
Abstract
The ∼80 amino acid A box DNA-binding domain of high mobility group box 1 (HMGB1) protein antagonizes proinflammatory responses during myocardial ischemia reperfusion (I/R) injury. The exact role of microRNA-21 (miR-21) is unknown, but its altered levels are evident in I/R injury. This study examined the roles of HMGB1 A-box and miR-21 in rat myocardial I/R injury model. Sixty Sprague-Dawley rats were randomly divided into six equal groups: (1) Sham; (2) I/R; (3) Ischemic postconditioning (IPost); (4) AntagomiR-21 post-treatment; (5) Recombinant HMGB1 A-box pretreatment; and (6) Recombinant HMGB1 A-box + antagomiR-21 post-treatment. Hemodynamic indexes, arrhythmia scores, ischemic area and infarct size, myocardial injury, and related parameters were studied. Expression of miR-21 was detected by real-time quantitative polymerase chain reaction (qRT-PCR) and terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) assay was used to quantify apoptosis. Left ventricular systolic pressure (LVSP), left ventricular end diastolic pressure (LVEDP), maximal rate of pressure rise (+dp/dtmax), and decline (−dp/dtmax) showed clear reduction upon treatment with recombinant HMGB1 A-box. Arrhythmia was relieved and infarct area decreased in the group pretreated with recombinant HMGB1 A-box, compared with other groups. Circulating lactate dehydrogenase (LDH) and malondialdehyde (MDA) levels increased in response to irreversible cellular injury, while creatine kinase MB isoenzymes (CK-MB) and superoxide dismutase (SOD) activities were reduced in the I/R group, which was reversed following recombinant HMGB1 A-box treatment. Interestingly, pretreatment with recombinant HMGB1 A-box showed the most dramatic reductions in miR-21 levels, compared with other groups. Significantly reduced apoptotic index (AI) was seen in recombinant HMGB1 A-box pretreatment group and recombinant HMGB1 A-box + antagomiR-21 post-treatment group, with the former showing a more dramatic lowering in AI than the latter. Bax, caspase-8, and CHOP showed reduced expression, and Bcl-2 and p-AKT levels were upregulated in recombinant HMGB1 A-box pretreatment group. Thus, recombinant HMGB1 A-box treatment protects against I/R injury and the mechanisms may involve inhibition of miR-21 expression.
Introduction
C
Reperfusion is essential for the survival of ischemia tissue, but evidence suggests that reperfusion itself causes irrecoverable additional tissue injury (Chen et al., 2008). Besides myocardial necrosis that is typically observed in I/R injury, ischemic insult promotes cardiomyocyte death through apoptosis (Gerczuk et al., 2012; Linkermann et al., 2013). The etiology of myocardial I/R injury is strongly linked to endogenous mediators of inflammatory responses, which stimulate the release of free radicals and oxidants, promoting myocardial damage (de Vries et al., 2013; van Golen et al., 2013). Further, inflammation also is induced in response to apoptosis following myocardial I/R injury (Miyazaki et al., 2011; Toldo et al., 2014). It is therefore reasonable to speculate that blockade of apoptosis may be beneficial to protect against myocardial I/R injury and the ideal therapeutic target to achieve this blockade is the subject of intense research.
Based on published studies, we hypothesized that a key correlation might exist between the initial myocardial cell damage and the activation of inflammatory mediators. High mobility group box 1 (HMGB1), is an abundant nuclear protein that is involved in nucleosome stability, DNA repair, and DNA replication. However, extracellular HMGB1 is detected in injured tissue and several studies have reported that the functions of extracellular HMGB1 are distinct from the nuclear functions of this protein. Cells undergoing death or necrosis, or during tissue damage, release of HMGB1 into extracellular space acts as a potent signal for initiating host defense responses or tissue regeneration, including strong proinflammatory responses (Tang et al., 2011; Nin et al., 2012; Yang et al., 2012).
Therapeutic blockade of extracellular HMGB1 functions may therefore be beneficial to control inflammation and limit ischemia-related tissue damage (Zhai et al., 2012). Such blockade appear to be possible by using HMGB1 A-box, a ∼80 amino acid long domain that has been shown to antagonize the extracellular cytokine activity of the 215 amino acid long full-length HMGB1 (Zhai et al., 2012). Treatment with recombinant HMGB1 A-box showed a remarkable protective effect against I/R injury and suppressed the activation of proinflammatory cascade (Andrassy et al., 2008).
microRNA (miRNAs) controls critical aspects of cardiovascular system, with a remarkable role in cardiovascular physiology and disease progression (Horie et al., 2010; Ono et al., 2011). For example, miR-30a/-30b overexpression reduces the levels of proapoptotic proteins like caspase-3 (Li et al., 2010). Similarly, myocardial-specific miR-1 is important in ischemic postconditioning (IPost) through regulating apoptosis-related genes (He et al., 2011). More recently, nicotine was shown to inhibit ERK1/2-SRF-miR-133 signaling to increase caspases-9 and -3, a novel mechanism to induce cardiomyocyte apoptosis (Wang et al., 2014). miR-21 is highly expressed in the cardiovascular system (Cheng and Zhang, 2010). miR-21 is preferentially expressed in adult cardiomyocytes and controls cardiac growth and gene activation stimulated by cardiac stress (Cheng et al., 2007; Tatsuguchi et al., 2007).
Previous studies using mouse myocardial I/R injury model showed that preinjection of miR-21 in vivo attenuated ischemia-induced cardiomyocyte damage by decreasing apoptosis, and specific antagomiR that inhibit miR-21 abolished this effect (Yin et al., 2008; Dong et al., 2009).
Based on current knowledge, we tested whether myocardial apoptosis could be modulated using recombinant HMGB1 A-box and antagomiR-21, and if better strategies could be identified to protect heart and cardiomyocytes against I/R injury. In this study, the effect of HMGB1 A-box and miR-21 on cardioprotection was tested in a well-known in vivo rat model of myocardial I/R injury.
Materials and Methods
Ethics statement
This study was approved by the Institutional Ethics Committee of the Fifth Affiliated Hospital of Sun Yat-Sen University. All procedures were in accordance with the Regulations on Animal Management Committee of the Fifth Affiliated Hospital of Sun Yat-Sen University. All effort was made to minimize the suffering of rats and to reduce the number of animals required in this study.
Animals and grouping
Male Sprague-Dawley rats (n = 60, specific pathogen-free [SPF] Grade), weighing 250–300 g, were obtained from the Experimental Animal Center of the Fifth Affiliated Hospital of Sun Yat-Sen University. Animals were housed at constant temperature (25°C) and humidity (60%) in a controlled environment with free access to water and food. Photoperiod was set at 12 h to mimic the normal physiological day-night regularity.
Sixty rats were randomly allocated in equal numbers to six groups (n = 10 per group). The left anterior descending (LAD) coronary artery was ligated to reproduce myocardial I/R model. The six groups were as follows: (1) Sham group, rats received sham-operations, where LAD was stringed without ligature; (2) I/R group, LAD was subjected to 40 min of MI followed by 120 min of reperfusion; (3) IPost group, similar to the I/R group, the LAD were subjected to 40 min of MI followed by 30 s of reperfusion for four cycles, and then reperfusion for 116 min; (4) AntagomiR-21 post-treatment group: 5 min before reperfusion (120 min) a dose of 2 mg/kg of antagomiR-21 was administered after undergoing right atrial catheterization; (5) Recombinant HMGB1 A-box post-treatment group, LAD was infused with a dose of 2 mg/kg of recombinant HMGB1 A-box (Department of Experimental Hematology, Institute of Radiation Medical Science, Academy of Military Medical Sciences, Beijing, China) 5 min before reperfusion (120 min) after undergoing right atrial catheterization; and (6) Recombinant HMGB1 A-box + antagomiR-21 post-treatment group, similar to the recombinant HMGB1 A-box pretreatment group, but LAD was also infused with a dose of 40 mg/kg antagomiR-21 (Guangzhou RiboBio Co., Ltd.) 5 min before reperfusion after undergoing right atrial catheterization. The same volume of normal saline was administrated under the right atrial catheterization in I/R and IPost groups lasting for 60 min as controls before refusion. All drugs were injected with gradually increased dose.
