
Abstract
Acute lung injury (ALI) is a severe form of diffuse lung disease, which imposes a substantial health burden all over the world. The immune system plays a key role in the development of ALI. The aim of the study was to investigate the expression of cytotoxic T-lymphocyte antigen 4 (CTLA4) in ALI. Levels of CTLA4 were tested on CD4+ and CD8+ T cells in 62 ALI cases and 75 healthy controls by flow cytometry. Data revealed that prevalence of CTLA4 on CD4+ T cells was significantly increased in ALI patients (3.7%±2.1%) than in controls (0.7%±0.3%). Similarly, the proportion of CTLA4 on CD8+ T cells was also significantly elevated in cases (1.0%±0.4% versus 0.5%±0.1%, p<0.05). Further analysis showed that the frequency of CTLA4+CD4+ T cells was positively correlated with the score of Acute Physiology and Chronic Health Evaluation II (APACHE II) (p=0.0005). In addition, when investigating CTLA4 expression with ALI patient mortality, we observed that the level of CTLA4+CD4+ T cells in patients was higher at the time before death than at the time of recruitment (p=0.001). These data suggested that CTLA4 was involved in the pathogenesis and progression of ALI and could be used as a potential target for treating this disease.
Introduction
Cytotoxic T-lymphocyte antigen 4 (CTLA4), the homologue of the T-cell costimulatory molecule CD28, is an important negative regulator of T cells, preventing or terminating activation (Evans et al., 1997). Views on the mechanism of this vary, but three possibilities have been described (Gajewski et al., 2006). First, by competing for their shared ligands, CTLA4 may act by depriving the cell of CD28-mediated costimulation (Greenwald et al., 2002). Second, CTLA4 ligation by CD80 and CD86 may trigger a distinct, negative, signaling pathway, or interfere with an activating pathway, thus inhibiting activation downstream of the T-cell receptor (TCR) (Greenwald et al., 2002; Hadinia et al., 2007). For example, recently, CTLA4 has been shown to attenuate TCR signaling by inhibiting the upregulation of signaling raft domains in human T cells (Hiraoka et al., 2006). Third, ligation of CTLA4 on regulatory T cells may induce the production of a factor(s) that inhibits the activation or proliferation of neighboring cells (Krummel and Allison, 1996; Hodi et al., 2003). It is likely that some or all of these mechanisms apply. Whatever its mode of action, CTLA4 has been implicated in the maintenance of peripheral tolerance and anergy induction (Leach et al., 1996; Ligers et al., 2001; Liu et al., 2011).
Previous studies showed that lymphocytes, in addition to neutrophils, infiltrate the lung in ALI models (Mohammed et al., 2000; Hotchkiss et al., 2001; Schwulst et al., 2008). Recently, Nakajima et al. (2013) demonstrated that T-cell pathways involving CTLA4 may contribute to a murine model of LPS-induced ALI. Analysis of additional T-cell subsets in human ALI remains ill defined. In the current study, we investigated CTLA4 expression on CD4+ and CD8+ T cells in ALI patients and healthy controls, and analyzed the CTLA4 level with the progression of this disease.
Materials and Methods
Study population
All patients were recruited from the Emergency Center, Surgical and Respiratory ICU at Shanghai East Hospital, Tongji University. Definition of ALI was in accordance with the American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference, and the American-European Consensus Conference statements. Exclusion criteria included ages less than 18 years, pregnancy, diffuse alveolar hemorrhage, severe chronic respiratory disease, directive to withhold intubation, severe chronic liver disease (defined as a Child–Pugh score of >10), malignancy, using of chronic high-dose immunosuppressive therapy (steroids with equivalent prednisone >0.5 mg/kg per day or cytotoxic agents for immunologic disorders), and AIDS patients. Subjects with a minimum 15-pack year smoking history were defined as smokers. Clinical and demographic data at baseline, including Acute Physiology and Chronic Health Evaluation (APACHE) II scores, organ failure, previous health status, and hospital and ICU mortality, were obtained after the patient met the inclusion criteria. The control group was recruited from people who came to the same hospital for a general health examination. Individuals who had any recent acute illness, any chronic illness, or a history of ALI were excluded. All participants provided informed consent and the University and Institutional Review Boards approved this research project.
