
Abstract
This study aims to investigate whether a relationship exists between the C3435T polymorphism of ABCB1 gene and poststroke depression (PSD). A total of 82 PSD patients and 115 nondepression patient (NPSD) controls were included in this study. All patients were evaluated using the Hamilton Rating Scale for Depression to determine the severity of depression and complete the packet. PSD patients were diagnosed in accordance with the DSM-V criteria. The C3435T polymorphism of ABCB1 was genotyped through fluorescence in situ hybridization and chromosome karyotype analysis system. The PSD (n = 82) and NPSD groups (n = 115) had a total prevalence rate of 41.6%. The prevalence of PSD in men was 58.5%, whereas that in women was 41.5%, and no statistically significant difference existed between the two groups (χ 2 = 1.009; p = 0.315). The CC, CT, and TT frequencies of the PSD group were 26.8%, 47.6%, and 25.6%, respectively, whereas those of the NPSD group were 42.6%, 45.2%, and 12.2%, respectively. Based on the CC genotype, the relative risk of homozygous mutant TT was 3.341 (χ 2 = 7.869; p = 0.005; OR = 3.341), and the T allele frequency in the PSD group was 49.4% higher than that in the NPSD group. The locus gene frequency was 34.8%, and the relative risk of allele T relative to allele C was 1.830 (χ 2 = 8.381; p = 0.004; OR = 1.830). A certain correlation exists between the C3435T gene polymorphism and PSD in the Han population in South Anhui Province, China, and further studies are needed to confirm our findings.
Introduction
Stroke is a common neurological disease with high rates of morbidity and mortality. The disease has caused a serious increase in global mortality and has now become the leading cause of death, especially in underdeveloped countries (Loubinoux et al., 2012; Ozturk, 2014; Bai et al., 2017). Stroke survivors are often accompanied with varying degrees of physical and psychological disability. Psychosocial aspects are more likely to be poststroke depression (PSD) (Al-Karawi et al., 2016) with clinical symptoms such as apathy, fatigue, loss of worth, and sleep disorders. These symptoms not only prolong the hospitalization time of stroke patients but also increase the economic burden and have a serious negative impact on the recovery of neural functions (Loubinoux et al., 2012; Visser et al., 2014).
Until now, the pathogenesis of PSD is still under study, and current related research suggests that multiple factors are involved in PSD (Feng et al., 2014; Shi et al., 2017). Several theories have been developed to explain its pathogenesis, including the stroke site theory (Santos et al., 2009), stroke area theory (Vataja et al., 2004; Nys et al., 2005), neuronal regeneration theory (Eisch and Petrik, 2012; Eyre and Baune, 2012), inflammatory and cytokine factor theory (Li et al., 2011), neuroendocrine theory (Mitchell, 1997), vascular depression theory (Hickie et al., 1995), serotonin transporter gene theory polymorphism theory (Mak et al., 2013), and social psychology (Feng et al., 2014). PSD is also a hotspot of this research because of its high incidence and harmfulness. Related studies suggest that when the hypothalamic–pituitary–adrenal axis (HPA axis) is activated, excessive cortisol in the patient can induce depression. Neurobiology states that the activation of this axis causes excessive glucocorticoids and may have some association with PSD (Mitchell, 1997; Barra de la Tremblaye and Plamondon, 2016; Keller et al., 2017). The ABCB1 gene encodes P-glycoprotein (Sadhasivam et al., 2015), which itself has a function of expelling glucocorticoids that invade the brain. Studies have shown that the ABCB1 gene is closely related to the occurrence of depression, but the specific polymorphic sites did not have consistent results (Wang et al., 2018). Moreover, whether a correlation exists between its genetic polymorphism and PSD is still unknown. Therefore, in this study, we analyzed the expression of genotypes and alleles of the C3435T locus in the ABCB1 gene in the Han population of southern Anhui, China.
