
Abstract
Psoriasis is caused by a combination of genetic, immunologic, and environmental factors. The vitamin D receptor (VDR) is involved in antiproliferative and prodifferentiation pathways in keratinocytes and exerts immunosuppressive effects. We aimed to investigate possible associations between VDR polymorphisms and psoriasis susceptibility and to evaluate functional effects of potential psoriasis-associated polymorphisms. We genotyped 108 patients with psoriasis and 268 healthy controls at 5 VDR polymorphisms (A-1012G, FokI, BsmI, ApaI, and TaqI) by TaqMan allelic-discrimination real-time polymerase chain reaction. We found a significant increased overall risk of psoriasis for the VDR A-1012G promoter polymorphism (odds ratio [OR]=2.43, 95% confidence interval [CI]: 1.15–5.13; p=0.05). A significant higher frequency (p=0.035) of the A allele was found in psoriatic cases compared with controls. In a case–case analysis, a statistically significant association between A-1012G and family history emerged (p=0.033). Furthermore, a significant association of A-1012G risk genotypes with a lower expression of VDR mRNA emerged (p=0.0028). Our data show that VDR promoter A-1012G polymorphism is associated with psoriasis risk and suggest that this polymorphism may modulate psoriasis risk by affecting VDR expression.
Introduction
P
The vitamin D receptor (VDR) is an intranuclear receptor that regulates gene transcription of vitamin D responsive genes together with its ligand, the active hormone 1,25-dihydroxyvitamin D3 (1,25(OH)2D3). The receptor–hormone complex binds to hormone response elements in regulatory regions of target genes modulating gene transcription. The 1,25(OH)2D3 signaling is of wide interest in psoriasis because of the antiproliferative and prodifferentiation effects of 1,25(OH)2D3 on keratinocytes (Hosomi et al., 1983; Smith et al., 1986) and its immunosuppressive effects (Deluca and Cantorna, 2001; Mathieu and Adorini, 2002; Mathieu et al., 2004). VDR is expressed in different tissues and cells, including normal (Stumpf et al., 1979; Feldman et al., 1980) and psoriatic (Milde et al., 1991; Sølvsten et al., 1996) keratinocytes and in cells of the immune system (monocytes, macrophages, and T lymphocytes) (Wang et al., 2012). Topical 1,25(OH)2D3 and its analogs are effective for the treatment of psoriasis (Kragballe et al., 1991) and, interestingly, treatment response has been shown to diversify with keratinocyte VDR mRNA expression (Chen et al., 1996). Thus, VDR may represent a candidate-modifying gene in psoriasis.
The VDR gene, located on chromosome 12q13.11, has more than 200 single-nucleotide polymorphisms (SNPs) (Nejentsev et al., 2004). A few VDR SNPs have been studied for their potential associations with susceptibility to several immune-mediated diseases, including psoriasis, severe atopic dermatitis, allergic asthma, and atopy, suggesting that VDR may contribute to the control of these diseases by the regulation of the epidermal barrier function and/or local immune response (Poon et al., 2004; Heine et al., 2013). Most of the studies focused on four SNPs: rs2228570:C>T, detected with FokI restriction enzyme and located at exon 2 initiation codon; rs1544410:G>A and rs7975232:T>G, detected with BsmI and ApaI restriction enzymes, respectively, and located at intron 8; rs731236:T>C, detected with TaqI restriction enzyme and located at exon 9 (Rucević et al., 2009).
To date, the majority of the studies evaluating associations between VDR SNPs and risk of psoriasis has provided inconsistent and contrasting results (Saeki et al., 2002; Dayangac-Erden et al., 2007; Rucević et al., 2009; Acikbas et al., 2012; Lee et al., 2012; Liu et al., 2013).
The functional significance of these polymorphisms is not completely known. The C>T substitution at FokI site, which results in a new start codon, is known to increase the overall length of VDR transcript by nine base pairs, resulting in a longer protein with lower transcriptional activity (Whitfield et al., 2001). On the other hand, functional significance of BsmI, ApaI, and TaqI polymorphisms remains unknown (Morrison et al., 1992).
