
Abstract
Immune thrombocytopenia (ITP) is an autoimmune-mediated hemorrhagic disease. Emerging evidence indicates that FOXO1 SNPs are related to the immune dysregulation of several autoimmune diseases suggesting that FOXO1 may be involved in inflammation and pathologic activities in patients with ITP. This study aimed to evaluate whether FOXO1 gene single-nucleotide polymorphisms (SNPs) are associated with susceptibility to ITP and clinical priorities of concern include bleeding severity and sensitivity of glucocorticoid treatment. This study recruited 327 newly diagnosed ITP and 220 healthy controls. Four SNPs (rs17446593, rs17446614, rs2721068, and rs2721068) of the FOXO1 gene were detected using the Sequenom MassArray system. Bleeding severity were classified into the mild and severe groups based on the bleeding scores. ITP patients were classified as sensitive and insensitive to glucocorticoid treatment according to the practice guideline for ITP (2019 version). The frequencies of the four SNPs did not show any significant differences between the ITP and healthy control groups. Patients with AA genotype at rs17446593 (p = 0.009) and GG genotype at rs17446614 (p = 0.009) suffered more severe bleeding than patients without them. Carriers of haplotype Grs17446593Ars17446614Crs2721068Trs2755213 were protective to severe bleeding (p = 0.002). The AA genotype at rs17446593 was significantly higher in ITP patients sensitive to glucocorticoid treatment than in those insensitive to glucocorticoid treatment (p = 0.03). Haplotype Grs17446593Grs17446614Trs2721068Trs2755213 increases the risk of glucocorticoid resistance (p = 0.007). Although FOXO1 gene polymorphisms were not associated with susceptibility to ITP, the AA genotype at rs17446593 and GG genotype at rs17446614 were associated with bleeding severity. Haplotype GACT have a protective effect against severe bleeding. Patients with AA genotype at rs17446593 may tend to have good responds to glucocorticoid treatment. However, the FOXO1 gene haplotype GGTT increases the risk of glucocorticoid-resistant. Trial registration: ChiCTR1900022419.
Introduction
Immune thrombocytopenia (ITP), one of the most common bleeding disorders in pediatrics, is an acquired autoimmune disease characterized by a reduced platelet count and an increased risk of bleeding (Neunert et al., 2019). Although the majority of bleeding complications in ITP patients are minor, major bleeds, especially in patients with severe thrombocytopenia (platelet counts below 20 × 109/L), can result in death or significant disability. High bleeding severity and glucocorticoid treatment resistance are what clinician concerned extremely in pediatric patients (Neunert et al., 2015). Immune dysregulation such as T helper cells polarization, increased Th17/Treg ratio, and higher CD8+ CTL, as well as a highly imbalanced cytokine secretion pattern (Aslam et al., 2012; Gu et al., 2021; Zufferey et al., 2017) and/or multiple genetic factors, contribute to ITP pathogenesis (Cines et al., 2009; McMillan et al., 2004). Several reports describe genetic disease susceptibility loci.
Many SNPs have been reported to be associated with ITP susceptibility, clinical presentation, and outcome of clinical intervention, including many immune system-related genes, such as IL-10, TNFα, IL-17, TGF-β, STAT1, FOXP3, CTLA-4, and CARD9 (AbdelGhafar et al., 2020; Chen et al., 2015; Doaa et al., 2015; Kasamatsu et al., 2018; Li et al., 2017; Sheng et al., 2019; Soliman et al., 2018; Tolba et al., 2019; Zhang et al., 2019).