Establishment of rat I/R injury model
Rats were injected with 3% sodium pentobarbital (30 mg/kg) after 12 h fasting. Heparin (1 mg/kg) was employed as an anticoagulant. After separation of carotid artery, guiding catheters (6F) were inserted into left ventricle through right carotid artery. A four-channel physiological recorder was used to monitor left ventricular pressure (LVP). Further, electrocardiogram (EKG) was recorded from four silver wire leads and rat limbs. The EKG recordings were high-pass filtered to exclude DC shifts due to animal movement. The trachea was incised transversely between the third and fourth rings, and a 24-G venous indwelling needle (0.7 × 1.9 mm) was used for tracheal intubation. Next, the endotracheal tube was connected to a TKR-200C small animal ventilator (Teli Anaesthesia & Respiration Equipment Co., Ltd.) and ventilated with 95% O2 and 5% CO2 gas mixture.
The effective ventilatory volume was adjusted to maintain 1 mL/g/min. The breathing rate was set at 80 breaths per minute, and the respiratory rate was set to 1:1.5 (Normal pressure: 5–15 cm H2O). Preoperative hair removal was performed, followed by further intravenous administration via femoral vein. Briefly, heart was exposed by left thoracotomy under sterile conditions. Chest was opened with blunt and sharp dissection, and heart was exposed via pulling the pericardium with a retractor. The left atrial appendage was lifted with a pair of hemostatic forceps to locate the anterior descending branch of coronary artery. Establishment of regional MI was done by transient occlusion of LAD coronary artery. The LAD coronary artery was suture ligated (Ethilon; Ethicon) 1.5–2 mm below the junction of pulmonary conus and aorta, with a section of silicone tube (diameter 0.15–0.18 mm) placed over the left coronary artery.
LAD ligation resulted in color change (pale to cyanotic) on the left ventricular wall, and the ventricular wall motion was weakened. ECG showed significant ST elevation (over 0.25 mV), indicating successful ligation. I/R injury were induced by LAD coronary artery occlusion for 40 min followed by 120 min reperfusion of LAD. For consistency, the same person performed a specific step in the operation for all the animals. After 30 min of ischemia, tube and suture were removed for reperfusion. After completion of reperfusion period, cardiac impulse of rats was recorded, and the chest wall was closed layer by layer. In the sham-operated group, LAD coronary artery was sutured passing through the vessels, but without LAD coronary artery occlusion.
Clinical indexes observation
Hemodynamic indexes monitoring
Catheterization was conducted from the right common carotid artery to the left ventricle before chest opening. Heart rate (HR), left ventricular systolic pressure (LVSP), and left ventricular end diastolic pressure (LVEDP) were recorded using RM6240 multichannel physiologic recording and processing system (Chengdu Instrument Factory) connected to a Baroreceptor, with recordings collected at 15 min before ischemia, 30 min after ischemia, and 2 h after reperfusion. LVP curves were recorded onto a computer equipped with a data acquisition program (SonoView 3.1.4; Sonometrics) and analyzed to estimate the left ventricular dp/dt curve and maximal rate of pressure rise (+dp/dtmax) and decline (−dp/dtmax) over time.
Score of arrhythmia
Cumulative duration of ventricular premature beat (VPB), ventricular tachycardia (VT), and ventricular fibrillation (VF) were recorded during I/R. The severity of arrhythmia was assessed by the following scale (Tsuchida et al., 1994): (1) 0 point, no ventricular arrhythmias or only VPB occurred (<5 times/min); (2) 1 point, only VPB occurred (≥5 times/min); (3) 2 points, only burst of VT (<60 s); (4) 3 points, VT (≥60 s) or multiple VT with accumulative time ≤60 s; (5) 4 points, multiple VT with accumulative time ≥60 s; (6) 5 points, VF occurred but spontaneously recovered; (7) 6 points, unrecoverable VF or animal died during observation period.
Measurement of ischemic regions and extent of myocardial infarction
Half the rats in each group were administrated supplemental local anesthesia, and the LAD branch of each rat was blocked again at the end of the experiment. Next, 3–4 mL of 2% Evans blue dye (BMassay) was injected into the left cardiac catheterization. The chest cavity was quickly opened and the heart was excised. Left ventricle tissues were further isolated, snap frozen in liquid nitrogen, and stored at −20°C for 25 min. Heart tissues were isolated and serially sliced (five pieces, 2–2.5 mm thick each) using a heart slicer and incubated in 1% TTC (PH7.4; BMassay) (in phosphate-buffered saline) pre-equilibriated at 37°C for 10–15 min. Observations using naked eyes were as follows: the myocardial infarction area (IA) was white in color, the area of myocardial infarction was white, and the healthy myocardium was red in color. High-resolution pictures (>10 million pixels) were taken with a professional-grade digital camera. The MiVnt image analysis software system was used for image processing of the meso-observation images for the determination of the left ventricle area (LVA), IA, areas at risk (AAR) of infarction in the myocardial infarct and border area, and the myocardial infarction area, to calculate AAR/LVA and IA/AAR.
Markers of myocardial injury and related indicators detection
Blood (2 mL) from right atrial appendage was collected 15 min before ischemia, 30 min after ischemia, and 2 h after reperfusion. The quantitative determination of serum creatine kinase MB isoenzymes (CK-MB) and lactate dehydrogenase (LDH) was performed by fluorescent probes using Automatic Biochemistry Analyser (Beckman Coulter, Inc.). Total plasma superoxide dismutase (T-SOD) activity was determined by Xanthine/xanthine oxidase method using a TSOD Assay Kit A001. The concentration of malondialdehyde (MDA) was measured by the thiobarbituric acid (TAB) method using a MDA Assay Kit A003. The kits were purchased from Nanjing Jiancheng Bio-engineering Institute (Nanjing, China).
Real-time quantitative polymerase chain reaction
After I/R, the remaining six rats in each group were used to study the expression levels of miR-21. The mirVana qRT-PCR miRNA detection kit was used to detect miR-21 expression, and all steps were performed according to manufacturer's instructions (Ambion). Normal myocardial tissues from the Sham group and infarcted myocardium from the experimental groups were removed from liquid nitrogen and thinly sliced (0.5–1.0 cm). The sliced tissues were ground into powder in liquid nitrogen. Total RNA was isolated using TRIzol reagent (Invitrogen Company), according to the instructions contained in the miRNA isolation kit (mirVana; Ambion). The concentration and purity of RNA were measured by optical density (OD, at λ = 260/280 nm) using an ultraviolet spectrophotometer (UV-2700; SHIMADZU). RNA samples of high quality with 260/280 ratios (1.8–2.1) were used in subsequent steps. RNA reverse transcription: The reverse transcription reactions (20 μL final volume) contained 40 ng of RNA template, 1 μL of miScript Reverse Transcriptase Mix, 4 μL of 5* miScript RT Buffer, and RNase free water. Further, the reaction mixture was incubated for 60 min at 37°C, followed by reverse transcriptase inactivation at 95°C for 5 min. Samples were stored at −20°C for qRT-PCR.