Recently, a novel VDR polymorphism A-1012G (rs4516035:A>G), located in the promoter region, has been identified (Fang et al., 2005; Halsall et al., 2005). The functional role of this promoter variant is still largely unknown.
The aims of the present study were to determine whether the VDR SNPs rs4516035:A>G (A-1012G), rs2228570:C>T (FokI), rs1544410:G>A (BsmI), rs7975232:T>G (ApaI), and rs731236:T>C (TaqI) may confer psoriasis susceptibility, to investigate possible associations with the main clinical–pathological characteristics of psoriasis, and to evaluate potential functional effects of the VDR polymorphism A-1012G (rs4516035:A>G).
Materials and Methods
Study population
In our observational study, we enrolled 108 patients affected with psoriasis and 268 healthy controls, for a total of 376 participants. Thus, we set up a case–control study with a ratio of 1:2.5, to increase the power of the study. All cases and controls were Caucasians and >18 years old at the enrollment in the study. One or more blood sample(s) together with informed consent were obtained from each study participant. The study was approved by the local ethical committee.
Patients were recruited at the Department of Dermatology and Venereology, Policlinico Umberto I of Rome (Rome, Italy). For each patient, we collected the following information: gender, age at onset, type, and severity of the disease (mild or moderate/severe, <10 or ≥10 respectively, referring to Psoriasis Area Severity Index score), family history (FH) of psoriasis, body mass index (BMI; 25–30 kg/m2=BMI for overweight; >30 kg/m2=BMI for obesity), and information about life behaviors (smoke and alcohol consumption). Overall, of the 108 patients, 61 (56.5%) were men and 47 (43.5%) were women. Age at psoriasis onset ranged between 6 and 80 years, with a mean age of 37.8 years. Patients presented more often a moderate/severe (74%), nonarthropathic (64.8%) psoriasis. Thirty-four cases (31.5%) reported a FH of psoriasis in the first-degree relatives. Patients tended to have a normal BMI (54.6%), to be nonsmokers (57.1%), and to not consume alcohol (91.5%).
Control samples came from blood donors, enrolled under other research or clinical protocols at host institution. Overall, 197 (73.5%) were men and 71 (26.5%) were women. Age at blood withdrawal ranged between 19 and 65 years, with a mean age of 53.4 years.
Genotyping analysis
DNA was extracted from peripheral blood lymphocytes using ReliaPrep™ Blood gDNA Miniprep System (Promega, Fitchburg, WI), following the manufacturer's instructions. All DNA samples were quantified by a Qubit 2.0 fluorometer (Life Technologies, Carlsbad, CA).
Cases and controls were genotyped using commercially available assays (Life Technologies) rs4516035:A>G (A-1012G), rs2228570:C>T (FokI), rs1544410:G>A (BsmI), rs7975232:T>G (ApaI), and rs731236:T>C (TaqI), by allelic-discrimination real-time polymerase chain reaction (PCR) with TaqMan probes in an ABI 7500 fast real-time PCR instrument (Life Technologies) as previously described (Ottini et al., 2013).
Gene expression analysis
Peripheral blood mononuclear cells (PBMCs) were isolated from whole blood samples by Ficoll-Paque (GE Healthcare, Little Chalfont, Buckinghamshire, United Kingdom) gradient centrifugation. RNA was then extracted using a standard phenol/chloroform method (Chomczynski and Sacchi, 2006). RNA quality and quantity were assessed by an Agilent 2100 Bioanalyzer with RNA 6000 Nano Assay Kit (Agilent Technologies, Santa Clara, CA).