FOXO1 gene encodes the forkhead transcription factor O1 (FOXO1) and plays an essential role in the development and differentiation of immune cells to keep immune homeostasis. FOXO1 can maintain naive T cell quiescence and survival, enhance the formation and function of regulatory T cells and inhibit the T-helper 17 cells, promote antibody production. Moreover, transcriptome analysis uncovered that FOXO1 protein regulates a series of Treg-associated genes, including CTLA-4 and interleukin-7 receptor subunit-α (IL-7Rα) (Adriana, 2017; Bothur et al., 2015; Hawse et al., 2015; Ouyang et al., 2012). These negative effects on patient's immune system were known to be closely associated with pathogenesis and development of ITP. Accordingly, the abnormality of FOXO1 expression or post-translational modification mediates the pathogenesis of many autoimmune diseases, including psoriasis (Li et al., 2018), systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and so on (Liu et al., 2017).
In addition, several studies show that FOXO1 SNPs are associated with susceptibility to carotid atherosclerosis (Muller et al., 2015), early-onset type 2 diabetes (T2D) (Kedenko et al., 2014), and relapsing-remitting MS (Edgünlü et al., 2020). However, few studies attempt to clarify the link between FOXO1 polymorphism and ITP.
This study aimed to explore the role of FOXO1 gene polymorphisms and their relationship with ITP (in a well characterized-clinical cohort of Chinses pediatric patients). We also analyzed the bleeding severity and sensitivity of glucocorticoid treatment among pediatric ITP patients with these gene polymorphisms.
Materials and Methods
Enrollment of patients
A total of 327 children with ITP and 220 gender- and age-matched healthy controls were recruited prospectively between October 2009 and January 2020 from the Department of hematology of Beijing Children's Hospital. All subjects were Han Chinese, and no genetic associations were found between any participants. Written informed consent was obtained from each participant's legal guardians or themselves, and this study was approved by the Research Ethics Committee at the Beijing Children's Hospital. The diagnosis of ITP was consistent with the criteria of a practice guideline for
Inclusion in the study required the absence of other causes of secondary thrombocytopenia based on patient history, physical examination, clinical manifestations, and laboratory tests. Patients with other autoimmune or hemorrhagic diseases (e.g., SLE, severe anemia), or thrombocytopenia due to virus, familial, or drug-induced etiologies were excluded in this study. For each patient, demographic data and clinical presentations were collected during the initial enrollment and the 1-year follow-up was completed through outpatient visits or telephone. In the validation cohort, DNA samples were collected from 153 pediatric ITP patients who were consecutively enrolled from 2014 to 2018 and who were different from the patients of the first cohort. The study design was approved by the Beijing Children's Hospital, Capital Medical University Ethics Committee (approval No. 2018-k-97).
The bleeding severity was classified according to the bleeding score ranges from grade 0 to 4. Grade 0 refers to no bleeding. Grade 1 refers to few petechiae (≤100 total) and/or five or less small bruises (≤3 cm in diameter), and no mucosal bleeding. Grade 2 refers to many petechiae (>100 total) and/or five or more large bruises (>3 cm in diameter), and no mucosal bleeding. Grade 3 refers to mucosal bleeding and troublesome lifestyle. Grade 4 refers to bleeding leading to decrease in Hb >2 g/dL or suspected internal hemorrhage. Children with a bleeding score of 2–4 were placed in the severe bleeding group.
According to the criteria of clinical response of International Working Group, ITP patients were divided into three groups after glucocorticoid treatment (prednisone (PDN) 2 mg/kg/d (maximum 60 mg/day) for 2 consecutive weeks or 0.6 mg/kg/day dexamethasone (maximum 40 mg/day) by intravenous infusion for 4 consecutive days.), which were “Complete Response” (CR), “Response” (R), and “No Response” (NR). Patients were considered NR if they met any of the following criteria: (1) a platelet count that did not reach 30 × 109/L; (2) did not have a two-fold rise in platelet count compared with their baseline level; and (3) had continued issues with bleeding after 2 weeks of standard dose glucocorticoids. ITP patients who responded appropriately to glucocorticoid treatment were considered CR and R.
