4) differentially regulate the expression of eotaxin-2 in monocytes and macrophages. Functionally, eotaxin-2 is more closely related to eotaxin-1/CCL11 and eotaxin-3/CCL26. The three proteins share low sequence homology but have been shown to be potent eosinophil chemoattractants that bind and activate the chemokine receptor CCR3, a receptor that is highly expressed in eosinophils. CCL24 also has the ability to suppress myeloid cell proliferation, a biological function not shared by eotaxin (Petkovic et al., 2004).
CCR3 has also recently been designated as CD193 (cluster of differentiation 193). The protein encoded by this gene is a receptor for C-C-type chemokines. It belongs to family 1 of the G protein–coupled receptors. This receptor binds and responds to a variety of chemokines, including eotaxin-2 (CCL24), eotaxin-3 (CCL26), MCP-3 (CCL7), MCP-4 (CCL13), and RANTES (CCL5). In addition, it has been shown that eotaxin–CCR3 is expressed on the surface of CNV vessels in humans but is absent from normal retinal vascular tissue. Our report uncovers the nonredundant role of CCL24 in pathogenesis of AMD and may stimulate multicenter and multiethnic studies to verify the evidence presented here. It is pertinent to note that many of the important molecules being investigated in the recent studies bear direct association with lifestyle risk factors; for instance, many epidemiology studies have found an association between hypertension, smoking, and increased risk of AMD (Hogg et al., 2008; Kabasawa et al., 2011). Our results also showed association of hypertension with levels of CCL24 in the AMD patients analyzed, but the difference between smoker/nonsmoker and alcoholic/nonalcohlic AMD patients was not significant. Hypertension may increase the oxidative stress known to be associated with AMD resulting in expression of CCL24 in choroidal endothelial cells and its ligands in RPE (Chong et al., 2008). Notwithstanding AMD as an eye disorder, the analysis of serum is consistent with several previous reports in both retina and brain (Sharma et al., 2009; Baas et al., 2010; Vinish et al., 2010). Therefore, CCL24 could represent a novel biomarker for early detection of CNV with potential to be targeted as a new therapeutic entity through future studies. Early analysis of CCL24 in patients presenting with CNV—prior even to the lesion entering the subretinal space, compared to other progressive stages of AMD—could shed light on whether CCL24 is causally related to AMD or is the consequence of CNV. Thus, at this point, we are unable to speculate whether CCL24 precedes CNV. A logistic longitudinal study is implicated to address such outstanding questions. Abundant quantity of CCL24-specific binding molecule either detected in the retina or choroid could be indicative of CNV. Early detection may allow for therapy to be initiated early, even before CNV takes place, thereby resulting in halting the disease. In addition, labeling of CCL24 molecules can be used to monitor the progress of therapy.
Our observations concluded that higher levels of serum CCL24 are associated with AMD patients despite Avastin treatment as compared with normal controls and those without Avastin, indicating that CCL24 may have an association with CNV and may be an important target to validate future therapeutic approaches in AMD in tandem with Avastin treatment but other ligands need to be studied before concluding that CCL24 is the only one among other ligands to be involved in the study. Additional immunohistochemical and biochemical investigations in autopsy specimens are needed to verify the claims held by this study. Besides, future studies can focus on the association of CCL24 levels in various populations with previously reported genetic risk factors.
Footnotes
Acknowledgments
The study was carried out at Department of Neurology, PGIMER, Chandigarh, India. The authors acknowledge Department of Science and Technology, India, for providing funds (F. No. SR/SO/HS-109/205 dated 1-05-2007). We are grateful to the volunteers involved in the study, laboratory staff, and all those who contributed in terms of time and effort.
Acquisition of data, writing, and editing of article: NKS. Grant co-PI and editing of article: SP. Inclusion of patients and clinical scoring: AG RS. Editing of article: PKG. Statistical analysis: PKG. Interpretation and analysis of data, grant PI and editing of article: AA.
Disclosure Statement
The authors declare that they have no competing interests to disclose.
The funders (F. No. SR/SO/HS-109/205 dated 1-05-2007) had no role in study design, data collection, and analysis; decision to publish; or preparation of the article.