
Abstract
Interleukin-4 (IL-4) is a pleiotropic cytokine that plays an important role in the immune system. Emerging evidences have shown that the common polymorphism (−590C/T; rs2243250 C>T) in the IL-4 gene may play an important role in the development of various liver diseases, but individually published studies revealed inconclusive results. This meta-analysis aims to derive a more precise estimation of the association between the IL-4 −590C/T polymorphism and susceptibility to liver disease. A literature search of PubMed, Embase, Web of Science and China BioMedicine databases was conducted on articles published before January 1st, 2013. Crude odds ratio with 95% confidence intervals were calculated to assess the strength of this association. Ten case–control studies were assessed with a total 1,140 patients and 1,649 healthy controls. The meta-analysis results indicated that the IL-4 −590T polymorphism might increase the risks of hepatitis B (HBV) and hepatitis C (HCV) infections. Further subgroup analyses showed significant associations between the IL-4 −590T polymorphism and increased risks of liver diseases among Caucasian populations, but similar associations were not found among Asian populations. Univariate and multivariate meta-regression analyses showed that differences in ethnicity and clinical subtype are the major sources of heterogeneity. No publication bias was detected in this meta-analysis. In conclusion, the current meta-analysis indicates that the IL-4 −590T polymorphism may play an important role in increasing HBV and HCV infection risks, especially among Caucasian populations.
Introduction
Several studies have indicated that the common promoter polymorphism (−590C/T) in the IL-4 gene might play a critical role in increasing an individual's susceptibility to HBV and HCV infection (Aithal et al., 2004; Zhu et al., 2005; Wang et al., 2006; Gao et al., 2012). However, some previous studies also suggested that the IL-4 polymorphisms were not associated with susceptibility to HBV, HCV, drug-induced liver injury, or hepatocellular carcinoma (Chen et al., 2007; Liu et al., 2007; Naslednikova et al., 2007; Pachkoria et al., 2008; Gao et al., 2009; Ognjanovic et al., 2009). In view of the conflicting results from previous studies, we performed a meta-analysis of all the available data to evaluate the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver diseases.
Materials and Methods
Literature search strategy
Relevant articles published before January 1st, 2013 were identified through a search in Pubmed, Embase, Web of Science and China BioMedicine databases using the following terms: (“genetic polymorphism” or “polymorphism” or “SNP” or “single-nucleotide polymorphism” or “gene mutation” or “genetic variants”) and (“liver diseases” or “hepatitis” or “liver cirrhosis” or “liver injury” or “hepatocellular carcinoma” or “fatty liver” or “hepatocellular carcinoma” or “hepatocellular carcinoma”) and (“interleukin-4” or “B-cell growth factor-1” or “IL4” or “IL-4”). The references from the eligible articles or textbooks were also reviewed to find potential sources of studies. Disagreements were resolved through discussions between the authors.
Inclusion and exclusion criteria
Studies included in our meta-analysis have to meet the following criteria: (1) case–control studies focused on the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver diseases; (2) all patients diagnosed with various liver diseases should have serological or histopathological confirmations or evidences; (3) published data about the frequencies of alleles or genotypes must be sufficient. Studies were excluded when they were (1) not a case–control study on the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver diseases; (2) duplicates of previous publications; (3) publications with incomplete data; (4) meta-analyses, letters, reviews, or editorial articles. If more than one study by the same author using the same case series were published, either the study with the largest sample size or the most publication date was included.
Data extraction
Data from the published studies were extracted independently by two authors into a standardized form. For each study, the following characteristics and numbers were collected: the first author, year of publication, country, language, study design, ethnicity of subjects, numbers of subjects, gender ratio, mean age, detecting sample, genotype method, allele and genotype frequencies of SNP, and evidence of Hardy–Weinberg equilibrium (HWE). In cases of conflicting evaluations, disagreements were resolved through discussions between the authors.
Quality assessment of included studies
Two authors independently assessed the quality of the included studies according to the modified STROBE quality score systems (da Costa et al., 2011). Forty assessment items related to quality appraisal were used in this meta-analysis with scores ranging from 0 to 40. Scores of 0–20, 20–30, and 30–40 were defined as low, moderate, and high quality, respectively. Disagreements were also resolved through discussions between the authors.