The criteria of CR included a platelet count that reached 100 × 109/L and did not have continued issues with bleeding after normal dose glucocorticoids. The criteria of R included a platelet count that reached 30 × 109/L, had a two-fold rise in platelet count compared with their baseline level, and did not have continued issues with bleeding after normal dose glucocorticoids.
DNA extraction
Whole blood samples (2 mL) were collected from children in vacuum tubes containing 5% EDTA. Peripheral blood mononuclear cells (PBMCs) were isolated by a standard protocol. Genomic DNA was extracted according to the manufacturer's instruction of QIAamp DNA Mini Kit (Qiagen, Hilden, Germany).
Genotyped of four SNPs in FOXO1 gene by sequenom massarray
We eventually chose four SNPs (rs17446593, rs17446614, rs2721068, and rs2755213) located in the intron of the FOXO1 gene from the Hapmap database (www.hapmap.org). Haploview software (2MIT Media Lab, Cambridge, MA) was used in the analysis of the haplotype maps (Barrett et al., 2005). Also, the genotype of four selected SNPs was detected by the Sequenom MassArray system (Sequenom, San Diego, CA), which is based on a multiplex PCR. To confirm the results of the genotyping, 10% of samples were randomly selected for DNA sequencing per SNP site. The sequences of primer are shown in Table 1.
Primer List of Single-Nucleotide Polymorphism
CHB, Chinese Han in Beijing.
RNA extraction and real-time quantitative PCR detection for FOXO1
The mRNA from PBMC of 65 patients, who were admitted to the hospital without receiving any ITP-specific treatments, was isolated by TRIzol reagent (Invitrogen Life Technologies, Carlsbad, CA). The reverse transcription reactions were using M-MLV RT-PCR kit (Solarbio) and quantitative PCR was performed on the ABI 7500 Real-Time PCR System (Applied Biosystems, Foster City, CA). The housekeeping gene β-actin was used to normalize mRNA. Each PCR reaction was repeated three times. The primers for FOXO1 and GAPDH are shown in Table 2.
Primer List of Real-Time Quantitative Polymerase Chain Reaction Detection
Statistical analysis
Statistical analysis was performed using SPSS 26.0. The p-value of Hardy–Weinberg equilibrium (HWE), genotype, and allele frequencies were calculated using the chi-square test or Fisher's exact test (when the expected frequencies <5). Adjusted p values and odds ratios (ORs) with a corresponding 95% confidence interval (95% CI) were analyzed by Univariate binary logistic regression analyses. The haplotype analysis was performed by SHEsis online after removing the subjects with missing SNP. The mRNA expression levels of FOXO1 among the several FOXO1 SNPs genotype groups were analyzed using Mann–Whitney U test. p < 0.05 was considered statistically significant.
Result
Study population
The demographic and clinical characteristics of participants are shown in Table 3. No observed difference in gender and age between the patient group and the healthy control group (p > 0.05). All selected SNPs in the control group were in agreement with the Hardy–Weinberg equilibrium (p > 0.05, shown in Table 4). Among all children in the current study, a total of 283 patients accepted corticosteroid treatment.
The Characteristics of the Subjects
p < 0.05.
M, male; F, female; NA, not applicable; ITP, primary immune thrombocytopenia.
Distribution of the Genotype and Allele Frequencies of Selected FOXO1 Single-Nucleotide Polymorphisms in All Patients with Immune Thrombocytopenia and Controls
SNPs, single-nucleotide polymorphism; n, number; HWE-p, p-value of Hardy–Weinberg equilibrium.
p value calculated with the chi-squared test; Bold highlights statistical significance (p < 0.05).
Association between FOXO1 SNPs and ITP susceptibility
No significant statistical difference for the four SNP genotypes were observed between the ITP group and healthy controls (rs17446593, p = 0.1808; rs17446614, p = 0.2218; rs2721068, p = 0.8256; and rs2755213, p = 0.9912). Similarly, negative results were found in the four selected SNP loci allele frequencies (Table 4).