VDR mRNA expression compared with the housekeeping gene PGK1 as endogenous control was evaluated by one-step quantitative real-time PCR in an ABI 7500 fast real-time PCR instrument (Life Technologies) using Real-Time Ready Taqman assays (Roche, Penzberg, Upper Bavaria, Germany). The fold change in gene expression, normalized to endogenous control, was calculated as ΔCt (±ΔCt standard error [SE]). ΔCt values were then normalized to a control sample, and differences in VDR mRNA expression were calculated using relative quantity (RQ)=2−ΔΔCt.
Statistical analyses
Association between the clinical–pathological characteristics of the psoriasis patients and the severity of the disease was assessed by using the chi-square test.
To avoid any significant differences in the demographic structure of cases and controls, we weighted each subject of the control series. In particular, the weight for the controls was evaluated by considering the ratio between the frequencies of patients with psoriasis and the control ones for each distinct value of gender crossed by the class of age.
To verify the relations between genotypes and psoriasis risk, we evaluated the genotype frequencies for each individual DNA polymorphism in both case and control series. Deviations from Hardy–Weinberg equilibrium in controls were assessed using the chi-square test with one degree of freedom.
Cases and controls were analyzed with a logistic regression model in which we assessed the association between each polymorphisms and the risk of psoriasis; the odds ratio (OR), with a 95% confidence interval (CI), was assessed by using the common homozygote genotype as the reference category. A specific analysis for the alleles, in which we compared the frequencies of the common one with the minor allele, was also performed.
Associations between polymorphisms and clinical features were assessed by using the chi-square statistics and logistic regression.
ANOVA and Kruskal–Wallis tests were used to determine the association of genotypes with VDR mRNA expression. For all the analyses, a p-value≤0.05 was considered statistically significant. Statistical analyses were performed with SAS (SAS/STAT version 9.1) software.
Results
Association of VDR A-1012G with psoriasis risk and clinical–pathological characteristics
To investigate possible associations between VDR polymorphisms and risk of psoriasis, we performed a case–control study including 108 patients with psoriasis and 268 healthy controls. Table 1 shows the clinical–pathological features of the psoriatic patients and their association with the severity of psoriasis. Interestingly, a statistically significant association emerged between severity of psoriasis and BMI (p=0.02).
p-Values<0.05 in bold.
FH, family history; BMI, body mass index.
All 108 cases and 268 controls were genotyped at five SNPs in the VDR gene, including rs4516035:A>G (A-1012G), rs2228570:C>T (FokI), rs1544410:G>A (BsmI), rs7975232:T>G (ApaI), and rs731236:T>C (TaqI). Genotypes distribution was consistent with the Hardy–Weinberg equilibrium among controls.
Estimates for the association between the five SNPs evaluated and psoriasis occurrence are shown in Table 2. We found a significant difference in the distribution of genotypes between normal controls and psoriatic patients for the A-1012G (rs4516035:A>G) polymorphism. In particular, compared with the reference GG genotype, the following ORs were found: AA genotype OR=2.43 (95% CI: 1.15–5.13; p=0.05) and GA genotype OR=2.14 (95% CI: 1.02–4.48; p=0.22). As expected, a statistically significant association between increased psoriasis risk and A-1012G risk genotypes emerged in a multivariate analysis, including terms for all the five genotyped polymorphisms, adjusted for age and sex (OR=1.47, 95% CI: 1.03–2.11; p=0.04).
p-Values<0.05 in bold.
VDR, vitamin D receptor; OR, odds ratio; CI, confidence interval.
A significant association for A-1012G with increased risk of psoriasis emerged also under dominant model (OR for GG vs. GA+AA=2.19, 95% CI: 1.09–4.40; p=0.02) (data not shown).
Considering allelic frequencies, a statistically significant higher frequency of the A allele of A-1012G was found in psoriatic cases compared with controls, indicating an association with increased risk of psoriasis (OR=1.43, 95% CI: 1.02–1.99; p=0.035) (Table 3).
p-Values<0.05 in bold.
