
Abstract
Increasing scientific evidences suggest that CDH1 gene promoter polymorphism and DNA methylation may contribute to the development and progression of bladder cancer, but many existing studies have yielded inconclusive results. This meta-analysis aims to assess the role of CDH1 gene promoter polymorphism and methylation in bladder carcinogenesis. An extensive literature search for relevant studies was conducted in PubMed, Embase, Web of Science, Cochrane Library, and CBM databases from their inception through April 1, 2013. This meta-analysis was performed using the STATA 12.0 software. The crude odds ratio with 95% confidence interval was calculated. Fifteen studies were included in this meta-analysis with a total of 824 bladder cancer patients and 818 healthy controls being assessed. Our meta-analysis revealed that the A variant of CDH1 −160C/A polymorphism was associated with an increased risk of bladder cancer. Further analysis by pathological subtype indicated that patients with invasive carcinoma had a higher frequency of CDH1 −160A variant than those with superficial carcinoma. We analyzed the methylation frequency of CDH1 gene in 608 bladder cancer samples and 338 normal bladder samples. Our data strongly suggest that the CDH1 promoter methylation frequencies in bladder cancer tissues were greater than those in normal control tissues. In conclusion, our meta-analysis indicates that promoter polymorphism and methylation of CDH1 gene may be involved in the development and progression of bladder cancer. CDH1 gene promoter polymorphism and methylation might be promising biomarkers for the diagnosis and prognosis of bladder cancer.
Introduction
B
E-cadherin, encoded by CDH1 gene, is a single-pass transmembrane glycoprotein, containing five extracellular repeats, which mediates its Ca2+-dependent homophilic interactions with opposing molecules on neighboring cells (Kitajima, 2013). Recent evidences indicate that the loss of E-cadherin functions may alter neoplastic cell growth and adhesion, which has been suggested to be a major factor responsible in tumor invasion and metastasis, known in breast, colon, prostate, stomach, liver, and bladder carcinomas (Rakha et al., 2010; Canel et al., 2013). Inactivation or downregulation of E-cadherin through mutations, allelic deletions, or epigenetic changes are associated with tumor aggressiveness and metastasizing potentials (Kiemeney et al., 2006). Therefore, CDH1 gene has generally been recognized as an invasion-suppressor gene (Christofori and Semb, 1999). Human CDH1 gene is located on chromosome 16q22.1 and consists of 16 exons, spanning∼100 kb (Christofori and Semb, 1999). Promoter silencing of CDH1 gene through aberrant methylation is the earliest and most frequent event known to occur in human cancer (Esteller et al., 2001; Esteller, 2008). Accumulating experimental evidences indicate that promoter polymorphism and DNA methylation of CDH1 gene are associated with bladder cancer susceptibility and prognosis (Hoque et al., 2006; Kiemeney et al., 2006; Lin et al., 2006; Yates et al., 2007). It was reported that a common SNP at position −160 (rs16260 C>A) in the promoter region of the CDH1 gene might act as a risk factor for bladder cancer (Ma et al., 2008). A recent meta-analysis also indicated that −160A of the CDH1 gene is emerging as a low-penetrance tumor susceptibility allele for developing urothelial bladder cancer (Wang et al., 2008). Several previous studies have suggested that DNA methylation of CDH1 gene might be a reliable predictor of tumor progression in bladder cancer (Chan et al., 2002; Ribeiro-Filho et al., 2002; Friedrich et al., 2005; Pu et al., 2006; Yates et al., 2007). However, there are also some contradictory conclusions in the literatures concerning the prognostic value of CDH1 DNA methylation in the development and progression of bladder cancer (Bornman et al., 2001; Sun et al., 2009; Lin et al., 2012). The controversial findings are probably related to the effects from interacting with other genes, environmental effects on DNA methylation, different methods of classification, sample sizes, and study design. Therefore, we conducted a meta-analysis of all eligible studies to provide insights into the role of CDH1 −160 C>A polymorphism and promoter DNA methylation in bladder carcinogenesis.
Materials and Methods
Search strategy
The PubMed, CISCOM, CINAHL, Web of Science, Google Scholar, EBSCO, Cochrane Library, and CBM databases were searched from inception through April 1, 2013, without language restrictions. The following key words and MeSH terms were used: (“genetic polymorphism” or “single nucleotide polymorphism” or “SNP” or “mutation” or “variation” or “variant” or “methylation” or “hypermethylation”) and (“bladder cancer” or “bladder neoplasm” or “bladder tumor” or “bladder carcinoma” or “bladder carcinogenesis”) and (“E-cadherin” or “CDH1” or “cadherin-1”). We also performed a manual search to find other potential articles.
Selection criteria
The included studies had to meet all four of the following criteria: (1) cohort studies, nested case–control studies, or case–control studies that focus on the role of CDH1 −160 C>A polymorphism and promoter DNA methylation in bladder carcinogenesis; (2) the minimum number of cases in the included studies should be>30; (3) all patients diagnosed with bladder cancer should be confirmed through histopathologic examinations; (4) published data on the genotype and methylation frequencies were sufficient. If the study had failed the inclusion criteria, then it was excluded. When authors published several studies using the same subjects, either the one most recently published or with the largest sample size was included.