Association between FOXO1 SNPs and bleeding severity
All the patients were classified to nonsevere group (N = 119) and severe group (N = 208, included NBS-2 = 134, NBS-3 = 74, NBS-4 = 0). We next explore the association between the four SNPs and the bleeding severity of ITP (Table 5). Genotypic frequencies of the rs17446593 and rs17446614 were statistically different between severe and nonsevere groups (p = 0.009). Patients with AA genotype at rs17446593 (p = 0.009) and GG genotype at rs17446614 (p = 0.009) suffered more severe bleeding than patients without them. However, no significant association was observed in the other two selected SNPs. In addition, Allele G of rs17446593 and Allele A of rs17446614 was significantly associated with nonsevere bleeding (rs17446593: OR = 0.504, 95% CI = 0.328–0.775, p = 0.002; rs17446614: OR = 0.453, 95% CI = 0.276–0.735, p = 0.002).
Association Between Selected FOXO1 Single-Nucleotide Polymorphisms and Immune Thrombocytopenia Bleeding Severity
p value calculated with the chi-squared test; adjusted p value calculated by univariate logistic regression; Bold highlights statistical significance (p < 0.05).
n, number; OR, Odds Ratio; CI, Confidence Interval; ref, reference; NA, not applicable.
Association between FOXO1 SNPs and sensitivity to corticosteroid therapy
Besides exploring associations with the susceptibility and bleeding severity of ITP, we studied the association between the four SNPs and outcomes of corticosteroid therapy as well. All patients who accepted corticosteroid therapy were divided into the corticosteroid-sensitive group (n = 174) and the corticosteroid-resistant group (n = 109). After adjusting for age and gender by univariate binary logistic regression, the results showed no statistically different distribution of alleles and genotypes under the codominant model of the four SNPs between the corticosteroid-resistant and corticosteroid-sensitive groups. However, ITP children carrying the AA genotype of rs17446593 was significantly higher in ITP patients sensitive to corticosteroid treatment than the others under the dominant model (OR = 0.558, 95% CI = 0.334–0.932, p = 0.03) (Table 6).
Association Between Selected FOXO1 Single-Nucleotide Polymorphisms and Sensitivity to Corticosteroid Therapy
p value calculated by univariate logistic regression; Bold highlights statistical significance (p < 0.05).
n, number; ref, reference; NA, not applicable.
Validation cohort to investigate bleeding severity and steroids sensitivity of rs17446593
To confirm the results of the rs17446593 SNP, we performed genotyping using a “validation cohort” of patients with ITP (N = 153). As shown in Table 7, the results of the validation cohort indicated a difference between patients' severe bleeding and nonsevere bleeding (p = 0.046). Moreover, we investigated the association of the rs17446593 SNP with corticosteroid treatment. There was a significant difference between patients sensitivity to corticosteroid treatment and insensitivity to corticosteroid treatment (p = 0.029).
Genotype of rs17446593 Single-Nucleotide Polymorphism in Immune Thrombocytopenia Patients with Different Bleeding Severity and Sensitivity to Corticosteroid Treatment in the Validation Cohort (N = 153)
p value was estimated by Fisher's exact test.
GT, glucocorticoid treatment.
Analysis of haplotype
The combined effects of FOXO1 gene and four SNPs on glucocorticoid sensitivity and bleeding severity were estimated by haplotype analysis (Tables 8 and 9). The Global χ 2 and p-value for haplotype analysis of glucocorticoid sensitivity was 8.06 and 0.045, respectively. The Global χ 2 and p-value for haplotype analysis of bleeding severity was 11.11 and 0.004, respectively. Grs17446593Grs17446614Trs2721068Trs2755213 was the most common haplotype in the different phenotype subjects. Haplotype analysis showed that haplotype Grs17446593Grs17446614Trs2721068Trs2755213 (OR = 0.138, 95% CI = 0.026–0.731, p = 0.007) increases the risk of glucocorticoid-resistant. Carrier of haplotypes Grs17446593Ars17446614Crs2721068Trs2755213 (OR = 0.46, 95% CI = 0.279–0.459, p = 0.002) were protective to severe bleeding.