We further evaluated the distribution of genotype frequencies for the five VDR polymorphisms in the patients' series, stratified according to clinical characteristics, including severity, gender, age at onset, type of psoriasis, and FH of psoriasis. As shown in Table 4, the prevalence of the AA risk genotype of A-1012G tended to be higher in patients without FH of psoriasis compared with patients with a positive FH (50% vs. 29.4%). A statistically significant association between A-1012G and FH status emerged in the case–case analysis (p=0.033). No significant differences in genotype frequencies were found for FokI, BsmI, ApaI, and TaqI polymorphisms for the above-mentioned characteristics (data not shown).
p-Values<0.05 in bold.
We further investigated whether the risk of severe psoriasis may be modulated by VDR polymorphisms in patients according to gender, class of age, type of psoriasis, BMI, and FH. A statistically significant association between the severity of psoriasis and TT genotype of FokI (rs2228570:C>T) polymorphism emerged when it is considered jointly with the gender (p=0.01), indicating an increased risk of severe psoriasis for male patients harboring TT risk genotype (Supplementary Table S1; Supplementary Data are available online at
Association of VDR A-1012G with variation in VDR mRNA expression levels
We investigated the functional relevance of VDR A-1012G promoter polymorphism by performing a VDR expression analysis in 80 cases for which RNA was available. These cases had been free of any other medical illness, including acute infections and allergic reactions, for at least 1 month before the blood withdrawal. The samples analyzed included 11 (13.8%) GG, 36 (45%) GA, and 33 (41.2%) AA genotype cases. Notably, no difference in treatment modalities (topical, systemic, and biologic agents) existed in the three genotype groups (p=0.35).
The mean ΔCt value (±SE) was 5.08±0.38 for the GG group, 5.72±0.21 for the GA group, and 5.99±0.22 for the AA group, and these differences are statistically significant (p=0.0028). Comparing the VDR mRNA levels among the groups, with GG as the reference category (RQ=1), we found a significant association (p=0.006) of A-1012G risk genotypes with a lower expression of VDR mRNA (Fig. 1). In particular, VDR mRNA expression was dose dependent and decreased with the number of A alleles (RQ for GA group=0.749, p=0.098; RQ for AA group=0.601, p=0.013; Benjamini–Hochberg false discovery rate adjusted p-values). mRNA expression did not vary by disease severity (p=0.28) and treatment modalities (p=0.17).