Relevant data were systematically extracted from all included studies by two authors (C.-Z.K. and Z.Z.) using a standardized form. The researchers collected the following data: language of publication, publication year of article, the first author's surname, geographical location, design of study, sample size, the source of the subjects, pathological subtype, types of DNA samples, detection method of SNP and DNA methylation, and genotype and methylation frequencies. In cases of conflicting evaluations, disagreements on inconsistent data (such as multiethnicity, unknown source of controls, unknown method for SNP and methylation, and uncertain frequencies of genotype and methylation) among the eligible studies were resolved through discussions and careful reexaminations of the full text by the authors.
Quality assessment
Methodological quality was independently assessed by two researchers according to the Newcastle-Ottawa Scale (NOS) criteria (Stang, 2010). The NOS criteria include three dimensions scored within the following ranges: (1) subject selection, 0–4; (2) comparability of subject, 0–2; (3) and clinical outcome, 0–3. NOS scores range from 0 to 9 with a score ≥7 indicating good quality.
Statistical analysis
The crude odds ratio (OR) with 95% confidence interval (CI) was calculated in a fixed- or random-effect model. The significance of the pooled estimate was determined using the Z test. The Cochran's Q-statistic and I 2 test were used to evaluate potential heterogeneity between studies (Zintzaras and Ioannidis, 2005; Jackson et al., 2012). If the Q-test showed a p<0.05 or I 2 test exhibits >50%, indicating significant heterogeneity, then the random-effect model was conducted; otherwise the fixed-effect model was used. We also performed subgroup and meta-regression analyses to explore potential sources of heterogeneity (Ioannidis