Detecting CTLA+CD4+ and CTLA+CD8+ T cells
Peripheral blood was obtained from patients before any intervention and from controls at their convenience. Peripheral blood was also collected from patients every 7 days for 2 months after recruitment. The mononuclear ring was collected after Ficoll hypaque gradient centrifugation. The cells were washed twice with a washing and staining solution (PBS 1%, BSA 1%, and sodium azid 0.1%), and viability was checked being more than 95% by trypan blue exclusion assay. For surface antigen staining, the cells were then incubated, 30 min in dark, with fluorochrome-conjugated antibodies to surface antigens (CD4, CD8, and CTLA4). The dye format antibodies used in this study were mouse antihuman CTLA4-PE, CD4-PerCP, CD8-PerCP, and matched isotype control antibodies for setting the quadrant marker and excluding the background staining during the analysis. All tubes were finally fixed and analyzed by the FACSCalibur flow cytometer equipped with argon ion laser (BD Biosciences). At least 20,000 events were collected during acquisition. The CellquestPro software package (BD Biosciences) was used for data acquisition and analyses.
Statistical analysis
All data were analyzed using the GraphPad Prism 5 (GraphPad Software, Inc.). The student's t test and the Mann–Whitney nonparametric U test were used for comparison between groups. A value of p<0.05 is considered as a significant difference.
Results
Characteristics of the study population
The distributions of selected characteristics of the cases and controls are presented in Table 1. A total of 62 ALI cases and 75 healthy controls were recruited in the study. The mean age of patients and controls was 65.2±12.3 and 64.6±11.5, respectively. No significant differences were observed with regard to age, sex, and body mass index, whereas cases had more smoking history than controls. Of the 62 ALI patients, 9 (14.5%) subjects had diabetes; 3 (4.8%) subjects had liver cirrhosis; the average score of APACHE II was 19.6, and mortality in 60 days was 41.9%.
ALI, acute lung injury; BMI, body mass index; APACHE II, Acute Physiology and Chronic Health Evaluation II.
CTLA4 expression on peripheral CD4+ and CD8+ T cells in ALI patients and controls
To understand the effect of CTLA4 on ALI, we first investigated the expression levels of CTLA4 on CD4+ T cells and CD8+ T cells from the PBMC of ALI cases and healthy controls. As shown in Figure 1A, increased proportion of CTLA4+ cells was detected on CD4+ T cells in ALI patients than in controls (mean±standard deviation [SD] 3.7%±1.9% vs. 0.7%±0.3%, p<0.01). Similarly, the expression of CTLA4 in CD8+ T cells was also significantly upregulated in cases compared to controls (1.0%±0.4% vs. 0.5%±0.1%, p<0.05) (Fig. 1B). These results indicated that CTLA4 may be involved in the pathogenesis of ALI by its regulation on various immune cells.