First strand cDNA was amplified using specific miR-primers (Applied Biosystems). miR-21 was quantified using miScriptSYBR Green PCR Kit, which contained hs-miR21 (miR-21 specific primer; Takara Company). Light Cycler 480® system was used for PCR amplification and detection. U6 (Takara Company) was used as an internal reference. The primers used for amplification of miR-21 and U6 were designed with Primer Premier 5.0 software (Premier Biosoft International) and the sequences were as follows: miR-21: RT: 5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATAC GACTCAACA -3′; Forward primer: 5′-GTGCAGGGTCCGAGGT-3′; Reverse primer: 5′-GCCGCTAGCTTATCAGACTGATGT-3′; U6: RT: 5′-AACGCTTCACGAATTTGCGT-3′; Forward primer: 5′-CTCGCTTCGGCAGCACA-3′; Reverse primer: 5′-AACGCTTCACGAATTTGCGT-3′. PCR were carried out as follows: 95°C for 15 min, 94°C for 15 s, 55°C for 30 s, and 70°C for 30 s for 50 cycles.
The threshold value was set at the minimum for each amplification curve, with the fluorescence signal significantly rises above the background signal, and threshold cycle (Ct) was calculated. Relative expression of miR-21 was calculated with 2−ΔΔCt method as follows: ΔCT = (Target gene CT − Reference CT); ΔΔCT = (Infarcted myocardium ΔCT − Normal myocardial tissues ΔCT).
Western blotting
Western blotting was used to measure the levels of several markers of the pathways investigated. Total protein from myocardial tissue was extracted using lysis buffer (Pik-day Biotechnology Research Institute, Beijing, China). Tissue samples were sonicated (Fisher 550 sonicator) for 1 min at 4°C and centrifuged, and the supernatant was stored at −70°C until assay. Protein concentrations were determined using Bradford assay. Protein separation was performed by SDS-PAGE (Pik-day Biotechnology Research Institute). The separated proteins were transferred onto nitrocellulose membranes. After blocking with 5% skimmed milk, the membranes were incubated at 37°C for 1 h with rabbit polyclonal primary antibodies p-AKT (1:1000), Bcl-2 (1:1000), Bax (1:2000), Caspase-8 (1:5000), CHOP (1: 1000), and β-actin (1:1000) purchased from Abcam.
Following washing, the membranes were incubated at 37°C for 30 min with a secondary horseradish peroxidase-conjugated goat anti-rabbit IgG antibody (1:1000; Beyotime Institute of Biotechnology, Haimen, China). Protein bands of interest were detected with ECL chemiluminescence reagent (Amersham Pharmacia Biotech), and IPP 6.0 image analysis software was used to analyze the gray value of each band area. β-actin was the loading control.
Myocardial apoptosis by TUNEL assay and myocardial ultra-structure observation
The left ventricle tissue was fixed in 4% formaldehyde overnight at room temperature. After dehydration with gradient ethanol, fixed tissue was embedded in paraffin and serially sliced, and TUNEL assay was performed using apoptosis detection kit (Wuhan Boster Biological Technology Co., Ltd.). A TUNEL-negative control was part of the kit components. Red-colored particles appearing in the cell nucleus with clear nuclear labeling were defined as TUNEL-positive cells. The number of TUNEL-positive cardiomyocytes, indicating apoptosis, was counted and expressed as mean number per/100 cells/microscopic field. Four randomly selected fields of each sample were examined using a Nikon Eclipse E400 microscope (10 × 100; Nikon) in each group. Photographs were taken and archived. The apoptotic index (AI) was counted using Leica Qwin V3 software, and average values were used for final analysis. Positive-labeled cells were expressed as percentage of total cells counted. AI = ODaverage × TUNEL-positive cells/total number of myocytes ×100.
Some specimens were fixed in 3% glutaraldehyde (pH 7.4) and stored at 4°C for the purpose of electron microscopy. These tissues were washed with phosphate-buffered saline (PBS, pH 7.4), followed by dehydration with gradient alcohol solution. Epoxy resin was used to infiltrate the samples. The samples exhibited correct localization upon examination using a light microscopic, following flat embedding in polymerized resin. Collected specimens were sliced, stained with uranyl acetate and lead citrate, and observed under H-600 transmission electron microscope (Hitachi) for myocardial ultra-structure.
Statistical analysis
SPSS 18.0 software was used for statistical analysis. Measurement data were represented as mean ± standard deviation (SD). LSD- t test was applied for paired comparison of continuous variables. Comparison of measurement data among groups was performed by one-way analysis of variance (ANOVA). The clinical indexes and relative expression of miR-21 was expressed as median (interquartile range) and analyzed by nonparametric Wilcaxon's test. Differences were considered significant at p < 0.05.
Results
Hemodynamic indexes
After 120 min reperfusion, no differences were obvious in HR among all the experimental groups (all p > 0.05). As shown in Figure 1, compared with the Sham group, LVSP, LVEDP, +dp/dtmax, and −dp/dtmax were decreased in the other groups that underwent ischemia, with statistically significant differences (all p < 0.05) except LVSP, indicating left ventricular systolic and diastolic dysfunction. The above indexes also showed clearly decreasing trend in antagomiR-21 post-treatment group, recombinant HMGB1 A-box pretreatment group and recombinant HMGB1 A-box + antagomiR-21 post-treatment group, compared with the I/R group, with the penultimate group showing the most reduced value (all p < 0.05). However, no relationship was evident when compared to IPost group (all p > 0.05). Detailed data are shown in Table 1.