et al., 2008). Sensitivity analysis was performed by omitting each study in turn to evaluate the influence of single studies on the overall estimate. Begger's funnel plots and Egger's linear regression test were conducted to investigate publication bias (Peters et al., 2006). STATA software version 12.0 (Stata Corp., College Station, TX) was used for this meta-analysis.
Results
Baseline characteristics of included studies
A total of 113 articles relevant to the searched key words were initially identified. Of these articles, 43 were excluded after an initial review of their titles and key words; then, abstracts and full texts were reviewed, and another 55 articles were excluded. Fifteen studies met our inclusion criteria for this meta-analysis. Publication years of the eligible studies ranged from 2001 to 2012. The flow chart of the study selection process is shown in Figure 1. A total of 1624 subjects were included in this meta-analysis, including 824 bladder cancer cases and 818 healthy controls. Peripheral blood samples were used to determine the promoter −160C/T (rs16260 C>A) polymorphism. Genotype methods include polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) and direct DNA sequencing. Analysis of the promoter DNA methylation of CDH1 gene was investigated in 950 samples, including 620 bladder cancer samples, 199 normal adjacent samples, and 131 normal urothelium samples. The classical methylation-specific polymerase chain reaction (MSP) was performed in eight studies, while quantitative MSP (QMSP) was used in the other two studies. The characteristics and methodological quality of the included studies are summarized in Tables 1 –3.

Flowchart of the literature search and study selection.
SNP, single-nucleotide polymorphism; NOS, the Newcastle-Ottawa Scale; HB, hospital-based; PB, population-based; PCR-RFLP, polymerase chain reaction–restriction fragment length polymorphism.