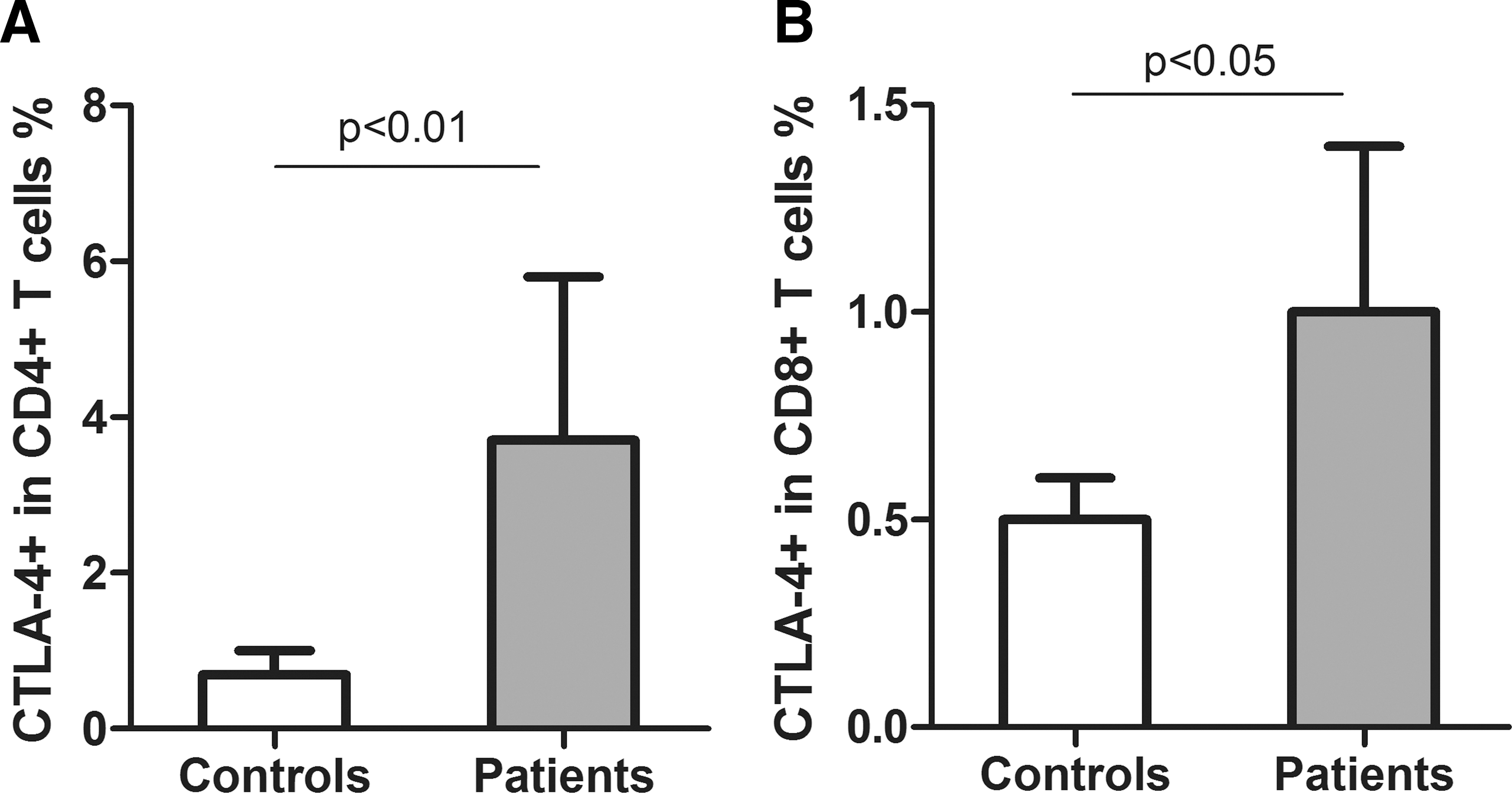
CTLA4 expression on CD4+ and CD8+ T cells in peripheral blood of ALI patients and healthy controls.
CTLA4 expression in patients with different smoking status
Since smoking is one of the established risk factor for ALI, we investigated whether smoking may affect CTLA4 and cause ALI. We compared CTLA4 expression on CD4+and CD8+ T cells in ALI patients with different smoking status. Data showed that the proportion of CTLA4+CD4+T cells was 4.1%±2.3% in smokers and 3.4%±1.5% in nonsmokers. No significant difference was observed (Fig. 2A). Similarly, CTLA4+CD8+ T cells were not significantly changed between cases with different smoking status (Fig. 2B). These data suggested that smoking may not affect the CTLA4 expression on CD4+ and CD8+ T cells in ALI cases.