Materials and Methods
Research participants
Entry criteria: (1) age ≥18 years; (2) confirmed by the head CT scan and/or head MRI plain scan as acute ischemic stroke; (3) onset to hospitalization ≤7 days; (4) completed a 6-month follow-up and Hamilton Depression Rating Scale (HAMD) score; and (5) patients enrolled informed consent.
Exclusion criteria: (1) previous affective disorder, a history of mental disorders; (2) hemorrhagic stroke; (3) merger of other serious diseases; (4) disturbance of consciousness, severe aphasia, dysarthria, and other reasons such as refusal to participate in the investigation; and (5) associated with other serious diseases.
The patients enrolled in this study were the first patients with acute ischemic stroke admitted to the department of neurology in the First Affiliated Hospital of Wannan Medical College from January 2016 to December 2017. The study protocol was approved by the medical ethics committee of the hospital, and all enrolled patients signed a written informed consent form.
Initially, 230 patients were enrolled. According to the results of follow-up, 197 cases were included in the final research, and 33 patients were excluded. Among them, 23 patients were unable to complete the 6-month follow-up and HAMD due to disturbance of consciousness, severe aphasia, dysarthria, and other reasons; 3 patients had other serious physical illnesses; and 7 patients had a previous history of stroke.
Diagnostic criteria for PSD
All enrolled patients were followed up by trained neurologists for 2 weeks and 1, 3, and 6 months. The follow-up was mainly through outpatient and inpatient follow-up. The subjects' depression status was mainly investigated by using the HAMD questionnaire. Subjects with a score of 7 or more on the HAMD were re-evaluated by a more experienced physician. Subjects with a HAMD score ≥8 were classified as the depression group (PSD group), and those with a HAMD score <8 were treated as the nondepression (NPSD) group (Park et al., 2017). The diagnosis of PSD is subject to DSM-V of the American Psychiatric Association (Zimmerman et al., 2018).
Genotyping
The genotype of venous blood was analyzed through nonamplified fluorescence staining in situ hybridization (Beijing Precision Medical Platform analysis software). (1) Preparation of blood sample: venous blood (3–6 mL) was collected in an EDTA anticoagulant tube. The pretreatment solution (10 × NH4Cl) and double-distilled water (1:9 ratio) were added into 1 × NH4Cl working fluid. Next, 1.2 mL of the above working fluid was added to a 1.5 mL centrifuge tube, and then the collected venous blood (150–200 μL) was added to the centrifuge tube. The supernatant was discarded after centrifugation at 3000 rpm, adding 30–50 μL of Yao Jin Bao (nucleic acid purification reagents; Beijing Huaxia Times Gene Technology Co., Ltd.) after the precipitate to obtain a leukocyte suspension. Then, 1.5 μL of white blood cell suspension was added to a Yao Jin Bao dye reagent (digoxin dyeing solution; Beijing Huaxia Genetics Technology Development Co., Ltd.) and thoroughly mixed and centrifuged for a short time. After completion, the tube cap was sealed tightly, and the tube was placed in a fluorescent detector. (2) The fluorescence signal was automatically extracted by fluorescence in situ hybridization and chromosome karyotype analysis system, and the fluorescence curve was obtained. The C3435T locus of the ABCB1 gene was genotyped and was positive for control.
Statistical analysis
Statistical analysis was performed using the SPSS 21.0 software. The Hardy–Weinberg genetic balance test was performed. p > 0.05 denoted that the Hardy–Weinberg equilibrium test was consistent, indicating that the sample has group representativeness. The genotypes and allele frequencies of the two groups were compared using a chi-square test. The correlation between genotype and allele frequency and disease was analyzed through single-factor logistic regression. p < 0.05 indicated that the difference was statistically significant.
Results
Incidence of PSD
The PSD group comprised 82 patients (34 women and 48 men), and the NPSD group consisted of 115 patients (56 women and 59 men). The prevalence of PSD was 42.62%. No statistically significant difference existed between male and female subjects (χ 2 = 1.009; p = 0.315), which is shown in Figure 1.