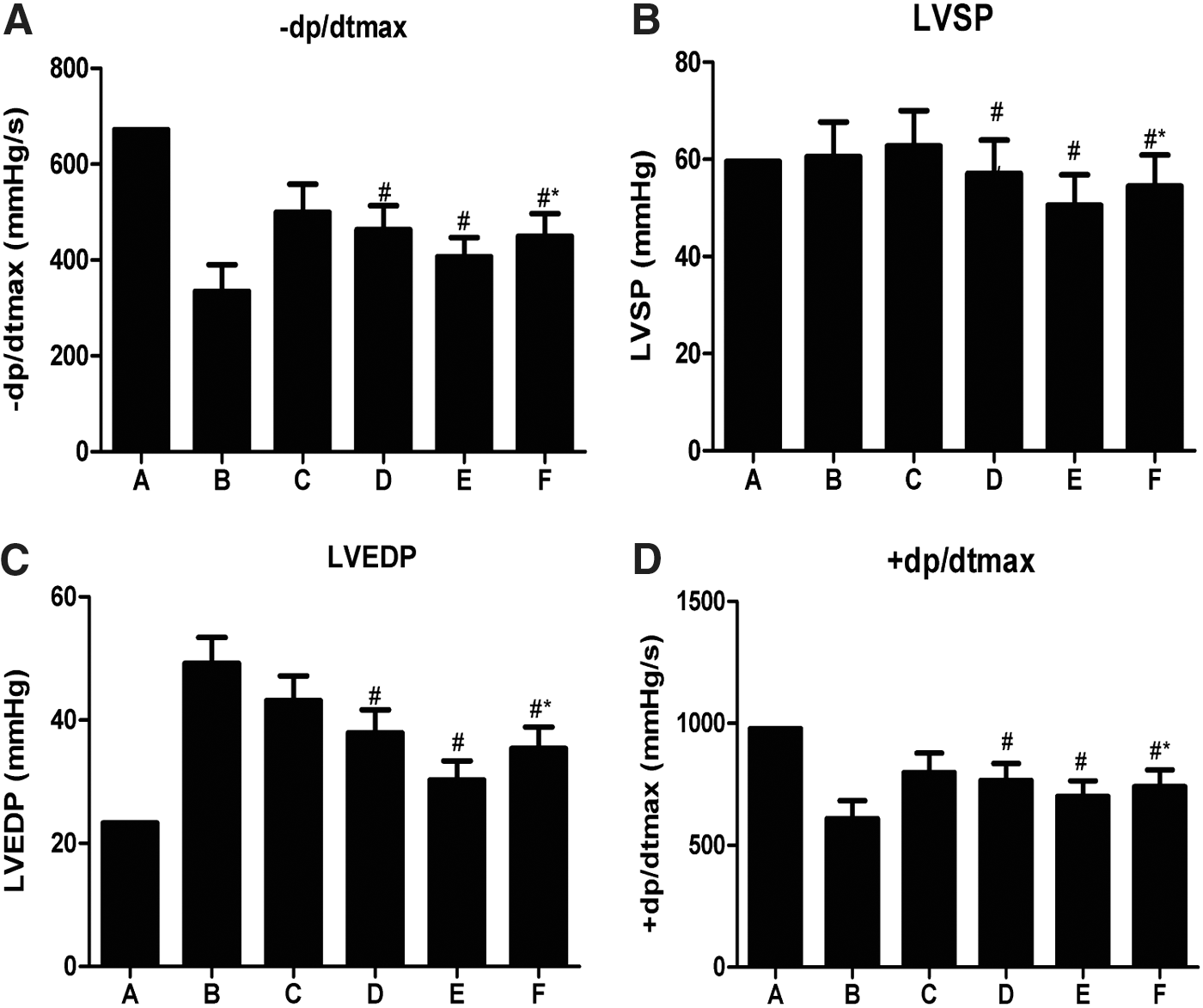
Hemodynamic indexes (
Compared with the Sham group, p < 0.05.
Compared with the I/R group, p < 0.05.
Compared with the Recombinant HMGB1 A-box pretreatment group.
A: Sham group; B: Ischemia reperfusion (I/R) group; C: IPost group; D: antagomiR-21 post-treatment group; E: Recombinant HMGB1 A-box pretreatment group; F: Recombinant HMGB1 A-box + antagomiR-21 post-treatment group. HR, heart rate; LVSP, left ventricular systolic pressure; LVEDP, left ventricular enddiastolic pressure; +dp/dtmax, maximal rate of pressure rise; −dp/dtmax, maximal rate of pressure decline; HMGB1, high mobility group box 1.
Arrhythmia scoring
Ventricular arrhythmia scoring is shown in Table 2. There were occasional VPB detected in the Sham group, but no other signs of cardiac arrhythmias were observed. Frequent VPB, VT, VF, and second-degree or third-degree atrioventricular block were observed immediately 1 min after coronary reperfusion in the I/R group (two rats died of VF), which was significantly increased compared with the Sham group (all p < 0.05). There were six cases of arrhythmia, mainly VPB and VT, which was significantly reduced when compared with the I/R group (p < 0.001). Arrhythmias showed no significant relief in the antagomiR-21 post-treatment group. The recombinant HMGB1 A-box pretreatment group showed greater relief of recombinant HMGB1 A-box + antagomiR-21 post-treatment group (p < 0.05). Therefore, rats treated with recombinant HMGB1 A-box experienced dramatically reduced symptoms of arrhythmia (p < 0.001).
Compared with the I/R group, p < 0.05.
Compared with the Recombinant HMGB1 A-box pretreatment group.
A: Sham group; B: Ischemia reperfusion (I/R) group; C: IPost group; D: antagomiR-21 post-treatment group; E: Recombinant HMGB1 A-box pretreatment group; F: Recombinant HMGB1 A-box + antagomiR-21 post-treatment group. VA, ventricular arrhythmias; CK-MB, creatine kinase MB isoenzymes; LDH, lactate dehydrogenase; MDA, malondialdehyde; SOD, superoxide dismutase. Two rats died of ventricular fibrillation in group B, data collected in group B were the valid data from the eight surviving rats. t-Test was applied to conduct the statistical test used to compare the categorical results obtained from the arrhythmia score.
Measurement of ischemic regions and extent of MI
As seen in Figure 2, MI was not detected in Sham group, and the extent of MI (AAR/LAV) caused by coronary artery ligation was 67.23 ± 6.98 and 50.30 ± 7.78 in the I/R group and IPost group, respectively. The differences in the severity of MI between the I/R and IPost groups were statistically significant (p < 0.05). Compared with the I/R group, infarct areas decreased by 25%, 33%, and 45% in the IPost group, antagomiR-21 post-treatment group, and recombinant HMGB1 A-box + antagomiR-21 post-treatment group, respectively, and decreased the most by ∼54% in recombinant HMGB1 A-box pretreatment group (all p < 0.05).
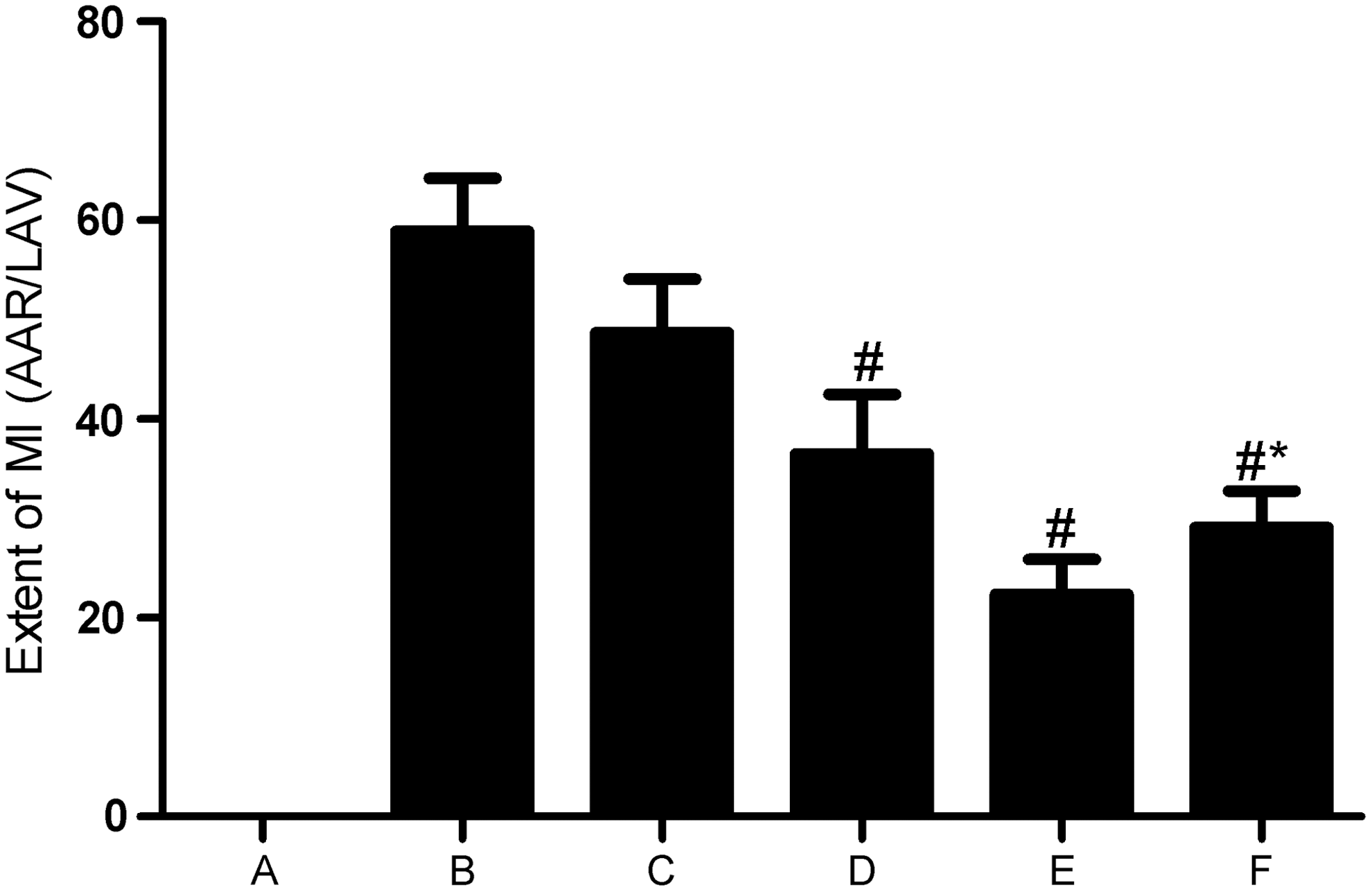
Measurement of ischemic regions and extent of MI among different groups.