TT, tumor tissue; NAT, normal adjacent tissue; NUT, normal urothelium tissue; M, male; F, female; MSP, methylation-specific PCR; Q-MSP, quantitative methylation-specific PCR.
CDH1 −160C/A polymorphism and susceptibility to bladder cancer
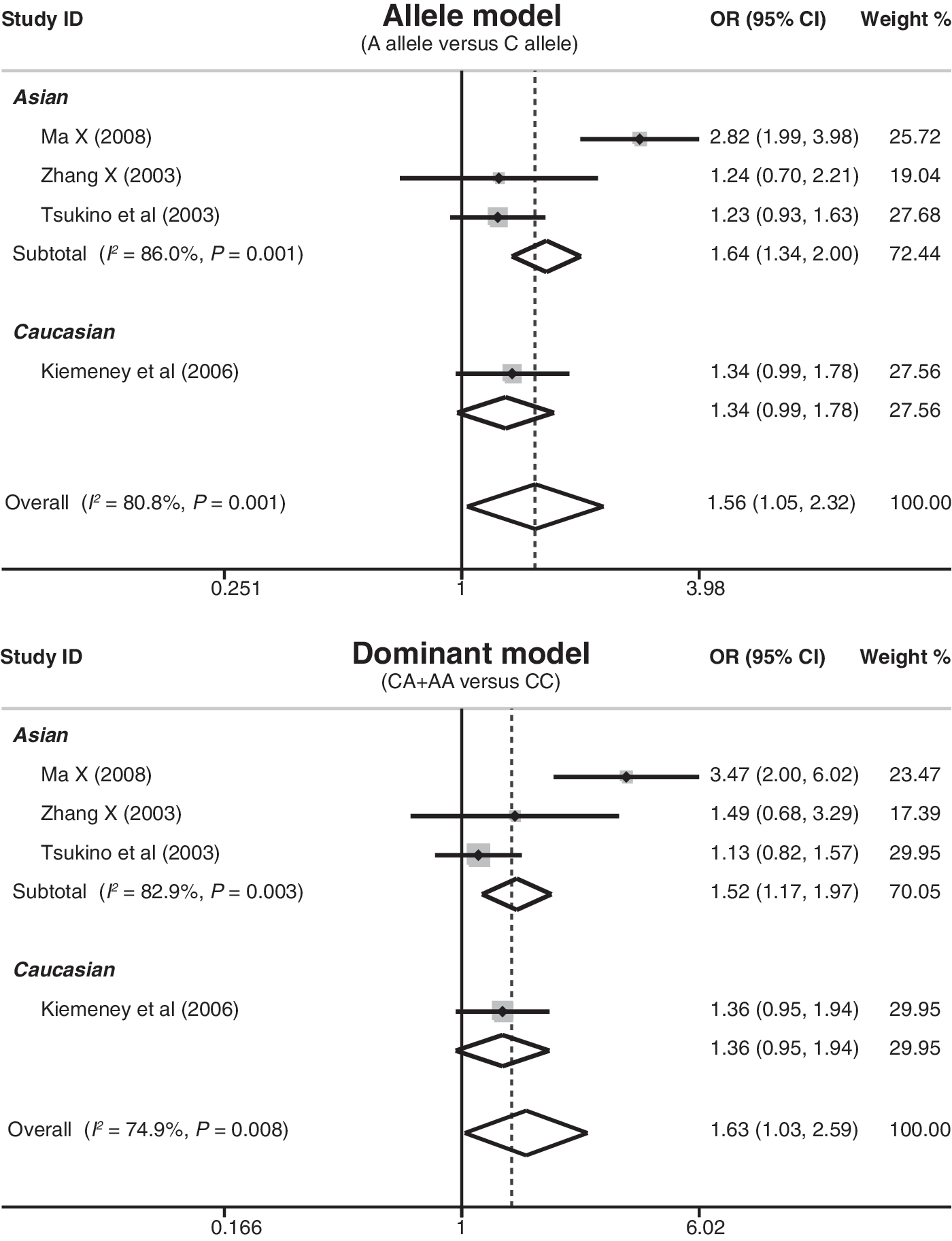
The role of the CDH1 promoter −160C/A polymorphism in bladder carcinogenesis is discussed in four case–control studies. Since heterogeneity obviously existed, which could be a result of differences in ethnicity, country, source of controls, and genotype methods, the random-effect model was conducted. The meta-analysis results revealed that the A variant of CDH1 −160C/A polymorphism may be associated with an increased risk of bladder cancer (A allele vs. C allele: OR=1.56, 95% CI: 1.05–2.32, p=0.027) (Fig. 2). Subgroup analyses showed significant associations between the CDH1 −160C/A polymorphism and bladder cancer risk in the population-based, PCR-RFLP, and direct DNA sequencing subgroups (as shown in Table 4). Although no significant associations were found in the hospital-based subgroup (all p>0.05), these results might still lack sufficient reliability due to the small sample size.
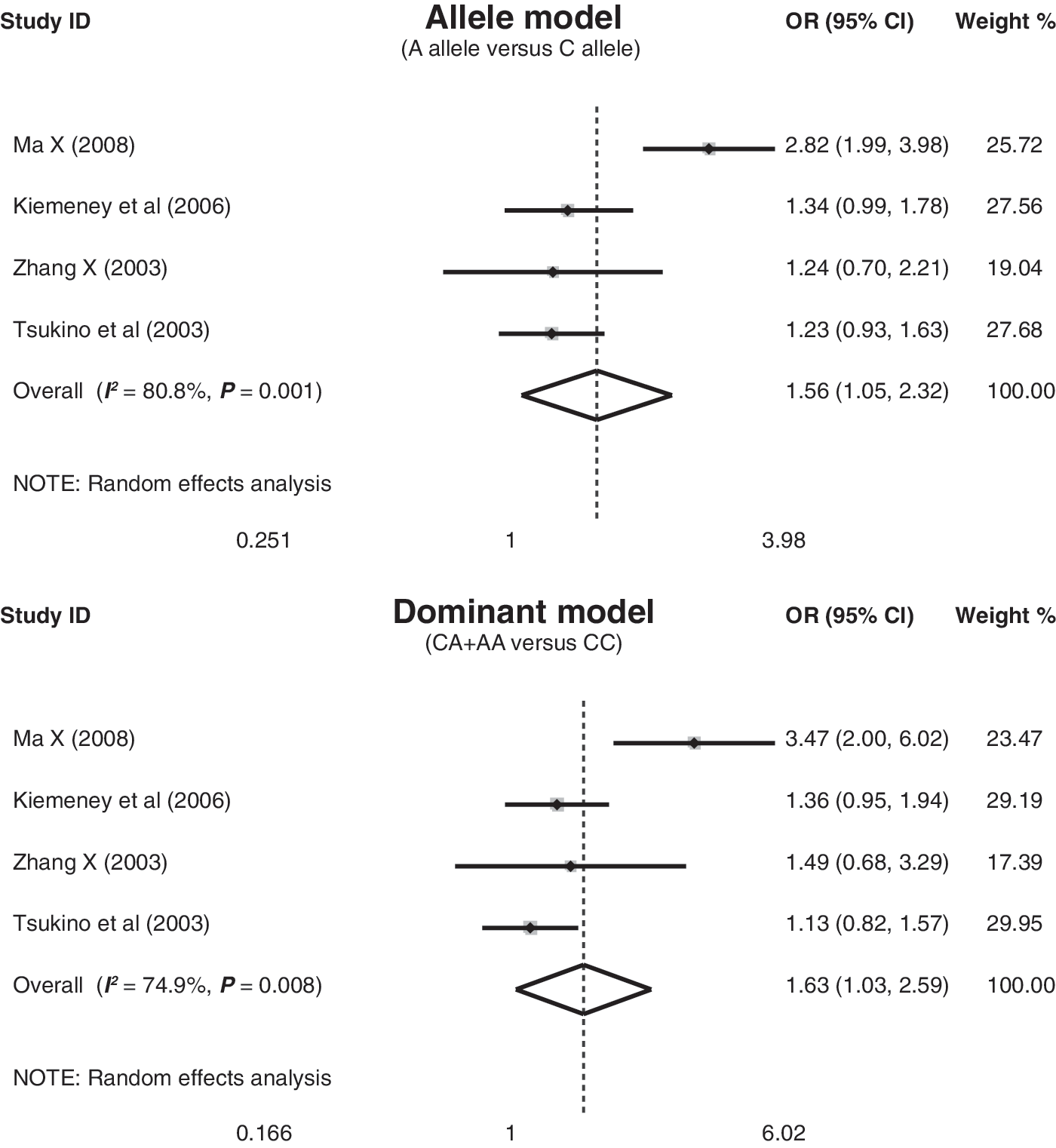
Forest plots for the associations between CDH1 promoter −160C/A polymorphism and bladder cancer risk under the allele and dominant models. The squares and horizontal lines correspond to the study-specific odds ratio (OR) and 95% confidence interval (CI). The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
OR, odds ratio; 95% CI, 95% confidence interval.
CDH1 −160C/A polymorphism and pathological stage of bladder cancer