Statistical analysis
Crude odds ratios (ORs) with 95% confidence intervals (CIs) were calculated under five genetic models: the allele model (T allele versus C allele), the dominant model (TT+CT versus CC), the recessive model (TT versus CT+CC), the homozygous model (TT versus CC), and the heterozygous model (TT versus CT). The statistical significance of the pooled ORs was examined using the Z test. Between-study variations and heterogeneities were estimated using Cochran's Q-statistic with a p-value<0.05 as statistically significant heterogeneity (Jackson et al., 2012). We also quantified the effects of heterogeneity using the I2 test (ranges from 0% to 100%), which represents the proportion of interstudy variability that can be contributed to heterogeneity rather than to chance (Peters et al., 2006). When a significant Q-test, with p<0.05 or I2 >50% indicated that heterogeneity among the studies existed, the random-effects model (the DerSimonian Laird method) was conducted for the meta-analysis; otherwise, the fixed-effects model (the Mantel-Haenszel method) was used. To explore sources of heterogeneity, univariate and multivariate meta-regression analyses were used. Subgroup analyses were performed based on the clinical subtype, ethnicity, and genotype method. Sensitivity analysis was performed through omitting each study in turn to assess the quality and consistency of the results. Funnel plots were used to detect publication bias. The Egger's linear regression test was also used to evaluate the publication bias (Zintzaras and Ioannidis, 2005). We tested whether genotype frequencies were in HWE using the χ2 test. All the p values were two-sided. All analyses were calculated using the STATA Version 12.0 software (Stata Corp, College Station, TX).
Results
Characteristics of included studies
In accordance with the inclusion criteria, 10 case–control studies (Aithal et al., 2004; Zhu et al., 2005; Wang et al., 2006; Chen et al., 2007; Liu et al., 2007; Naslednikova et al., 2007; Pachkoria et al., 2008; Gao et al., 2009; Ognjanovic et al., 2009; Gao et al., 2012) were included in this meta-analysis and 148 were excluded. The flow chart of the study selection process is shown in Figure 1. A total of 2,789 subjects were involved in this meta-analysis, including 453 patients with HBV infection, 183 patients with HCV infection, 96 patients with HBV-HCV coinfection, 124 patients with liver cirrhosis, 164 patients with drug-induced liver injury, 120 patients with hepatocellular