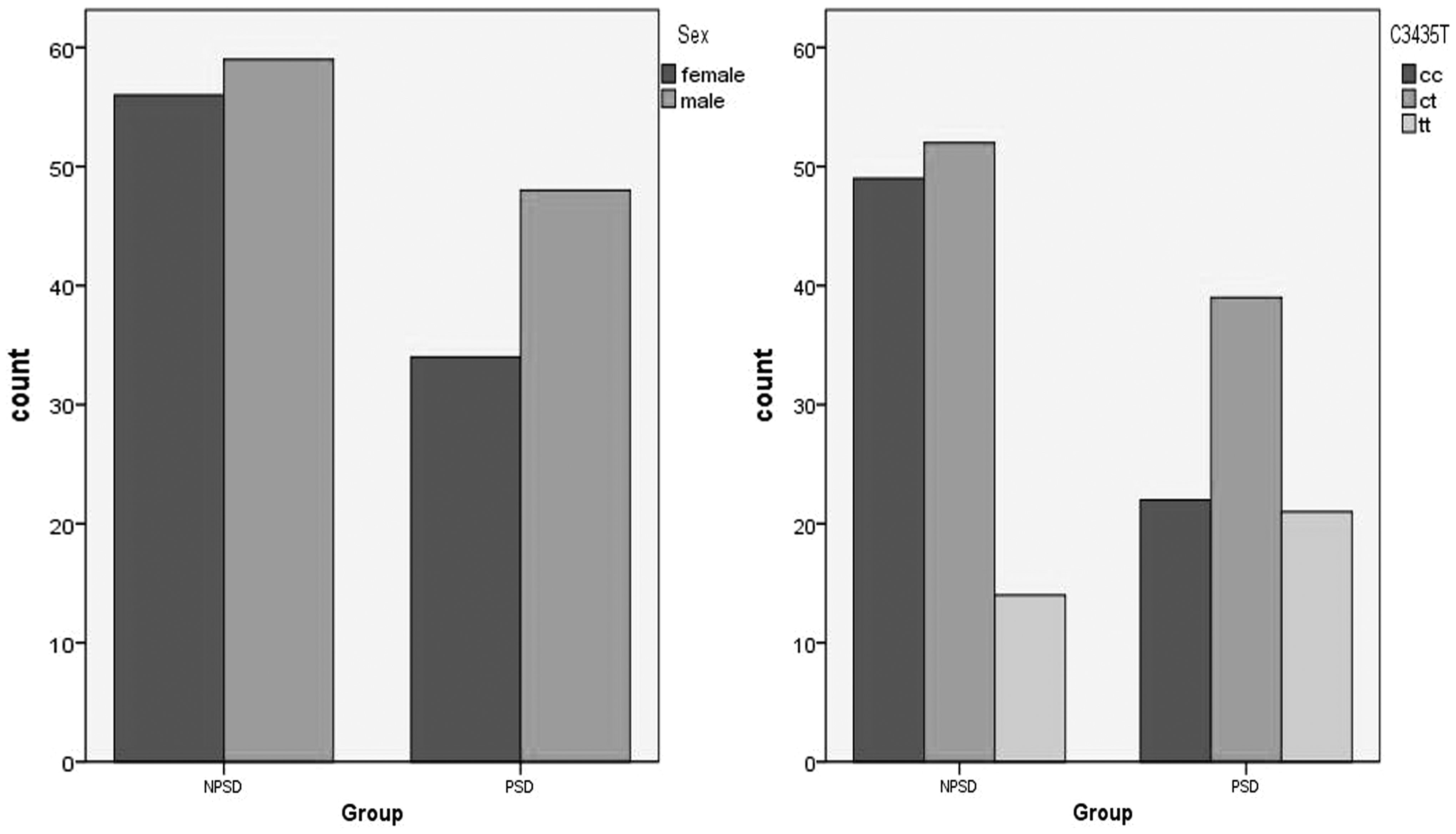
Left: gender distribution; Right: genotype distribution.