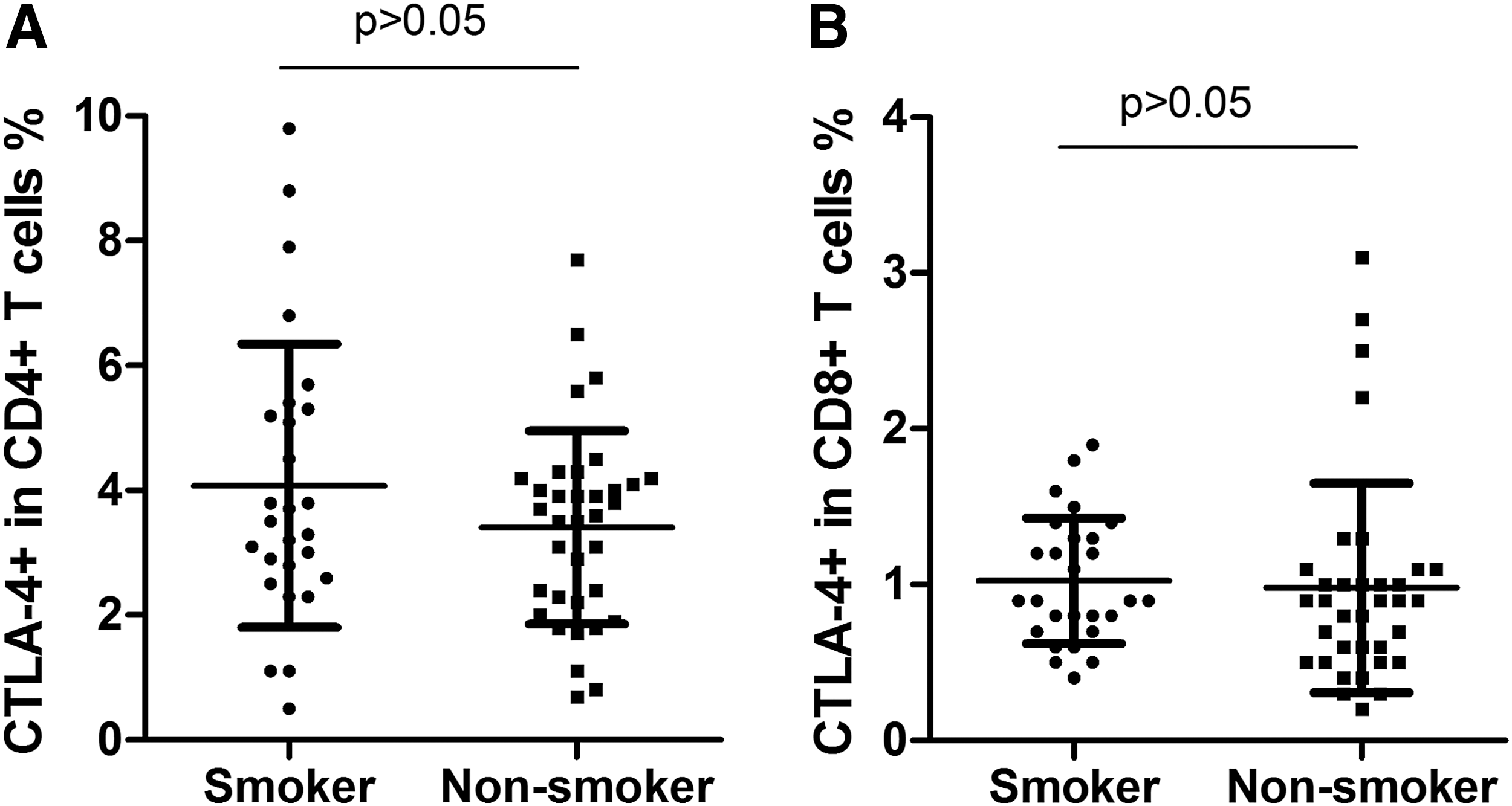
Comparison of CTLA4 expression on CD4+
CTLA4 expression in ALI patients with different APACHE II scores
APACHE II is a severity-of-disease classification system. Higher scores correspond to more severe disease and a higher risk of death. We observed a positive correlation between CTLA4+CD4+ T cells and APACHE II scores of the patients (p=0.0005, Fig. 3A), indicating that augmenting of CTLA4 in CD4+ T cells may be involved in the progression of ALI. However, our data did not reveal any significant correlation between CTLA4+CD8+ T cells and APACHE II scores of the patients (p=0.226, Fig. 3B), suggesting that CTLA4 may play less important roles on CD8+ T cells in the development of ALI.