carcinoma, and 1,649 healthy controls. The publication years of the involved studies ranged from 2004 to 2012. Six of the 10 studies were conducted in Asian populations and the other four studies in Caucasian populations. All included studies used blood samples for genotyping. A classical polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) method was performed in seven studies and the TaqMan assay used in the other three studies. The HWE test was conducted on the genotype distribution of the controls in all 10 studies. None of the studies deviated from the HWE (all p>0.05). All quality scores of the included studies were higher than 20, indicating moderate high quality. The characteristics and methodological quality of the included studies are summarized in Table 1.
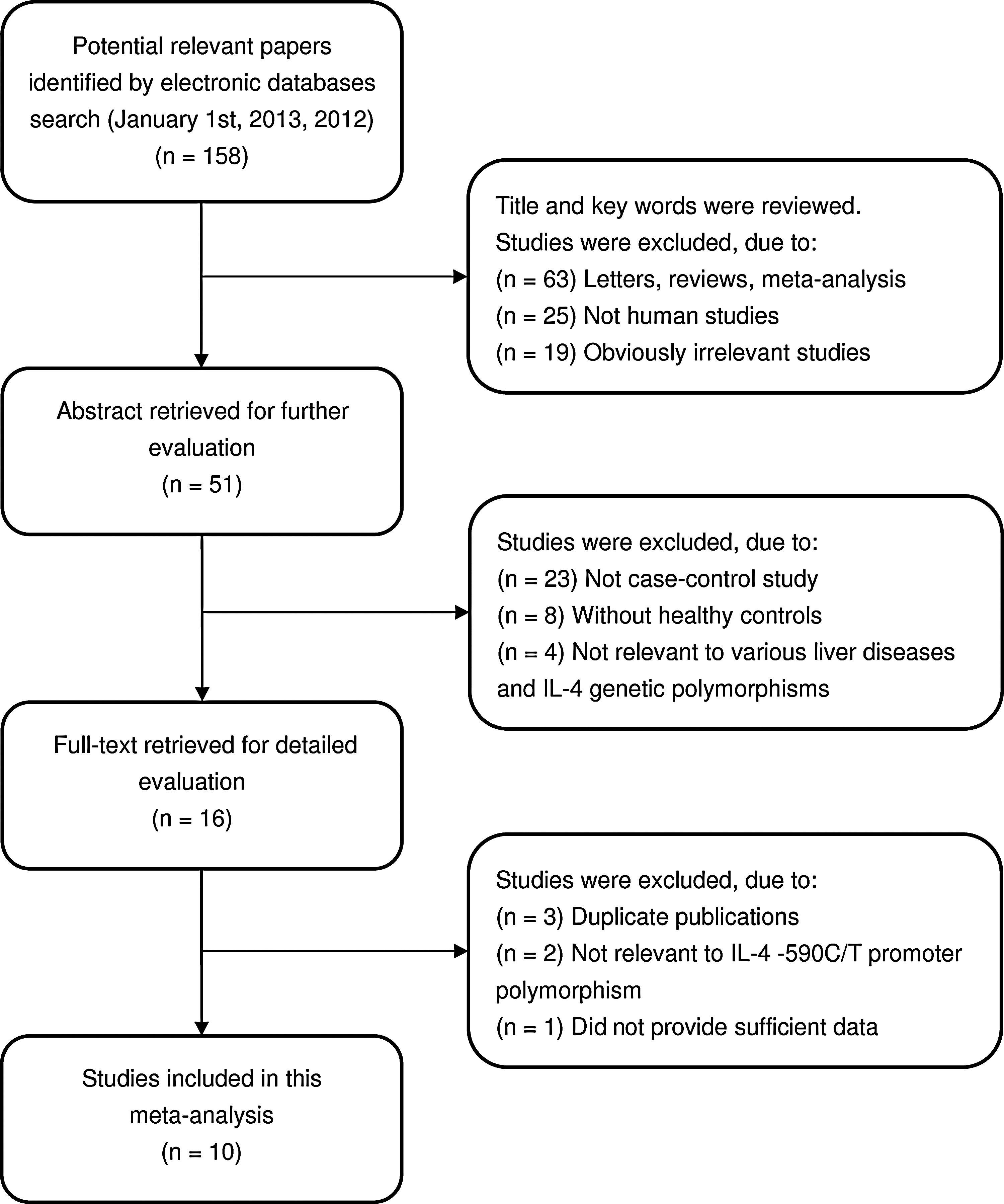
Flowchart of literature search and study selection process.
HBV, hepatitis B; HCV, hepatitis C; HCC, hepatocellular carcinoma; M, male; F, female; PCR-RFLP, polymerase chain reaction–restriction fragment length polymorphism; HWE, Hardy–Weinberg equilibrium; NR, not reported.
Quantitative data synthesis
A summary of the meta-analysis findings of the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver disease is provided in Table 2. The heterogeneity is not obvious under all five genetic models (all p>0.05 and I2 <50%), so the fixed-effects model was used. The meta-analysis results showed that the IL-4 −590T polymorphism may be associated with increased susceptibility to liver disease (T allele versus C allele: OR=1.20, 95%CI=1.01–1.41, p=0.035; TT+CT versus CC: OR=1.53, 95%CI=1.22–1.92, p<0.001). Further subgroup analysis by a clinical subtype showed significant associations between the IL-4 −590T polymorphism and increased risks of HBV and HCV infection under the dominant model (HBV: OR=1.54, 95%CI=1.07–2.21, p=0.019; HCV: OR=3.32, 95%CI=1.60–6.86, p=0.001) (Fig. 2). Results from subgroup analysis based on ethnicity indicated that the IL-4 −590T polymorphism may increase the risk of liver disease among Caucasian populations (T allele versus C allele: OR=1.54, 95%CI=1.09–2.18, p=0.015; TT+CT versus CC: OR=1.55, 95%CI=1.15–2.10, p=0.004), but similar associations were not found among Asian populations (Fig. 3). In the subgroup analysis by the genotype method, we also found significant associations between the IL-4 −590T polymorphism and increased risks of liver disease in the PCR-RFLP subgroup; however, we did not find similar associations in the TaqMan subgroup.