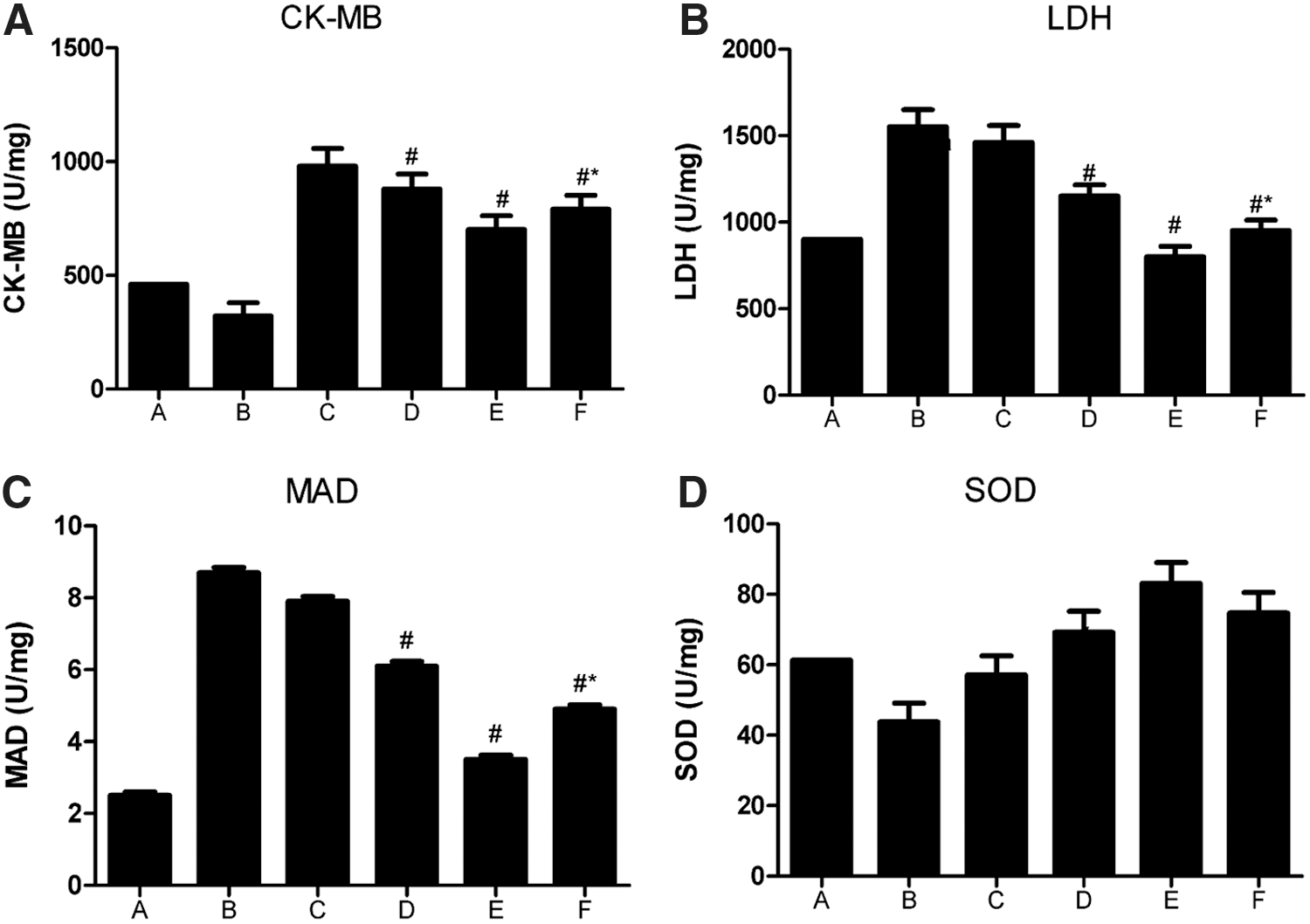
Activity of serum CK-MB
Serum CK-MB activity showed a remarkable decrease in the IPost group, the antagomiR-21 post-treatment group, and recombinant HMGB1 A-box + antagomiR-21 post-treatment group (42%, 46%, and 52%, respectively) compared with the I/R group (all p < 0.05). The decrease was 59% in the recombinant HMGB1 A-box pretreatment group compared with the I/R group (p < 0.05, Fig. 3A).
Detailed information of serum
Concentration of LDH in serum
Compared with the Sham group, LDH concentration in the serum was elevated in I/R and IPost group and this was readily reversed in the antagomiR-21 post-treatment group, recombinant HMGB1 A-box + antagomiR-21 post-treatment group, and recombinant HMGB1 A-box pretreatment group, with the last mentioned group showing significant decreases compared with the first two groups (all p < 0.05, Fig. 3B), suggesting that the recombinant HMGB1 A-box displays powerful protective role in myocardial I/R.
Serum MAD and SOD levels
As shown in Figure 3C and D, compared with the Sham group, serum level of MAD was elevated in the I/R group, while serum SOD level decreased (p < 0.05). In comparison to the I/R group, the converse was true in the other five groups (all p < 0.05). There was a clear increasing trend in serum SOD levels in the recombinant HMGB1 A-box pretreatment group compared to IPost group.