Haplotype Analysis of Four Polymorphism Site of FOXO1 in Immune Thrombocytopenia Glucocorticoid Sensitivity
Statistically significant values are shown in bold.
SNPs sequence: rs17446593, rs17446614, rs2721068, rs2755213. Global χ 2 = 8.06, p-value = 0.045.
Haplotype Analysis of Four Polymorphism Site of FOXO1 in Immune Thrombocytopenia Bleeding Severity
Statistically significant values are shown in bold.
SNPs sequence: rs17446593, rs17446614, rs2721068, rs2755213. Global χ 2 = 11.11, p-value = 0.004.
The mRNA levels of FOXO1 gene in several genotypes of ITP patients
To explore the potential effects of the gene polymorphism on FOXO1 expression, we examined the expression at the mRNA level of 65 patients by RT-PCR. However, the discrepancy in FOXO1 levels was not observed among the different genotypes of all four selected SNPs in ITP patients (rs17446593, p = 0.861; rs17446614, p = 0.966; rs2721068, p = 0.389, and rs2755213, p = 0.374, respectively) (Fig. 1).
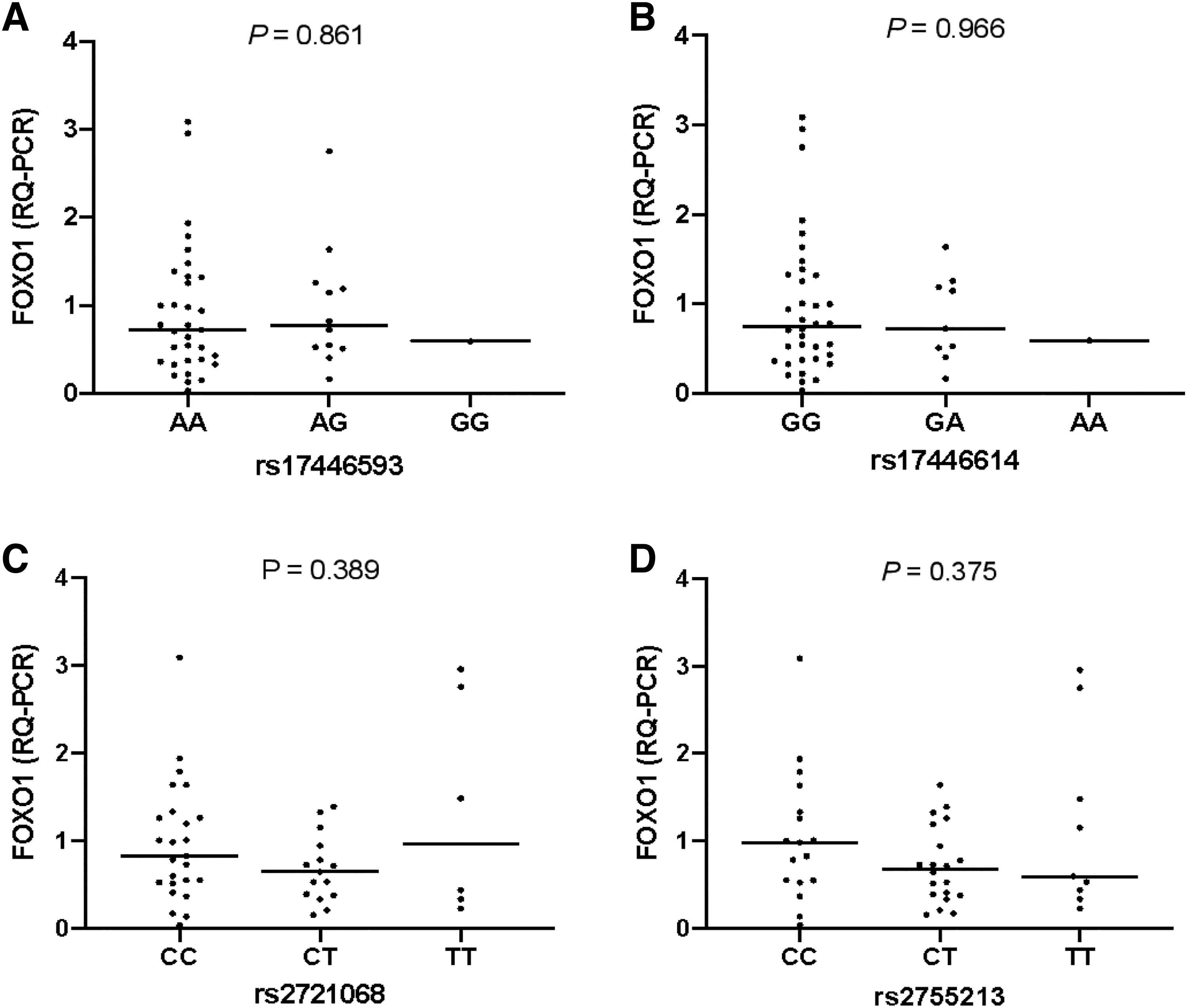
The mRNA levels of FOXO1 gene in several ITP groups according to genotypes. There were no significant differences of mRNA expression levels of FOXO1 gene in different genotype subgroups
Discussion
As we know, many studies have identified genes associated with the risk of severe bleeding, and resistant to glucocorticoid treatment includes SIRT1 (rs12778366 and rs4746720), SDF1 (rs266085), ABCB1 (C1235T, G2677T/A, and C3435T), TNFα (−308AG), and IL-23R (rs1884444) (Gu et al., 2023). FOXO1 can maintain naive T cell quiescence and survival, enhance the formation and function of regulatory T cells and inhibit the T-helper 17 cells, and promote antibody production, which is closely associated with ITP pathogenesis of imbalance of Treg/Th17 axis in our previous study (Gu et al., 2021). FOXO1, as an essential regulator of spontaneous T cell activation, effector T cell