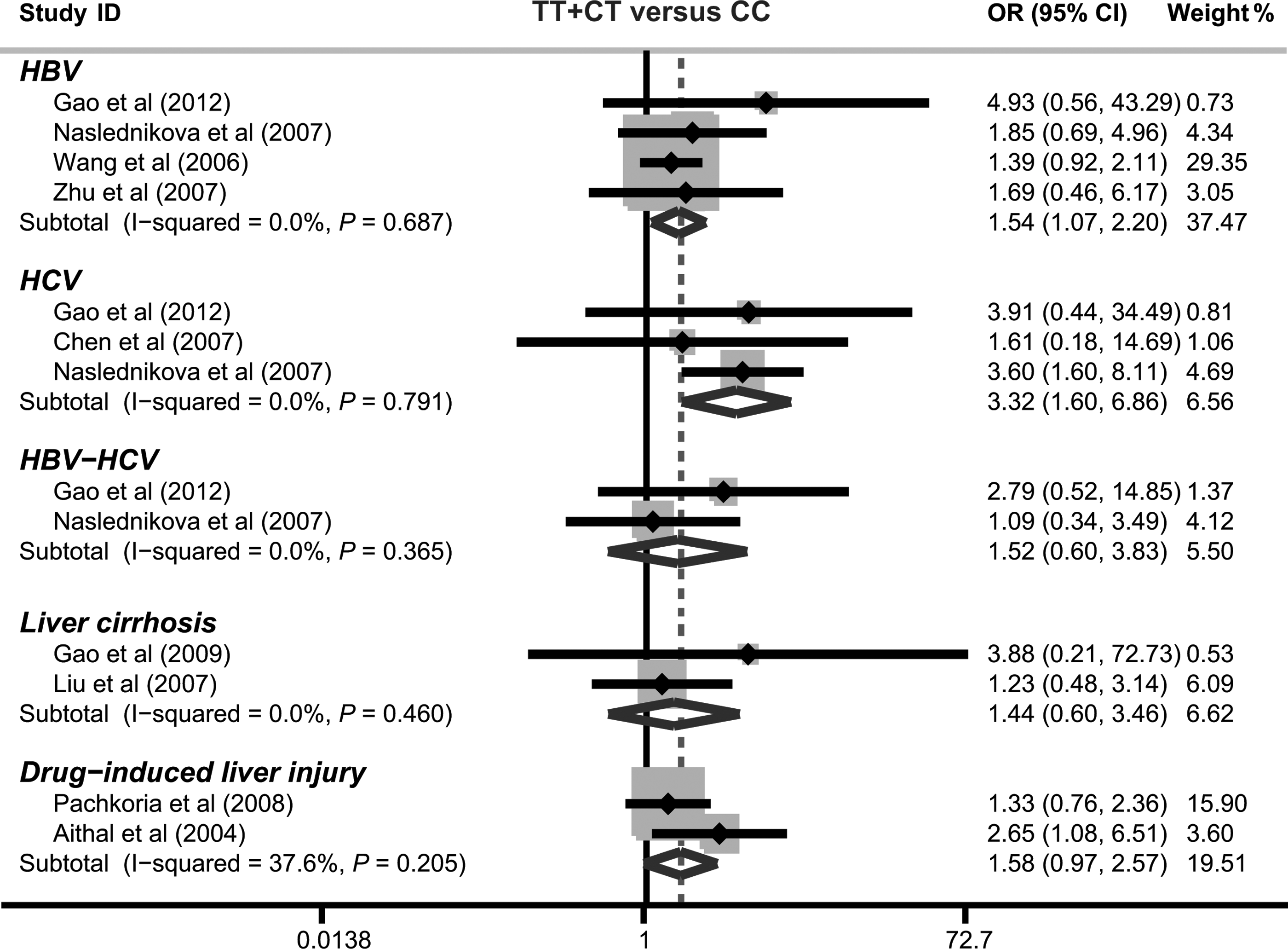
Forest plot for the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver disease under the dominant model.

Subgroup analysis by ethnicity for the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver disease under the allele model.
OR, odds ratios; ph , p value of heterogeneity test; †, estimates for random-effects model.