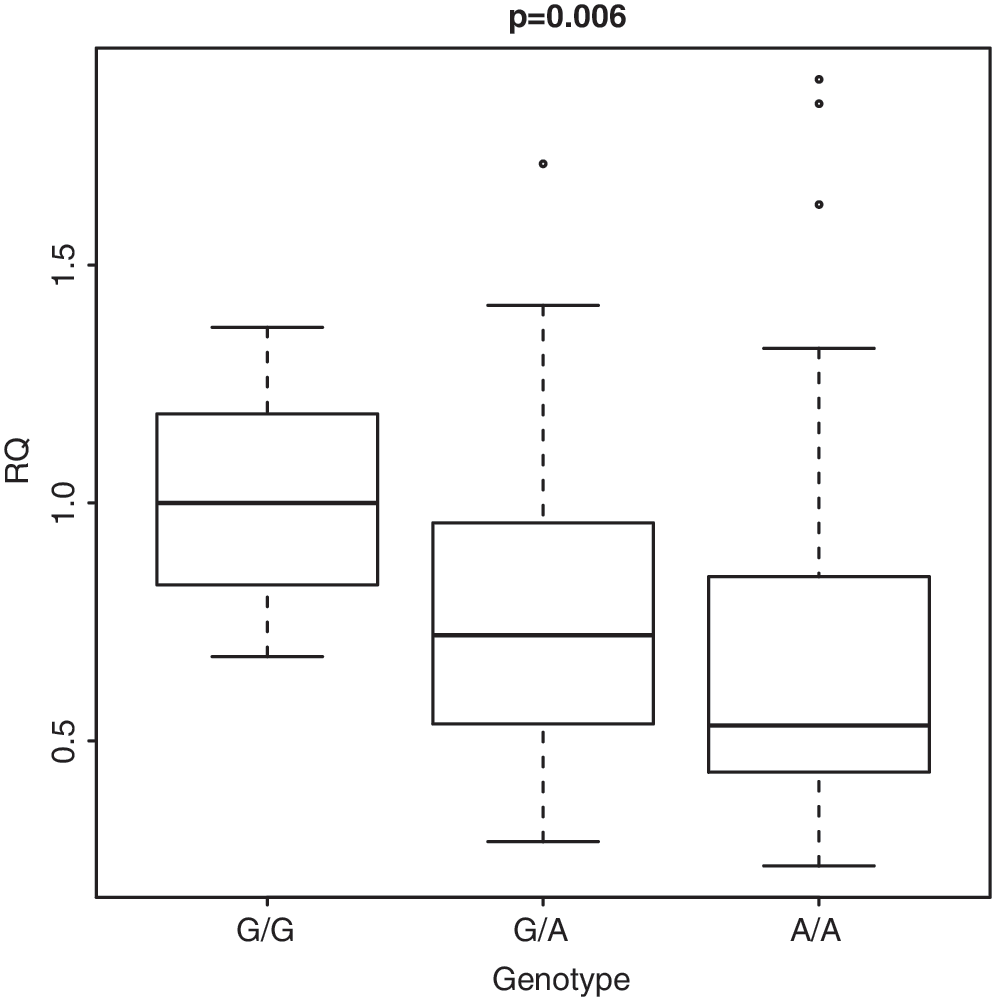
Vitamin D receptor (VDR) mRNA levels expressed as relative quantity (RQ) of 80 samples stratified for the three A-1012G genotypes, with G/G genotype as reference (RQ=1).
Discussion
In this study, we showed that the VDR A-1012G promoter polymorphism may influence psoriasis risk, overall and/or in association with specific clinical–pathological features and, importantly, that this polymorphism affects VDR mRNA expression.
In our series, A-1012G polymorphism was statistically associated with overall psoriasis risk. Our results showed that the A allele is significantly overrepresented in psoriatic patients compared with controls and that both AA and GA genotypes are associated with increased psoriasis risk compared with GG genotype. To the best of our knowledge, our results showed for the first time an association between the A-1012G polymorphism and the overall risk of psoriasis occurrence. Only a previous study aimed to test the role of this polymorphism in a series of 206 psoriasis patients and 80 controls but failed to found this association (Halsall et al., 2005). The strength of our study based on a well-characterized series of psoriatic patients and a large number of controls, thus allowing us to perform a case–control study with a case–control ratio of 1:2.5.
Our well-characterized patients' series also enabled us to carry out a more detailed analysis suggesting that the risk associated with VDR genetic variants may also be linked to clinically important characteristics of psoriasis. A statistically significant difference in the distribution of A-1012G genotypes among patients stratified according to FH was observed. In particular, A-1012G risk genotypes were significantly more frequent in patients without FH of psoriasis compared with patients with FH, suggesting that A-1012G may exert its effect on psoriasis susceptibility in sporadic cases, probably interacting with concurrent environmental risk factors.
It is noteworthy that a significant association between the severity of psoriasis and BMI emerged in our series, in agreement with previous studies (Armstrong et al., 2012). We further investigate this association to verify whether the risk of severe psoriasis may be modulated by VDR polymorphisms in patients stratified according to clinical–pathological features. No association between the severity of psoriasis and VDR polymorphisms in overweight/obese patients was found, thus suggesting that obesity predispose to more severe psoriasis independent of VDR polymorphisms.