differentiation, and autoantibody production (Ouyang et al., 2009), few studies have explored potential of FOXO1 SNP associated with autoimmune cytopenia manifestation and corticosteroid sensitivity. Herein, we report that the FOXO1 SNP is a related factor for bleeding severity and glucocorticoid treatment sensitivity in pediatric patients with ITP.
Forkhead box O signaling pathway is an important upstream regulatory mechanism for autoimmune, which can promote the expression of FOXP3, TGF-β, and CTLA-4 to increase the number and function of regulatory T cells (Homan et al., 2021). Meanwhile, FOXO1 can bind to the RORγt promoter region and inhibit the IL-23R, IFN-γ, and IL-17A expression, resulting in a downregulation of the immune response (Lainé et al., 2015). In addition, FOXO1 has been demonstrated to be essential for B cell proliferation, isotype switching, and efficient affinity maturation (Zaiss and Coffer, 2018). These effects of FOXO1 work together to maintain the balance of the immune system and prevent the occurrence of autoimmune diseases.
SNP is the most common form of human heritable variation and may alter gene expression and function, Previous studies have shown that the FOXO1 SNPs are associated with susceptibility to type 2 diabetes (Bottcher et al., 2007; Muller et al., 2015), sepsis, and progressive relapsing multiple sclerosis (Edgünlü et al., 2020). A study performed by Müssig K suggested that rs17446614 and rs2721068 FOXO1 SNPs were associated with beta cell function and increased susceptibility to T2D (Müssig et al., 2009). Recently, a study with a Chinese Han population has demonstrated that rs2721068 and rs17446614 FOXO1 SNPs were correlated with a predisposition to sepsis (Wang et al., 2019). Our study showed that the distribution of four selected FOXO1 SNPs did not exhibit significant deviation in ITP patients and controls.