Meta-regression and sensitivity analyses
Univariate and multivariate meta-regression analyses were used to explore possible sources of heterogeneity among the studies. The results showed that differences in ethnicity and clinical subtype may be the major sources of heterogeneity (p<0.05) (as shown in Table 3). Sensitivity analysis was performed to assess the influence of each individual study on the pooled ORs by omitting individual studies. The analysis results suggested that no individual studies significantly affected the pooled OR of the association between the IL-4 −590C/T polymorphism and susceptibility to liver disease under the dominant model (Fig. 4).
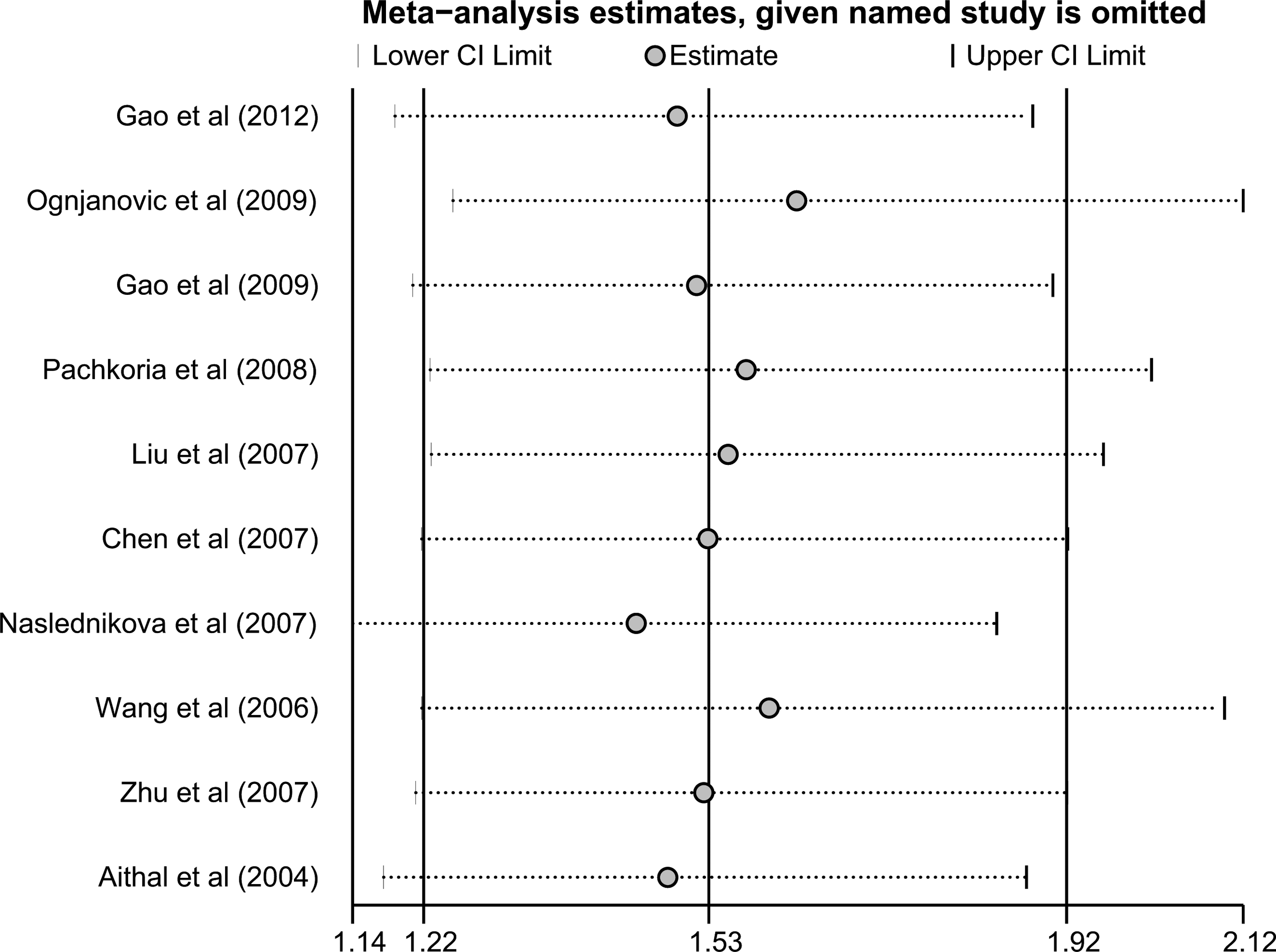
Sensitivity analysis of the summary OR of the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver disease under the dominant model. Results were computed by omitting each study in turn. Meta-analysis random-effects estimates (exponential form) were used. The two ends of the dotted lines represent the 95%CI.