There were four studies that refer to the association between the CDH1 −160C/A polymorphism and pathological stage of bladder cancer. All the four studies were conducted in Asian populations (Fig. 3). This meta-analysis revealed statistically significant differences in genotype distribution between superficial and invasive bladder cancers. The CDH1 −160A allele and genotype frequencies in patients with invasive bladder cancer were higher than those with superficial bladder cancer (allele frequency: OR=2.12, 95% CI: 1.13–3.99, p=0.020; genotype frequency: OR=2.55, 95% CI: 1.11–5.89, p=0.028) (Fig. 4).
Subgroup analysis by ethnicity for the role of CDH1 promoter DNA methylation in bladder carcinogenesis. The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
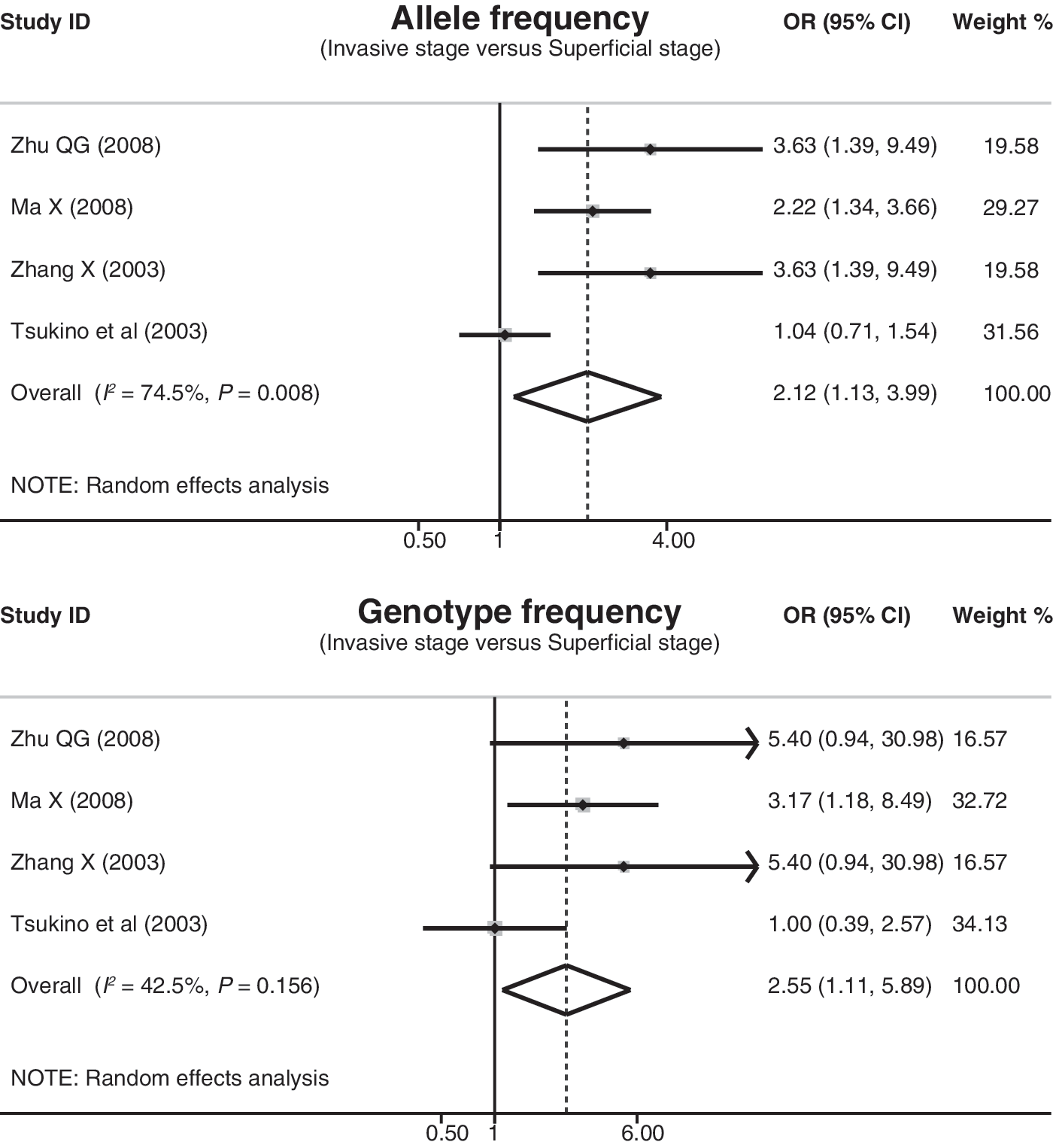
Forest plots for the associations between CDH1 promoter −160C/A polymorphism and pathological stage of bladder cancer under the allele and homozygous models. The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
CDH1 promoter DNA hypermethylation in bladder carcinogenesis
Ten cohort studies that refer to the role of CDH1 promoter DNA methylation in bladder carcinogenesis were assessed. Heterogeneity was significantly observed, so the random-effect model was used. The pooled estimate indicated that the methylation frequencies in bladder cancer tissues were significantly higher than those in normal control tissues (OR=3.03, 95% CI: 1.10–8.32, p=0.031). To explore potential sources of heterogeneity, we also performed subgroup analyses based on ethnicity, source of samples, and detection methods. Subgroup analysis by ethnicity indicated a higher methylation frequency observed among Asian populations (OR=3.70, 95% CI: 1.36–10.09, p=0.011), but not among Caucasian populations (OR=2.22, 95% CI: 0.38–12.91, p=0.375) (Fig. 5). Further subgroup analyses based on source of samples and detection methods also showed significant differences in the methylation frequencies between bladder cancer tissues and normal control tissues in the urothelium tissues and MSP method subgroups (Figs. 6 and 7). However, no evidence of any differences in the adjacent tissues and QMSP method subgroups (all p>0.05) was found.