Inconsistent results have been thus far provided on associations between overall risk of psoriasis and VDR SNPs, including FokI, BsmI, ApaI, and TaqI (Kaya et al., 2002; Dayangac-Erden et al., 2007; Lee et al., 2012; Liu et al., 2013). A meta-analysis, including 1106 psoriasis cases and 1209 controls, failed to show a robust association with these loci, suggesting potential associations restricted to specific populations (Stefanic et al., 2013). Our results are in agreement with these findings. Moreover, here, we showed that FokI polymorphism may be associated with increased risk of severe psoriasis in male patients and that ApaI may be associated with increased risk of severe psoriasis in patients with arthropathic psoriasis. These findings may suggest a gender- and type-specific effect for VDR polymorphisms in the susceptibility of severe psoriasis. Thus, our results indicate that the severity of psoriasis in arthropathic patients could be modulated by genetic risk factors, thus improving our knowledge of this peculiar type of psoriasis.
Overall, a potential limitation of our study is that it is an exploratory genotype-based study and that it may be limited by the relatively small sample size. Further studies are needed to validate our results on large and diverse populations.
Importantly, in this study, we provided evidence of the functional relevance of the VDR A-1012G promoter variant. It has been so far hypothesized that polymorphisms within the promoter region may have a functional role on VDR expression and/or activity and therefore be more tightly associated with the development of diseases.
It was observed that the A allele of A-1012G polymorphism contains a binding site for the T-helper 2 (Th2) signaling factor GATA-3 (D'Alésio et al., 2005; Halsall et al., 2009). Since the inflammatory response in psoriasis is Th1-mediated, the Th1 to Th2 T-cell switching effected by GATA-3 suggested a protective role for the A allele (Halsall et al., 2009).
Several studies concerning vitamin D and VDR expression in animal and in vitro models showed immunomodulating effects, resulting in a switch from the Th1/Th17 response to the Th2/Treg profile. These immunomodulating effects may explain the reported epidemiological associations between vitamin D status and psoriasis (Boonstra et al., 2001; Guillot et al., 2010).
In this study, we performed a functional analysis of A-1012G by gene expression analysis in real-time quantitative-PCR. Compared with GG genotype, AA and GA genotypes were significantly associated with a lower VDR mRNA expression in PBMCs from psoriatic patients, and this association was dose dependent. These findings are compatible with the observed associations between AA and GA genotypes and risk of psoriasis since a decreased expression of VDR in psoriasis patients harboring the A allele may reduce the beneficial role of GATA-3 in suppressing Th1 effects. Moreover, less abundant VDR levels in PBMCs may affect the immunosuppressive activity of vitamin D in these cells.
Notably, previous functional studies were performed in vitro (Boonstra et al., 2001; Fang et al., 2005), whereas here we evaluated mRNA levels in PBMCs of psoriatic patients. These cells are known to express the VDR and are a good model for other target tissues of vitamin D because they have revealed both qualitative and quantitative abnormalities of the VDR (Zerwekh et al., 1993).
Conclusion
In conclusion, our data showed that A-1012G polymorphism in the promoter region of the VDR gene is associated with the risk of psoriasis occurrence. Moreover, AA and AG genotypes were significantly associated with a lower expression of VDR mRNA compared with GG genotype, suggesting that the genetic effect of A-1012G on psoriasis risk may be due to the impaired expression of VDR mRNA.
Variations in the VDR may result in altered vitamin D responsiveness in inflammatory conditions. In several immune-related diseases, VDR polymorphisms may influence therapeutic response to vitamin D analogues (Poon et al., 2012). Whether these findings could support a pharmacogenetic approach in immune-related diseases, such as psoriasis, asthma, and atopy, is still largely unclear and should be considered an intriguing topic for further research.
Overall, results from this study may be helpful in the assessment of genetic risk in psoriatic patients, as well as the prediction of VDR expression in patients based on risk genotypes and, eventually, given that VDR gene polymorphisms may explain the variable responsiveness to vitamin D analogues, may improve the clinical management of this disease.
Footnotes
Acknowledgment
This study was supported by “Sapienza” University of Rome (Ricerche Universitarie 2011).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.