SE, standard error; 95%CI, 95% confidence interval; UL, upper limit; LL, lower limit.
Publication bias
The funnel plot and Egger's linear regression test were performed to assess publication bias in the included studies. The shapes of the funnel plots of the association between IL-4 −590C/T polymorphism and susceptibility to liver disease did not reveal any evidence of obvious asymmetry (Fig. 5). The Egger's test also did not indicate any strong statistical evidence of publication bias under the dominant model (t=0.57, p=0.587).
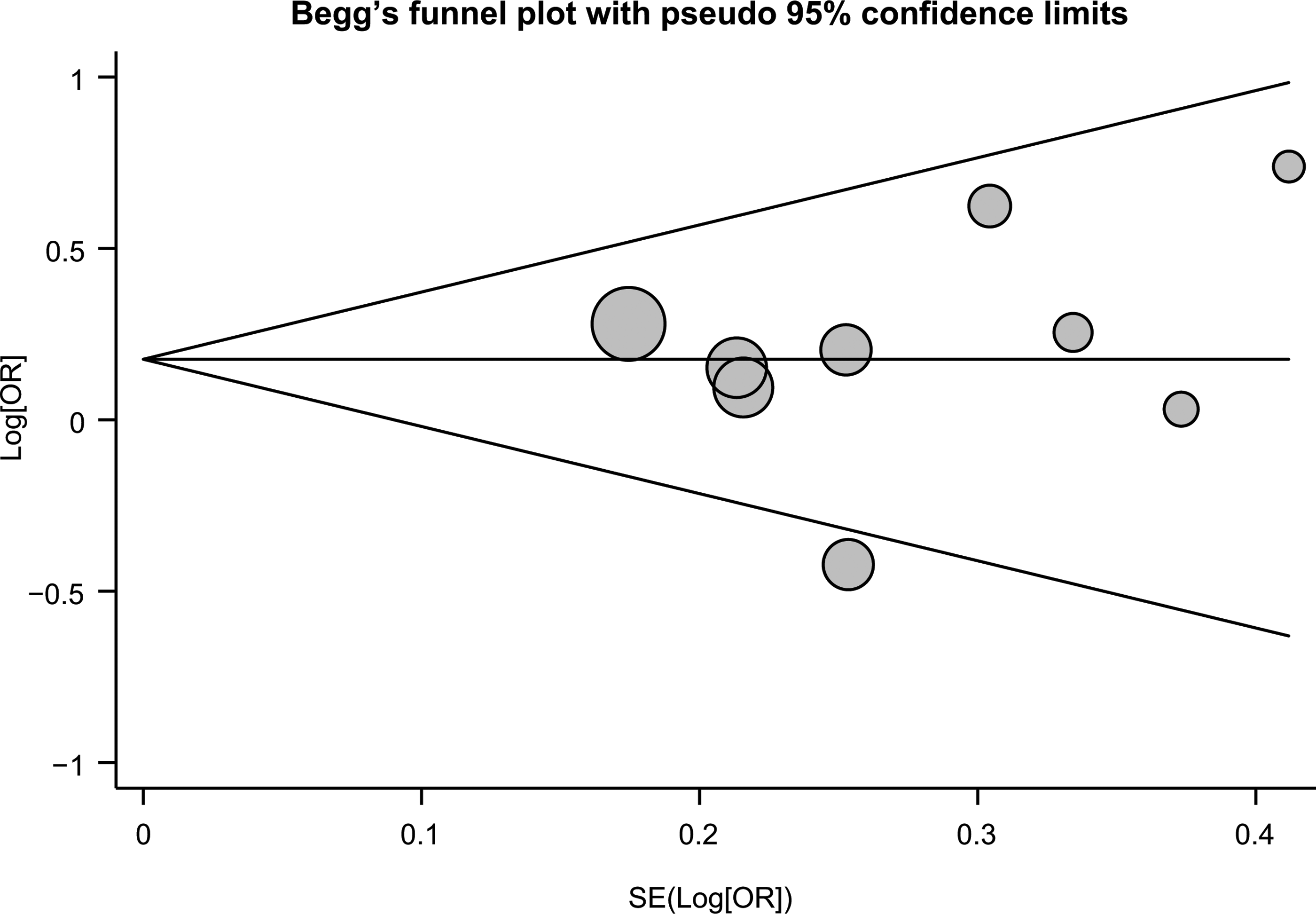
Funnel plot of the associations between the IL-4 −590C/T promoter polymorphism and susceptibility to liver disease under the dominant model. Each point represents a separate study for the indicated association. Log[OR], natural logarithm of OR. Horizontal line, mean magnitude of the effect.