Subgroup analysis by ethnicity for the role of CDH1 promoter DNA methylation in bladder carcinogenesis. The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.

Subgroup analysis by source of samples for the role of CDH1 promoter DNA methylation in bladder carcinogenesis. The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
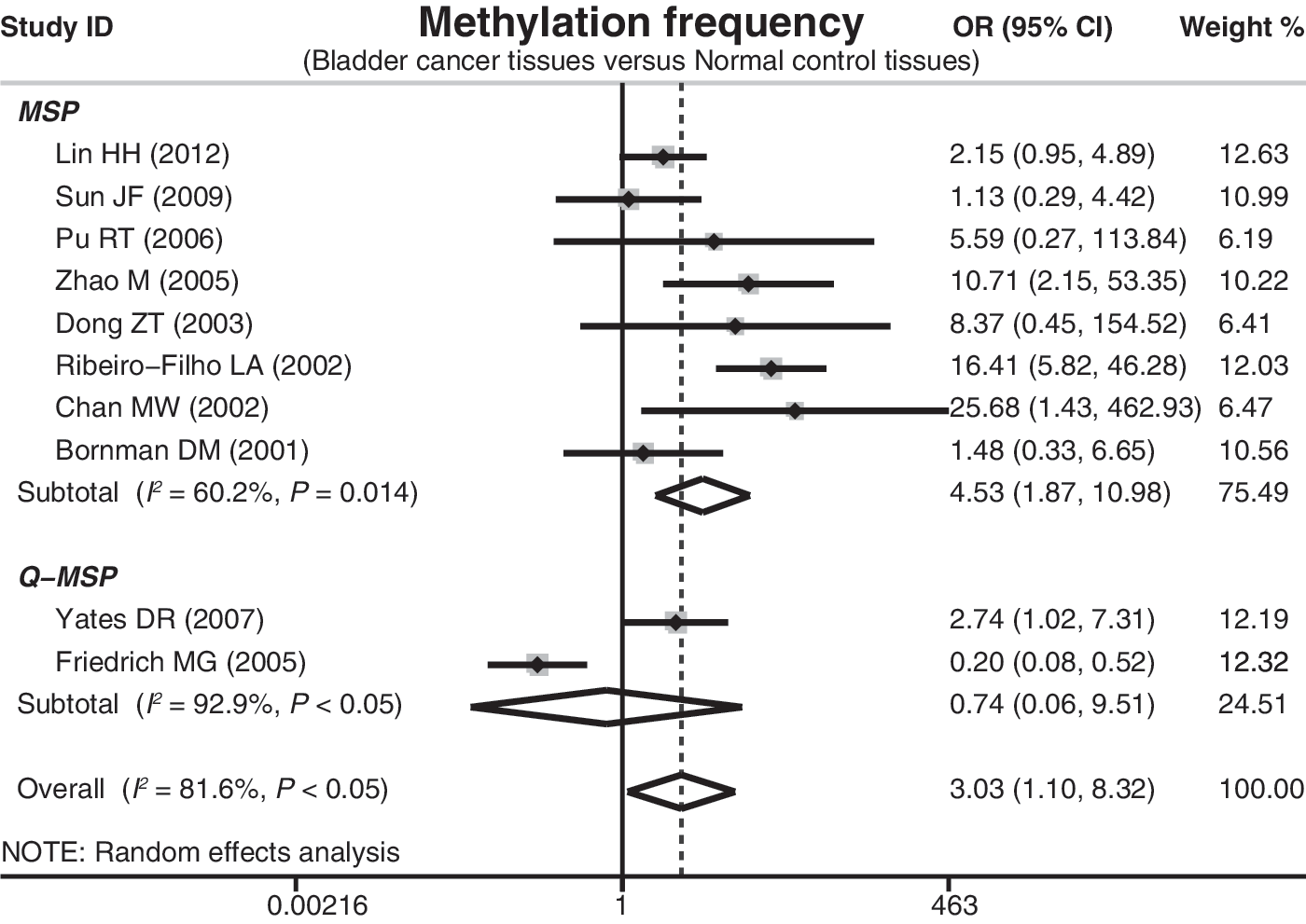
Subgroup analysis by detection methods for the role of CDH1 promoter DNA methylation in bladder carcinogenesis. The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
Evaluation of heterogeneity and publication bias
Sensitivity analysis was also performed to assess the influence of each individual study on the pooled OR by omitting each individual studies in turn to assess the quality and consistency of the results. Although the lower limit of 95% CI is<1 after omitting some studies, the overall trend in ORs is still larger than 1. The analysis results suggested that no individual studies significantly affected the pooled ORs (Fig. 8). Funnel plots and Egger's linear regression test were used to assess potential publication bias in the included studies. The shapes of the funnel plots did not reveal any evidence of obvious asymmetry (Fig. 9). Egger's test also did not display strong statistical evidence for publication bias (all p>0.05).
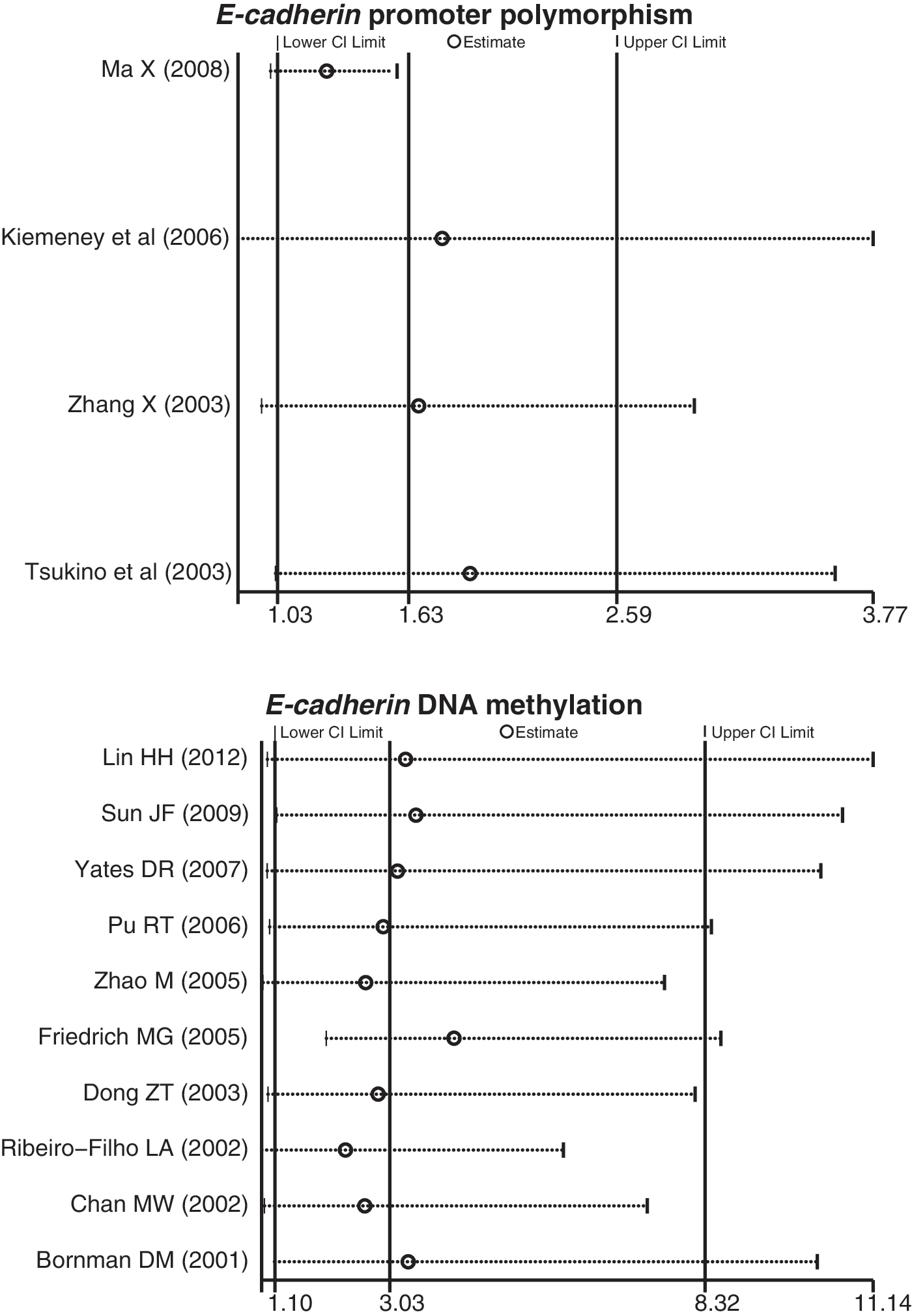
Sensitivity analysis for the pooled estimates of the role of CDH1 promoter polymorphism and methylation in bladder carcinogenesis. Results were computed by omitting each study in turn. Meta-analysis random-effect estimates (exponential form) were used. The two ends of the dotted lines represent the 95% CI.