miR-21 expression by qRT-PCR
The miR-21 levels measured by qRT-PCR is presented in Figure 4A. Compared with the sham group, miR-21 mRNA significantly increased in the I/R and IPost group, suggesting increased miR-21 expression after I/R treatment (all p < 0.05). No significant difference in the level of miR-21 was found between the I/R group and IPost group (all p > 0.05). Compared with the IPost group, miR-21 expression level showed significantly decreasing trend in the three intervention groups (all p < 0.05) except the antagomiR-21 post-treatment group, and recombinant HMGB1 A-box pretreatment group showed the highest level of reduction compared with recombinant HMGB1 A-box + antagomiR-21 post-treatment group (both p < 0.05). A pictorial chart of HMG box protein and microRNA-21 interaction was shown in Supplementary Figure S1 (Supplementary Data are available online at
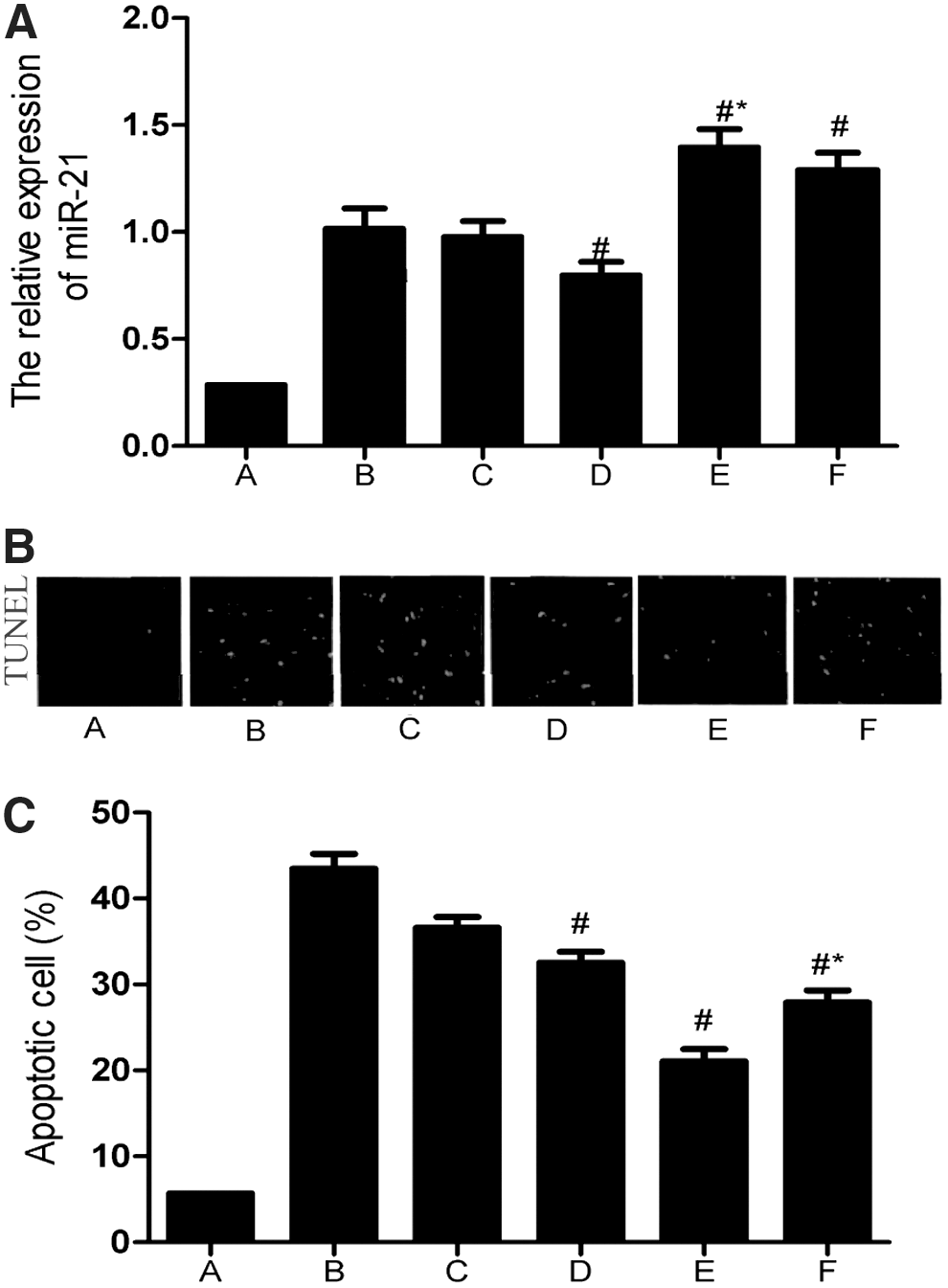
Protective effect of miR-21 on I/R by reducing cardiac cell apoptosis
The results of myocardial apoptosis in I/R model is shown in Figure 4B. The effect of miR-21 on cardiomyocyte apoptosis in I/R rats is shown in Figure 4C. TUNEL-positive cells were mainly located at the junction of the infarct zone and viable myocardium, and only a few scattered apoptotic cells were found within the infarction area. A relatively lower AI was seen in the Sham group, and TUNEL-positive cells in I/R group were significantly increased compared with the Sham group (36.83% ± 1.42% vs. 43.49% ± 1.69%). In comparison with the I/R group, AI was also reduced in IPost group (36.62% ± 1.22%) and the other three intervention groups. AI was further reduced in the recombinant HMGB1 A-box + antagomiR-21 post-treatment group and recombinant HMGB1 A-box pretreatment group (27.91% ± 1.39% vs. 21.05% ± 1.41%), with the latter showing significantly lower AI than the other two groups (all p < 0.05).
Expressions of Bcl-2, Bax, Caspase-8, and CHOP in the myocardial tissue
Apoptosis-related proteins Bcl-2, Bax, Caspase-8, and CHOP in the myocardial tissue were detected on western blots (Fig. 5). When compared with the sham group, Bcl-2, an antiapoptotic factor, decreased in the I/R and IPost groups, while Bax, Caspase-8, and CHOP, which are proapoptotic factors, increased in the I/R and IPost groups. Although Bcl-2/Bax ratio decreased, the difference between the two groups was not statistically significant (all p > 0.05).