Hardy–Weinberg equilibrium test
The genotype and allelic frequencies of the C3435T among PSD and NPSD patients were analyzed using the Hardy–Weinberg equilibrium test for all polymorphisms (p > 0.05). Suggesting genetic balance, the sample from the same Mondell group, with a higher group representative, as shown in Table 1.
Hardy–Weinberg Equilibrium Test
NPSD, nondepression; PSD, poststroke depression.
Comparison of genotype and allele distribution frequency
The fluorescence signal was automatically extracted by fluorescence in situ hybridization and chromosome karyotype analysis system, and the fluorescence curve was obtained. The C3435T locus of the ABCB1 gene was genotyped and was positive for control, as shown in Figure 2.
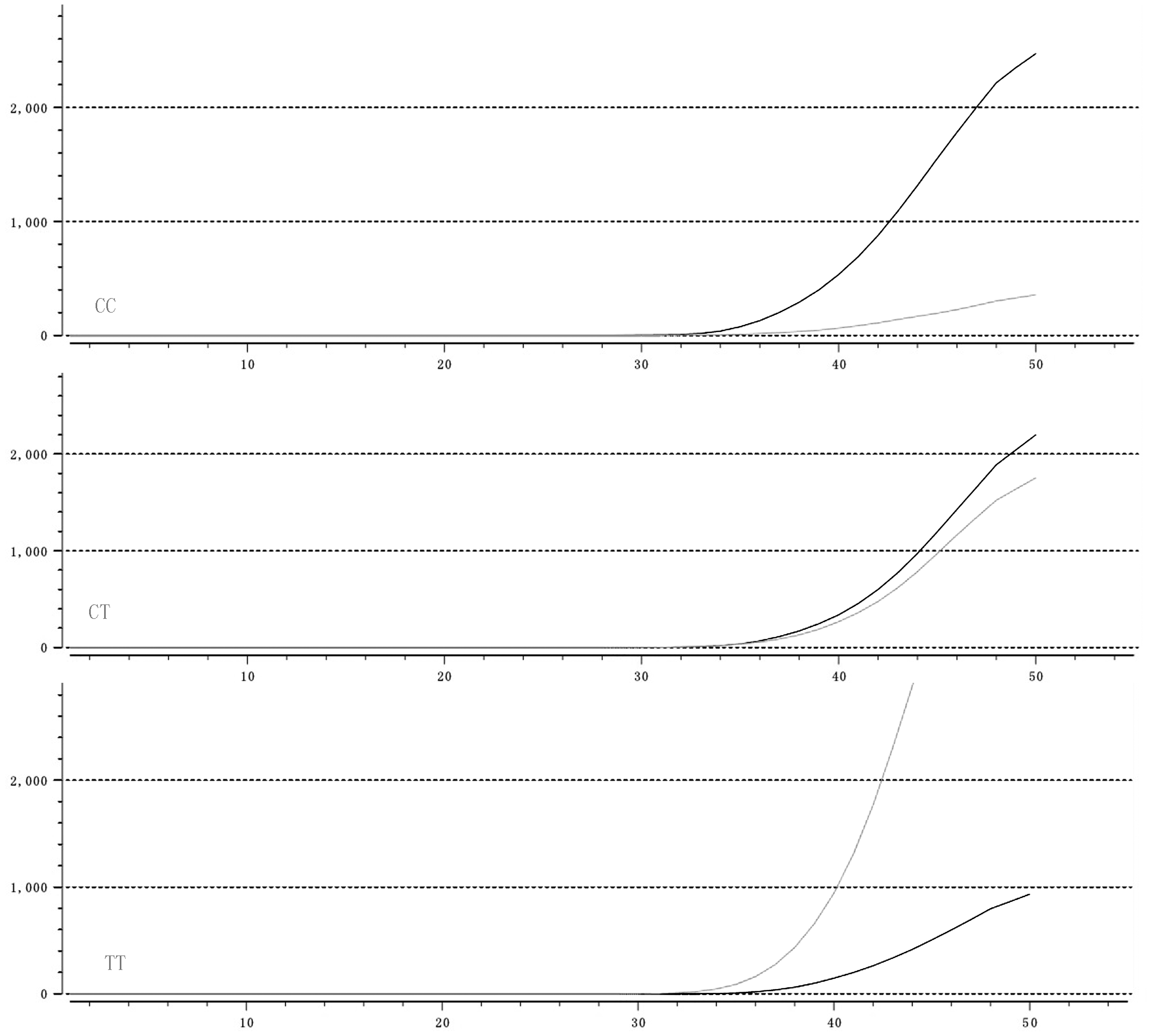
The fluorescence signal was automatically extracted by fluorescence in situ hybridization and chromosome karyotype analysis system, and the fluorescence curve was obtained. The C3435T locus of the ABCB1 gene was genotyped and was positive for control. The dark gray and light gray curves represent the fluorescence signal values automatically read by the karyotype analysis system. The two are close, representing heterozygous; the difference between the two is relatively large, representing homozygous, in which dark gray dominates CC and light gray dominates TT.