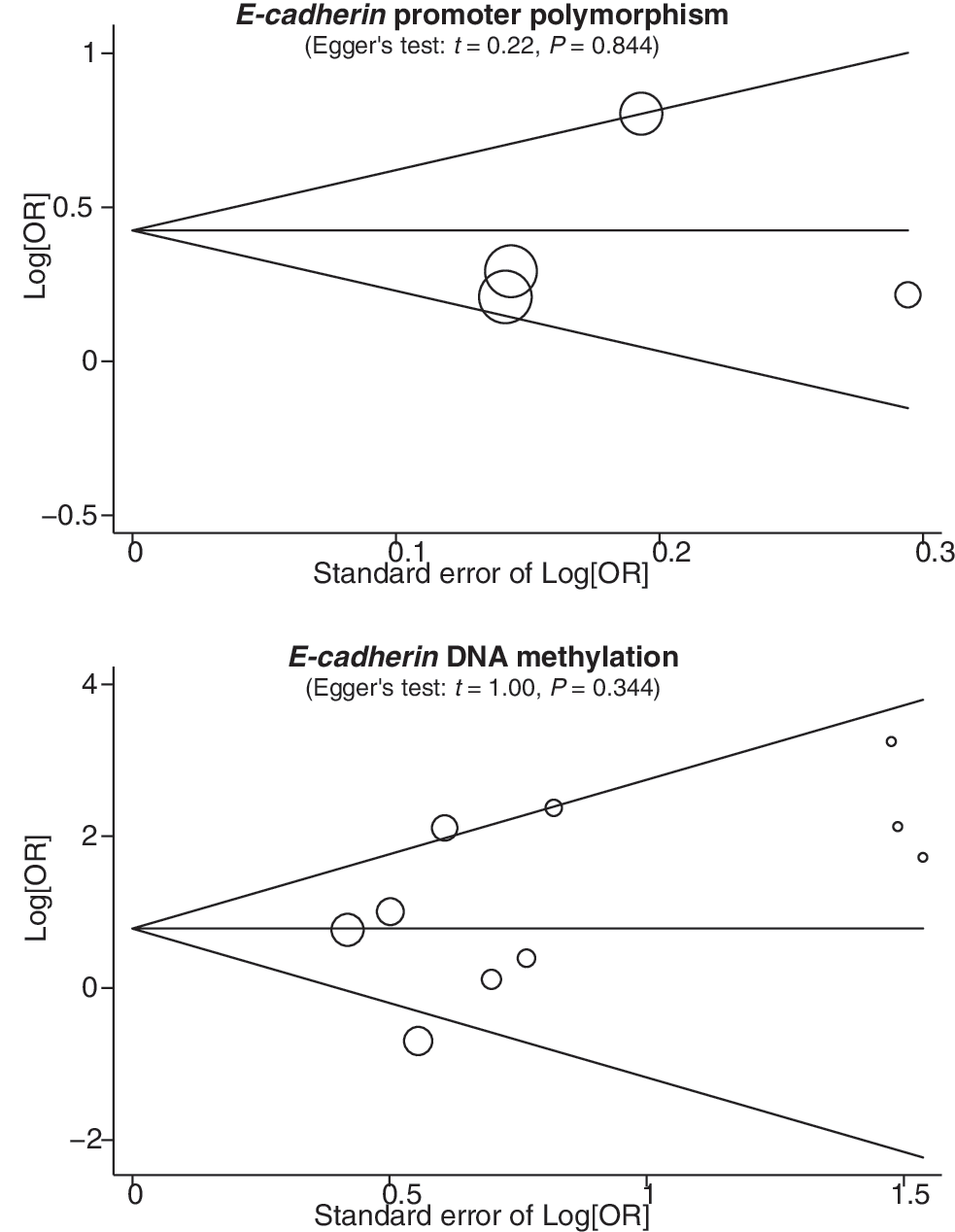
Funnel plots of the meta-analysis for the pooled estimates of the role of CDH1 promoter polymorphism and methylation in bladder carcinogenesis. Each point represents a separate study for the indicated association. Log[OR], natural logarithm of OR. Horizontal line, mean magnitude of the effect. Note: Funnel plot with pseudo 95% confidence limits was used.