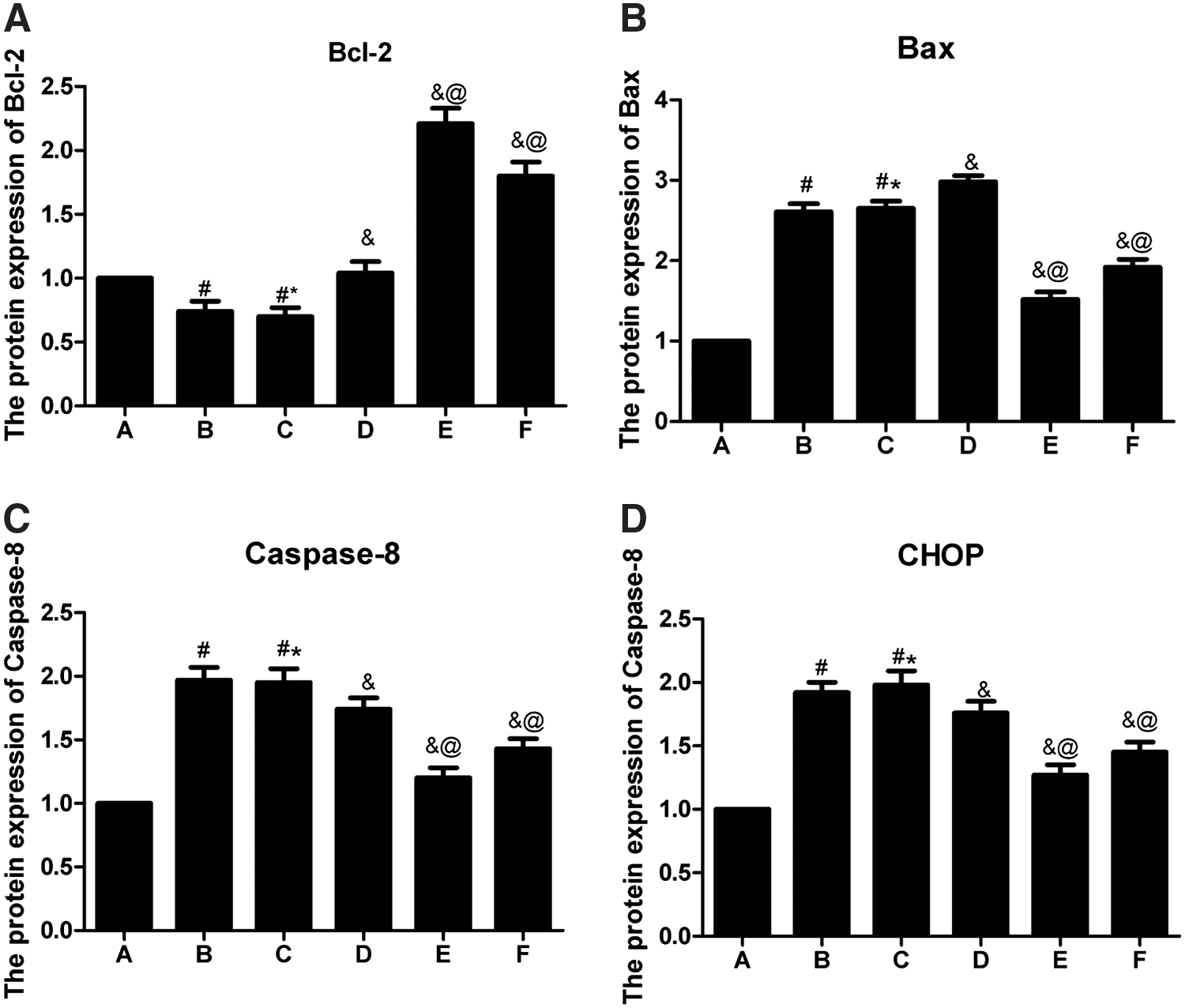
Western blotting detected the protein expression of
However, compared with IPost group, Bcl-2 expression was significantly elevated, while Bax, Caspase-8, and CHOP expressions were reduced, in the three intervention groups, with increased Bcl-2/Bax ratio (all p < 0.05). Thus, Bax, Caspase-8, and CHOP showed significantly decreased expression in recombinant HMGB1 A-box pretreatment group and recombinant HMGB1 A-box + antagomiR-21 post-treatment group, compared with antagomiR-21 post-treatment group. Further, Bax, Caspase-8, and CHOP expression levels were relatively lower in the recombinant HMGB1 A-box pretreatment group (all p < 0.05). On the contrary, Bcl-2 expression was higher in the recombinant HMGB1 A-box pretreatment group and recombinant HMGB1 A-box + antagomiR-21 post-treatment group, compared with AntagomiR-21 post-treatment group. Bcl-2 expression was higher in recombinant HMGB1 A-box pretreatment group (all p < 0.05).
Assessment of Ras/Akt signaling pathway
As shown in Figure 6, compared with the Sham group, the level of p-AKT activation in ischemic regions of I/R and IPost group were significantly lower (p < 0.05), but p-AKT levels in the three intervention groups were highly upregulated relative to I/R (p < 0.05). The level of p-AKT was sharply increased in recombinant HMGB1 A-box pretreatment group compared with the other two intervention groups (all p < 0.05).
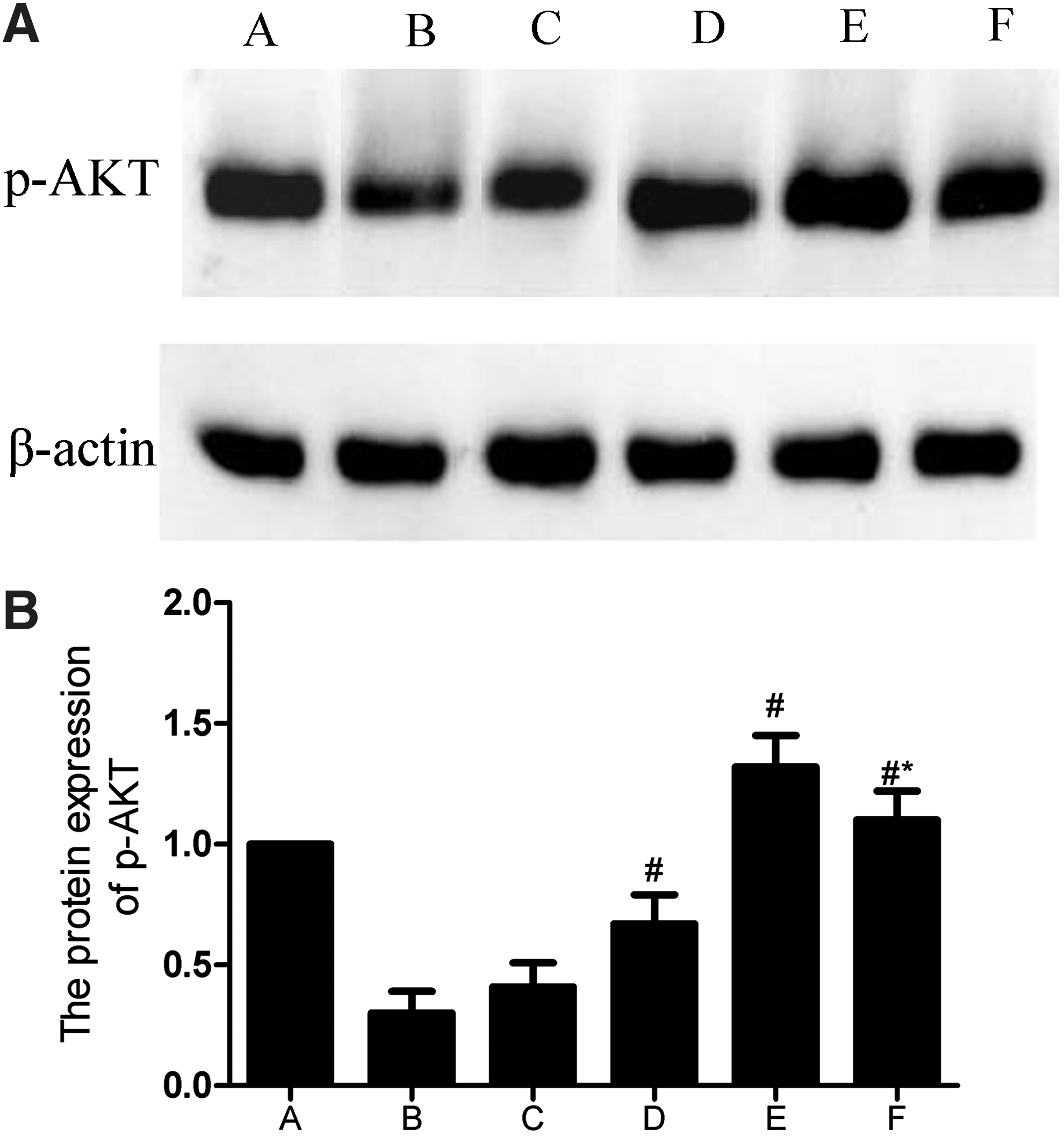
Western blotting detected the protein expression of p-AKT among different groups (
Discussion
In this study, recombinant HMGB1 A-box treatment during reperfusion after MI attenuated the progression of myocardial I/R injury. More importantly, HMGB1 A-box treatment dramatically increased myocyte apoptosis when combined with antagomiR-21, suggesting that antagomiR-21 effectively regulates myocardial protection role through control of myocyte apoptosis.
Our results show reductions in LVSP, +dp/dtmax, −dp/dtmax, and LVEDP, which are consistent with the aberrant pathophysiological changes during myocardial stress in the I/R model, suggesting significant left ventricular systolic and diastolic dysfunction. In HMGB1 A-box treatment group, however, the progression of ventricular chamber dilatation and ventricular dysfunction was prevented, thus administration of HMGB1 A-box indeed improves left ventricular systolic and diastolic function following MI using conscious rats.