Discussion
IL-4 is an immunomodulatory cytokine secreted by activated Th2 lymphocytes, basophils, and mast cells (Hou et al., 1994). It plays a critical role in the modulation of effector B and T cells and has been implicated in susceptibility to several human immune-related diseases (Dejaco et al., 2006; Huang et al., 2006). Thus, genetic mutations in the IL-4 gene may contribute to its abnormal expression and are probably linked to liver disease risks (Bataller et al., 2003). Many previous studies have suggested that the most common polymorphism (−590C/T) in the promoter region of the IL-4 gene may play an important role in the risk of liver disease (Aithal et al., 2004; Zhu et al., 2005; Wang et al., 2006; Gao et al., 2012), while other studies found no convincing evidence of these polymorphisms in increasing liver disease risks (Chen et al., 2007; Liu et al., 2007; Naslednikova et al., 2007; Pachkoria et al., 2008; Gao et al., 2009). This controversy could be explained with several reasons, such as the differences in study designs, sample size, ethnicity of the subjects, source of the subjects, and genotype methods (Rosenthal and DiMatteo, 2001; Chung et al., 2006). Therefore, we performed a meta-analysis to provide a comprehensive and reliable conclusion on the association between the IL-4 −590C/T promoter polymorphism and susceptibility to liver disease.
In this meta-analysis, 10 case–control studies were included with a total of 1,140 liver disease patients and 1,649 healthy controls. When all the eligible studies were pooled into the meta-analysis, the results indicated that the IL-4 −590T polymorphism may increase the risks of HBV and HCV infections, especially among Caucasian populations, while similar associations were not observed among Asian populations. Although the exact functions of the IL-4 genetic polymorphisms in HBV or HCV infections are not yet clear, a possible explanation could be that inherited mutations in IL-4 might be associated with the changes in expression and function of cytokines and thereby could possibly explain interindividual differences in susceptibility to HBV or HCV (Ganem and Prince, 2004; Nieters et al., 2005). These findings are consistent with the previous hypothesis that variability in the IL-4 gene may increase risks of HBV and HCV infections, suggesting that they may be useful as biomarkers in predicting an individual's susceptibility to HBV and HCV infections (Jiang et al., 2000; Donaldson, 2004).
Some limitations of this meta-analysis should be acknowledged. First, there were only 10 articles included in the present meta-analysis, so the sample size was relatively small and may not provide sufficient statistical power. Therefore, more studies with a larger sample size are still needed to accurately provide a more representative statistical analysis. Second, as a type of a retrospective study, a meta-analysis may encounter recall or selection bias, which could possibly influence the reliability of our study results (Ioannidis and Lau, 1999, Juni and Egger, 2009). Third, our lack of access to the original data from the studies limited further evaluations of potential interactions between other factors and liver disease risks, such as gene–environment and gene–gene interactions (Dennis et al., 2011). In spite of these limitations, however, this is the first meta-analysis of the relationship between the IL-4 −590C/T promoter polymorphism and susceptibility to liver disease.
In conclusion, our meta-analysis suggests that the IL-4 −590T polymorphism may play an important role in increasing HBV and HCV infection risks, especially among Caucasian populations. These relationships have the potential to provide a functional profiling of the IL-4 gene involved in humoral and cell-mediated immunity, and it may also help us understand the biological processes associated with the development of liver diseases, especially for HBV and HCV infections. However, detailed studies are still needed to confirm our findings. Further studies investigating the effects of gene–environment and gene–gene interactions on susceptibility to liver diseases are also essential.
Footnotes
Acknowledgments
This study is funded by the Science Foundation of Science and Technology Bureau of Liaoning Province of China (No. 2008225008-8).
Author Disclosure Statement
No competing financial interests exist.