The results of genotyping in the PSD group were as follows: 22 cases of wild homozygous (CC) mutation, 39 cases of heterozygous (CT) mutation, and 21 cases of homozygous mutation (TT). The results of genotyping in the NPSD group were as follows: 49 cases of wild homozygous (CC) mutation, 32 cases of heterozygous (CT) mutation, and 14 cases of homozygous mutation (TT). The distribution frequency of genotypes between the two groups was statistically significant (χ 2 = 8.228; p = 0.016), as shown in Table 2.
Genotype And Allele Distribution Frequency of C3435T in Poststroke Depression And Nondepression
The frequencies of C and T alleles in the PSD group were 50.6% and 49.4%, respectively. Meanwhile, the frequencies of C and T alleles in the NPSD group were 65.2% and 34.8%, respectively. The frequency of allele frequencies in the two groups was statistically significant (χ 2 = 8.454; p = 0.004), which is given in Table 2.
Association analysis between genotypes and alleles and PSD
The proportions of CC, CT, and TT in the PSD group were 22 (26.8%), 39 (47.6%), and 21 (25.6%), whereas those in the NPSD group were 49 (42.6%), 52 (45.2%), and 14 (12.2%), respectively. Based on the CC genotype, the relative risk OR of the homozygous mutant TT was 3.341, and the T allele frequency in the PSD group was 49.4% higher than that in the NPSD group (34.8%). The relative risk OR value of the allele T relative to allele C was 1.830, which is given in Table 3.
Association Analysis Between Genotypes and Alleles in Poststroke Depression
Discussion
PSD is a common complication after stroke, which remarkably increases the mortality of stroke patients, interferes with the recovery of neurological functions, and has a high recurrence rate (Quaranta et al., 2012). At present, the true epidemiological data of PSD are still difficult to define due to the differences in follow-up survey methods and follow-up time, as well as the complexity of recognition and diagnosis of PSD. Previous studies and meta-analysis suggest that the incidence rate is between 30% and 60% (Srivastava et al., 2010). In this study, the data show that the prevalence of PSD is 42.62%, which is consistent with previous studies, and shows no significant difference.
At present, few studies have reported on the association between the C3435T locus gene polymorphism and PSD risk in the Han population in southern Anhui, China. Our study suggests that a correlation exists between the C3435T locus polymorphism and PSD. The proportion of allele T in the PSD group (49.4%) was greater than that in the control group (34.8%), and the proportion of homozygous mutants (25.6%) was greater than that in the NPSD group (12.2%). According to logistic regression analysis, the relative risk of TT was 3.341 in the C3435T locus with reference to CC, and the relative risk of the allele T relative to allele C was 1.830. These results suggest that this site is associated with the onset of PSD. The risk of TT genotype is 3.341 times that of the CC genotype, and the risk of carrying the T allele is 1.830 times that of the C allele. These findings further demonstrate a close relationship between the C3435T locus gene polymorphism and the prevalence of PSD.