However, the polymorphisms of the rs17446593 and rs17446614 were significantly associated with the bleeding severity of ITP. We can propose that the initiation of ITP is attributed to triggering factors such as bacterial or viral infection (Swinkels et al., 2018) regardless of the FOXO1 genotype, but once the autoimmune disorder starts, FOXO1 and its target gene can affect the extent of autoimmune platelet destruction and the response of treatment. In addition, the rs17446593 associated with sensitivity to glucocorticoid treatment as well suggested that there may be some intrinsic connection between the bleeding severity in primary ITP and the sensitivity to glucocorticoid treatment. In the validation cohort, the genotype of rs17446593 SNP in ITP patients showed different bleeding severity and sensitivity to glucocorticoid treatment as well. Haplotype analysis has more statistical power than a single SNP because it contains multiple SNPs located in the same homologous chromosome and descended together.
We identified four haplotypes in FOXO1. Haplotype Grs17446593Grs17446614Trs2721068Trs2755213 increases the risk of glucocorticoid-resistant, however, carrier of haplotypes Grs17446593Ars17446614Crs2721068Trs2755213 were protective to severe bleeding. However, no relationship between the genotype and the mRNA expression of the FOXO1 gene was observed. The possible reason is that all of the four selected SNPs are located in intron regions of FOXO1. However, it does not exclude the potential effect of the selected SNPs of FOXO1 in the ITP. On the one hand, both the protein activity and expression level may be affected by the gene sequence variation of SNP (Bauer et al., 2009). In several studies about autoimmune diseases, it has been demonstrated that the post-translational modification of FOXO1 was involved in the pathogenesis rather than the abnormality of mRNA expression (Chen et al., 2020).
On the other hand, these four selected SNPs are all located in interspersed repeat elements of the genome, which can regulate gene expression by cis/trans regulator (Bujko et al., 2015).
These works point out that the relevance and functionality of this polymorphism over the transcription of FOXO1 are involved in ITP bleeding severity and the sensitivity to glucocorticoid treatment, which clinicians are concerned more about. Especially in this study, the rs17446593 A allele and A/A genotype showed a high risk of bleeding but low tendence to glucocorticoid-resistance. In our center, aggressive glucocorticoid treatment will be given to pediatric primary ITP patients with severe bleeding and showed a well initial response. Few ITP patients with mild clinical symptoms received pharmacological treatment at diagnosis.
However, chronicity at 12 months was not affected by different therapeutic approaches at diagnosis or response to therapy. Side effects of glucocorticoid treatment are what pediatrician concerned. When the pediatric patient showed a tendency to glucocorticoid insensitivity, an escalating treatment strategy and the long-term treatment with eltrombopag will be applicated. Studies on correlation of ITP bleeding severity and treatment sensitivity and other population of FOXO1 (rs17446593) are needed.
Conclusion
Although FOXO1 gene polymorphisms were not associated with susceptibility to ITP, the AA genotype at rs17446593 and GG genotype at rs17446614 were associated with severe bleeding. The AA genotype at rs17446593 was associated with the sensitivity to glucocorticoid treatment of ITP patients, suggesting that the rs17446593 SNP may contribute to the sensitivity of glucocorticoid treatment in pediatric ITP patients. The FOXO1 gene haplotype GGTT increases the risk of glucocorticoid-resistant. Haplotype GACT has a protective effect against severe bleeding. This work may provide a new point for pediatric ITP's bleeding severity and glucocorticoid treatment response prediction.
Ethics Approval and Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Capital Medical University. Patients (or their parent or legal guardian in the case of children under 16) signed informed consent regarding publishing their data and photographs.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported, in part, by grants from the National Natural Science Foundation of China (no.81970111), Beijing Natural Science Foundation of China (No. 7232051,7192064)