Discussion
The tumor-suppressor protein E-cadherin, a cell surface glycoprotein responsible for Ca2+-dependent intercellular adhesion, plays an important role in the growth, invasion, and metastasis of human cancers (Garcia del Muro et al., 2000). Previous studies have demonstrated the critical step of the loss of E-cadherin function in promoting epithelial cells into a more malignant phenotype, thereby promoting the development and metastasis of human cancers through multiple downstream transcriptional pathways (Hirohashi and Kanai, 2003; Jeanes et al., 2008). Recent advancements in the rapidly evolving field of cancer genetics and epigenetics have described extensive reprogramming of every component of the detailed biological mechanisms of cancer development and progression, such as genetic polymorphism and DNA demethylation (Watanabe and Maekawa, 2010). DNA methylation is the earliest and most extensively studied epigenetic change in human cancer (Lin et al., 2012). Silencing of the CDH1 gene by DNA methylation around the promoter region in human carcinomas occurs frequently, including bladder cancer (Bornman et al., 2001). It has been hypothesized that the promoter region of the CDH1 gene is responsible for interindividual variation in the production of CDH1 and in turn leads to individual susceptibility to various cancers (Chik et al., 2011). Many previous genetic studies have also suggested that CDH1 promoter polymorphism −160C/A may play an important role in bladder carcinogenesis (Tsukino et al., 2003; Zhang et al., 2003; Kiemeney et al., 2006; Ma et al., 2008). There is a compelling biological rationale for using CDH1 promoter polymorphism and DNA methylation to hinder tumor recurrence, progression, and development of metastases in bladder cancer.
Our meta-analysis suggested that the A variant of the CDH1 −160C/A polymorphism was associated with increased risk of bladder cancer. Additionally, our meta-analysis assessed the association between the CDH1 −160C/A polymorphism and pathological stage of bladder cancer. The results indicated that the −160A variant frequency in invasive bladder cancer was significantly higher than that in superficial bladder cancer, suggesting that −160A variant may be an independent predictor of tumor progression in bladder cancer. These findings are consistent with the previous studies that concluded that the CDH1 −160C/A polymorphism may serve as a diagnostic and prognostic marker of bladder cancer (Zhang et al., 2003).
DNA methylation is a common mechanism in inactivating tumor-suppressor genes in tumor cells. CDH1 promoter DNA methylation may inactivate the expression of the E-cadherin in human bladder cancer. Accumulating data documented that CDH1 promoter DNA methylation seems an attractive biomarker in bladder cancer and can be identified at an early stage of the disease. Our meta-analysis confirmed that the methylation frequencies in bladder cancer tissues were higher than those in normal control tissues, indicating the prognostic importance of CDH1 promoter DNA methylation in bladder carcinogenesis. It is possible that the methylation of CDH1 represents an early epigenetic change in urothelial carcinogenesis, thus showing high prevalence in some morphologically benign cases. Further subgroup analyses revealed that ethnicity, source of samples, and detection method may be potential sources of heterogeneity.
Our meta-analysis has several limitations that should be acknowledged. First, there were only 15 studies (only four case–control studies) included in this meta-analysis, so the number of included studies was relatively small and may not provide sufficient statistical power in estimating the role of the CDH1 gene promoter polymorphism and DNA methylation in bladder carcinogenesis. Therefore, more studies with larger sample size are still needed to accurately provide a more representative statistical analysis. On the other hand, as a type of a retrospective study, a meta-analysis of summary data from previously published studies may encounter recall or selection bias, thereby possibly influencing the reliability of the results. Third, our meta-analysis was based on unadjusted estimates because all of the published data presented adjusted estimates and if they did, then the estimates were not adjusted by the same potential confounders, such as ethnicity, age, gender, geographic distribution, smoking, and others. Nevertheless, it is well acknowledged that many other factors, such as gene–gene or gene–environment interactions could also affect bladder cancer susceptibility and prognosis. Finally, although all cases or controls of each study were well defined with similar inclusion criteria, there may have been other potential factors (such as differences in sample size, sex ratio, histological type, etc.) not taken into account that may influence our results.
In conclusion, our meta-analysis indicates that the CDH1 −160C/A polymorphism and promoter DNA methylation may be involved in the development and progression of bladder cancer. CDH1 gene promoter polymorphism and DNA methylation may serve as promising biomarkers for the diagnosis and prognosis of bladder cancer.
Footnotes
Acknowledgments
The authors would like to acknowledge the helpful comments on this article received from reviewers. We thank all our colleagues working in the Department of Urology, The First Affiliated Hospital of China Medical University.
Disclosure Statement
All authors declare that there are no conflicts of interest.