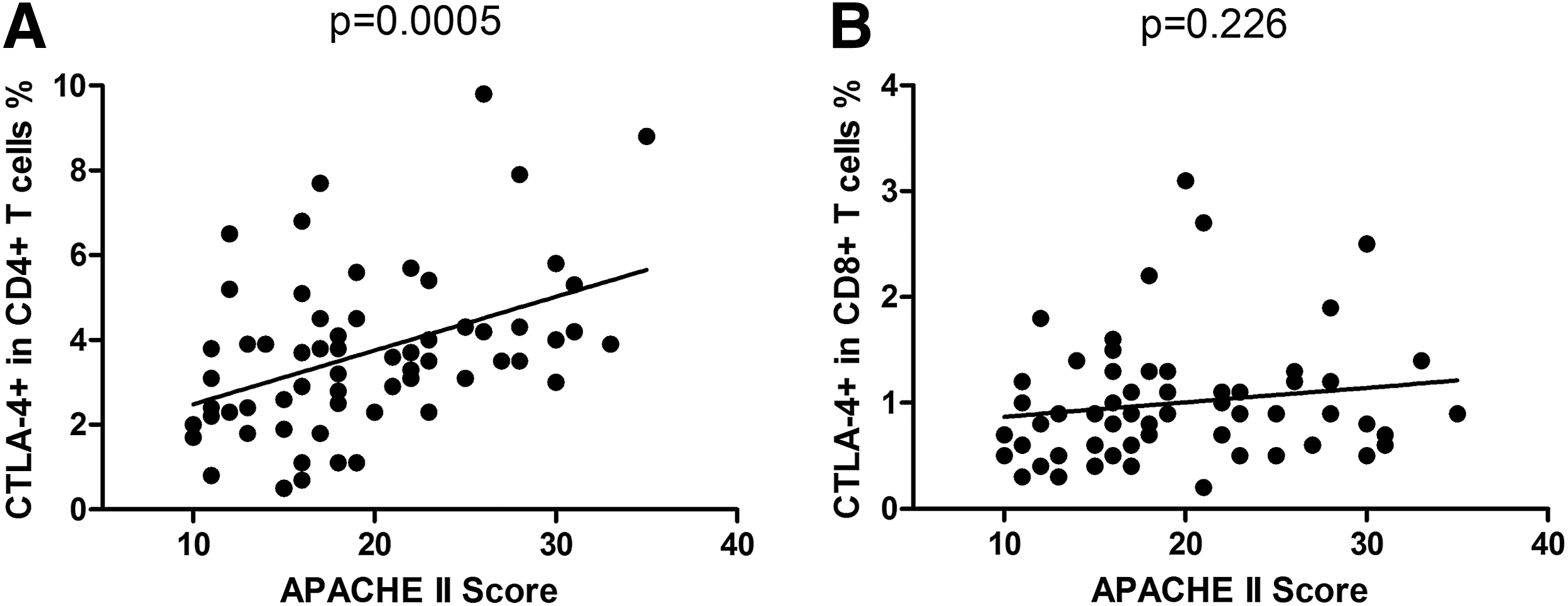
Correlation of CTLA4 expression on CD4+
CTLA4 expression in ALI mortality
To further understand the association between CTLA4 expression and the progression of ALI, we continued to collect blood from patients every 7 days for 60 days after the recruitment. During this period, 26 patients were dead. Of them, we compared the CTLA4 level between the blood gathered the last time and the blood collected at recruitment. Results demonstrated that patients who were dying had a significantly higher level of CTLA4 on CD4+ T cells than the time of recruitment (p=0.001, Fig. 4A). However, a significant change of CTLA4 on CD8+ T cells was not identified in patients with different time points (p=0.558, Fig. 4B). These data further confirmed that CTLA4 expression on different subsets of T cells may have various effects on the progression of ALI. In addition, the CTLA4 level of the 26 cases who died during the research was 3.9%±2.2% in CD4+ T cells, and 1.1%±0.6% in CD8+ T cells at the time of recruitment. The values were higher, but not significantly higher than the average of the cases, indicating that the expression of CTLA4 may accelerate at the late stage of the disease.