Genetic polymorphism refers to the polymorphism of DNA sequences caused by the variation of a certain nucleotide in the genome, which is of great significance for the human genome project. This research suggests that many diseases are closely related to the susceptibility of PSD, especially for the diagnosis and identification of certain diseases that could result in depression. However, this study suggests that an important relationship exists between the C3435T locus gene polymorphism and PSD, especially in patients with mutation allele T, in which the probability of concurrent PSD is remarkably higher.
Although a few studies on the ABCB1 gene C3435T polymorphism and PSD have been conducted, C3435T is a widely studied polymorphic site in the ABCB1 gene (Abanda et al., 2017). Given the polymorphism of the locus gene, the concentration of P-glycoprotein is reduced, which leads to extensive demonstration of pharmacokinetic differences and depression (Fung and Gottesman, 2009; Bruckl and Uhr, 2016). The association of the synonymous C3435T mutation and protein expression in different organs (e.g., duodenum, intestine, placenta, liver, and kidney) has been extensively studied. However, these studies were not conclusive, with conflicting observations. A recent review suggests that the effect of ABCB1 SNPs (C1236T, G2677T/A, and C3435T) on ABCB1 expression and/or activity in various tissues (e.g., the liver, gut, and heart) appears to be small (Wolking et al., 2015). In fact, C3435T polymorphism resides in exon26 of ABCB1 gene, which results in a synonymous amino acid change, is unlikely to alter the transcription of ABCB1. One possibility is that the C3435T may be linked to unidentified SNP(s) in the promoter/3′ UTR of ABCB1 gene, which could affect transcription and lower mRNA levels. By using Tag SNP strategy, the independent impacts of multiple novel functional SNPs on ABCB1 gene expression have been revealed recently ( Shou et al., 2012). Thus, linkage analysis regarding association between the C3435T SNP and other polymorphisms in the ABCB1 promoter region in Chinese patients will be necessarily needed.
In the brain, ABCB1 is mainly expressed in blood–brain barrier (BBB), which plays an important role in controlling the passage of substances between the blood and brain. Although there is no direct evidence showing that C3435T SNP could alter ABCB1 expression level in BBB, it is also possible that, as postulated by Fung and Gottesman (2009) that synonymous C3435T SNP may have functional effect by affecting the timing of cotranslational folding and insertion of P-glycoprotein into the membrane, thus altering the structure of substrate and/or inhibitor interaction sites.
From our research results, a question inevitably arises: what is the relationship between the C3435T locus gene polymorphism and the pathogenesis of PSD? Although its mechanism of influence on PSD is unclear, the neuroendocrine theory is mainly centered around the HPA, which acts as a functional axis in response to stimulation and is activated after stroke. The most prominent change is a remarkable increase in glucocorticoids in patients (Mitchell, 1997). The C3435T site is derived from the ABCB1 gene, which encodes P-glycoprotein. The P-glycoprotein itself has the function of excreting glucocorticoids that invade the brain. The concentration or the function of P-glycoprotein is reduced, and the excessively increased glucocorticoid in the brain cannot be ruled out, leading to the occurrence of PSD.
Until now, the exact pathogenesis of PSD remains unclear. The C3435T locus gene polymorphism may be a candidate gene for early recognition of PSD. We can boldly assume that the genetic polymorphism C3435T results in decreased P-glycoprotein expression, which causes a severe increase in intracranial glucocorticoid levels in stroke patients and thus induces PSD.
Our study presents several limitations. It is not multicentered, and the sample size, follow-up method, and time setting are limited. These drawbacks all limit the accuracy of this study to a certain extent. Moreover, several other factors remain to be studied in the future. However, our data do suggest that there is a correlation between the C3435T gene polymorphism and PSD in the Han population in South Anhui Province, China, whereas other underlying possible likelihood could not be excluded absolutely.
Footnotes
Acknowledgments
This study was supported by Natural Science Foundation of China (Grant No. 81171110, awarded to Z.Z.) and Wannan Medical College Youth Fund, China (Grant No. KY86700312, awarded to D.X.). The authors thank Dr. Kun Lu for his valuable technical assistance.
Disclosure Statement
No competing financial interests exist.