The rat I/R injury model reflects the dynamic environment and progressive stages of damage of the myocardium, beginning with ventricular arrhythmias (Quindry et al., 2010). Frequent VPB, VT, VF, and second-degree or third-degree atrioventricular block was observed immediately after coronary reperfusion in the I/R group. A potential explanation might be that I/R is associated with production of excessive reactive oxygen species (ROS), which cause structural damage to the biological membranes, and small changes in membrane fluidity and permeability may result in altered function, promoting the cardiac arrhythmia phenotype (Catala, 2012; Neckar et al., 2012). Importantly, recombinant HMGB1 A-box treatment resulted in significantly reduced symptoms of arrhythmia. The results suggest that HMGB1 A-box treatment may decrease membrane fluidity and permeability, either by preventing oxidation or through other mechanisms, leading to reduced leakage of ions and enzymes, thus preventing arrhythmia (Hu et al., 2013).
Measurement of infarct size is one of the gold standards to assess the severity of myocardial I/R injury (Fernandez-Jimenez et al., 2012). Indeed, MI were not evident in the Sham group, but the severity of MI (AAR/LAV) caused by coronary artery ligation showed no differences among the groups, suggesting a positive occlusion effect of LAD ligation, where the LAD ligation sites were basically the same. Additionally, compared with the I/R group, infarct area decreased in the IPost group and HMGB1 A-box groups and the area was the most dramatically reduced in rats that received recombinant HMGB1 A-box treatment, compared with the other two treatment groups. Thus, the recombinant HMGB1 A-box treatment regimen used in this study displayed excellent outcomes in reducing MI, consistent with previous studies (de Souza et al., 2012; Hu et al., 2012).
Cardiac-specific biomarkers that accumulate at high concentrations in damaged myocardium but show little or no expression in normal cardiac tissue or other tissues are ideal for assessing tissue-specific changes under experimental conditions (Recchioni et al., 2013). In this study, HMGB1 is expressed in adult cardiomyocytes. On the other hand, LDH (a variety of tissue damages increases serum LDH levels) and MAD (a ROS and an index for oxidative stress) are released into circulation in response to irreversible cellular injury and necrosis. CK-MB (MI-related enzyme) and SOD (antiapoptotic gene) were suppressed in the I/R group, which showed strong correlation with the severity of MI and infarct area in the different experimental groups. These results indicated that recombinant HMGB1 A-box treatment might regulate pathways that inhibit the production of ROS induced by myocardial I/R and mechanisms that elevate antiapoptotic gene expression (Du et al., 2014).
TUNEL assay demonstrated that cardiomyocyte apoptosis was mainly located at the junction of the infarct zone and viable myocardium, with a few scattered apoptotic nuclei found within the infarct area. This is consistent with previous observations that apoptotic cardiomyocytes are generally detected in MI, experimental MI after coronary ligation, or myocardial hibernation (Kristen et al., 2013). TUNEL-positive cells were significantly reduced by recombinant HMGB1 A-box pretreatment and recombinant HMGB1 A-box + antagomiR-21 post-treatment, with the former showing lower TUNEL-positive cells compared with the latter. This result indicated that HMGB1 A-box treatment also was highly effective in inhibiting cardiomyocytes apoptosis. I/R stimulates elevated myocardial expression of HMGB1 in vivo, where it is linked with myocyte apoptosis and activation of proinflammatory immune response (Xu et al., 2011).
The full-length HMGB1 protein mediates host defense response by activating toll-like receptors (TLR), TLR4 and TLR9, and the receptor for advanced glycation end products (RAGE), which are essential in the myocardial metabolism related to I/R injury in an external reperfusion Langendorff model (Ibrahim et al., 2013; Zhu et al., 2013). It is possible that recombinant HMGB1 A-box treatment could antagonize HMGB1-RAGE interaction, conferring protection against I/R injury and suppress the activation of proinflammatory cascades (Andrassy et al., 2008). A potential alternate explanation could be that HMGB1 acts as an early mediator of inflammation during I/R injury and promotes release of tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6).
By contrast, HMGB1 A-box domain attenuates myocardial I/R injury by suppressing the release of TNF-α and IL-6, thus halting the inflammatory cascade that is central to myocardial I/R injury (Du et al., 2014). Recent studies show that miR-21 has a protective role in MI by modulating ventricular remodeling and myocardial fibrosis, while miR-30b increases myocardial I/R injury in rats (Qin et al., 2012; Toldo et al., 2014).
Thus, overexpression of miR-21 may attenuate I/R injury via targeting specific genes to exert an antiapoptotic effect. Previous studies also showed a remarkable increase in miR-21 expression during I/R injury, and these led to the proposal that miR-12 influences cell proliferation and apoptosis in cardiac myocytes through targeting programmed cell death four (Cheng et al., 2009). After IPost, miR-21 was significantly upregulated in rat myocardium, conversely, the protective effect of miR-21 was suppressed by antagomiR-21 treatment, suggesting that miR-21 is involved in IPost-mediated cardiac protection (Cheng et al., 2010). In this study, recombinant HMGB1 A-box pretreatment alone showed significantly better outcomes in I/R injury by reducing cardiac cell apoptosis, compared with the combination of recombinant HMGB1 A-box + antagomiR-21.
We further examined Bcl-2, Bax, Caspase-8, and CHOP in the current I/R model. Bcl-2 is the principal antiapoptotic protein, and suppresses apoptosis through its effects on mitochondrial membrane integrity and apoptotic signaling pathways (Parsons and Green, 2010). Antiapoptotic factors Bax, Caspase-8, and CHOP, on the other hand, suppress the release of apoptosis-inducing factors (Serasinghe et al., 2015). In this study, Bax, caspase-8, and CHOP expression was suppressed, and Bcl-2 expression was upregulated. The upregulation of Bcl-2 and downregulation of Bax increases Bcl-2/Bax ratio, which is further associated with the greater activation of apoptotic pathways (Xia et al., 2014).
Activation of Akt is a prosurvival mechanism and leads to suppression of the phosphorylation of proapoptotic proteins, while activating mediators involved in angiogenesis, growth, proliferation, and transcription (Guertin et al., 2006; Bozulic and Hemmings, 2009). Akt activation induced by recombinant HMGB1 A-box and miR-21 could also be critical for the antiapoptotic response and for the suppression of proapoptotic factors expression, consistent with our results. Ras/Akt activation protects myocardial cells from apoptosis induced by ischemia by targeting downstream molecules like Bcl-2, Bax, Caspase-8, and CHOP, indicating the importance of Ras/Akt signaling pathway in the I/R model (van der Weyden and Adams, 2007; Kim and Kang, 2010; Kristen et al., 2013).
In this study, recombinant HMGB1 A-box treatment reduced myocardial I/R injury, which may be associated with the inhibition of HMGB1 expression. HMGB1 A-box shows a synergistic relationship with miR-21 with regard to their antiapoptotic effects relevant to myocardial I/R injury. Therefore, the underlying molecular mechanisms involving HMGB1 A box and miR-21 network should be further investigated in the early phases of rat MI injury model to uncover potential clinical applications. However, the limitation of this study is that hemodynamic parameters are measured in animals, thus potential variations in operating procedures or deviations due to adverse effects could have strongly influenced the accuracy and reliability of the measured parameters. Future investigations are therefore warranted to identify the precise mechanisms and confirm our current findings.
Footnotes
Acknowledgments
We would like to acknowledge our instructors for their valuable advice. We also thank the reviewers for their precious comments on this article.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.