Comparison of CTLA4 expression on CD4+
Discussion
The pathogenesis of ALI is still unclear. CTLA4 plays critical roles in downregulating immune responses and therefore may affect the development of ALI. In this study, we investigated the expression of CTLA4 in both CD4+ and CD8+ T cells of ALI patients and identified that CTLA4 expression was significantly increased on CD4+ and CD8+T cells in ALI cases. In addition, our data revealed that the upregulation of CTLA4 on CD4+ T cells was correlated with the severity and mortality of ALI.
Innate and adaptive immune responses to invading microbes (e.g., Gram-negative bacteria) are tightly interwoven and engage the total immunological capability of the host (Tivol et al., 1995; Sun et al., 2008; Royal et al., 2010). Innate immunity is the first line of lung defense, and it includes structural barriers, alveolar macrophages, neutrophils, NK cells, and dendritic cells. Adaptive immunity, which is promoted by innate immunity, is composed of Ag-specific lymphocytes that eliminate or prevent pathogenic challenges (Oosterwegel et al., 1999; Ueda et al., 2003). Lymphocytes, including T and B cells, are major cells of the adaptive immune system. CD8+ T cells destroy virally infected cells and tumor cells (Nishikawa et al., 2005). However, CD4+ T lymphocytes have no cytotoxic or phagocytic activity and cannot kill infected cells or clear pathogens, but they manage the immune response by directing other cells to perform these tasks. Experimental depletion of CD4+ T lymphocytes in mice with staphylococcus aureus pleural empyema is associated with decreased bacterial clearance (Liyanage et al., 2006; Loos et al., 2008). Sepsis, one of the main causes of ALI, induces a striking depletion of lymphocytes, leading to an inability of the host to combat the ongoing source of infection and predisposing to secondary opportunistic infections (Hotchkiss et al., 2001). In addition, sepsis activates the remaining lymphocytes (Hotchkiss et al., 2001), and inhibition of lymphocyte apoptosis may improve sepsis outcomes (Hotchkiss et al., 2001). Infection is a precipitating factor for ARDS, and T cells are considered to play an important role in host defense for infection. In the current study, we identified that both CTLA4+CD4+ and CTLA4+CD8+ T cells were significantly increased in ALI. These data were in accordance with a recently published article showing elevated CTLA4 expression on CD4+ T cells in a murine model of LPS-induced ALI (Nakajima et al., 2013). Interestingly, our results revealed that the increase of CTLA4 on CD4+ T cells (5.3-fold) is higher than that on CD8+ T cells (2.0-fold, Fig. 1), suggesting that CTLA4+CD4+ T cells may play a more important role in the pathogenesis of ALI. Our further analysis demonstrated that a proportion of CTLA4+CD4+ T cells, but not CTLA4+CD8+ T cells was positively correlated with APACHE II scores and patients mortality, indicating that CTLA4 may selectively affect the subsets of T cells and influence the progression of the disease.
In conclusion, the study identified that expression of CTLA4 was upregulated on CD4+ T and CD8+ T cells in peripheral blood of ALI. In addtion, the elevation of CTLA4 was further observed on CD4+ T cells of ALI patients with worse progression. Our data suggest a potential mechanism of the pathogenesis of ALI and provide a possible target for the treatment of this disease.
Footnotes
Disclosure Statement
No competing financial interests exist.