
Abstract
Radiation-induced intestinal injury is one of the most common intestinal complications caused by pelvic and abdominal tumor radiotherapy, severely impacting patients’ quality of life. Ionizing radiation, while killing tumor cells, inevitably damages healthy tissue. Radiation-induced enteropathy results from radiation therapy-induced intestinal tissue damage and inflammatory responses. This damage involves various complex molecular mechanisms, including cell apoptosis, oxidative stress, release of inflammatory mediators, disruption of immune responses, and imbalance of intestinal microbiota. A thorough understanding of these molecular mechanisms is crucial for developing effective prevention and treatment strategies.
Introduction
In recent decades, radiation toxicity has emerged as a global concern. The high-energy radiation waves used in radiation therapy inevitably harm healthy cells, leading to various forms of radiation toxicity (Kordahi & Chassaing, 2021). Radiation therapy is one of the effective methods for treating malignant tumors, with studies estimating that approximately 50% of cancer patients receive radiation therapy (Hauer-Jensen et al., 2014). Ionizing radiation (IR) refers to the energy released by atoms in the form of particles (neutrons, α or β particles) or electromagnetic waves (X-rays or γ-rays), ionizing atoms or molecules (Obrador et al., 2020). Although efforts are made to minimize exposure to normal tissues during radiation therapy, damage to normal tissues is inevitable. Intestinal tissue is one of the most radiation-sensitive organs in the abdomen (Kai, 2021), and the sensitivity of different parts of the intestine to radiation varies, with the incidence from high to low being rectum, sigmoid colon, transverse colon, ileum, jejunum, and duodenum. Among them, radiation-induced rectal injury is the most common and stubborn (Henson et al., 2011). The small intestine is less tolerant to radiation compared to the colon and rectum. However, due to its peristalsis, the small intestine constantly changes position, minimizing continuous radiation exposure and resulting in relatively less damage. In contrast, the rectum and colon are relatively fixed, making them more susceptible to higher doses during intracavitary irradiation for most gynecological tumors, thereby increasing the risk of bowel injury. Therefore, the incidence of radiation enteropathy is closely linked to the radiation dose. Currently, endoscopy techniques such as colonoscopy and capsule endoscopy serve as the primary diagnostic methods for radiation enteropathy, enabling precise localization of stenosis and bleeding sites (Hokama, 2023).
When the total radiation dose is below 30 Gy, the likelihood of radiation enteritis is minimal. However, as the radiation dose exceeds 50 Gy, the probability increases significantly. Given that typical therapeutic doses for tumors often surpass 50 Gy, radiation damage frequently affects the intestines near the target area. Clinical manifestations of radiation-induced intestinal injury (RIII) typically include vomiting, anorexia, abdominal pain, and diarrhea, and in severe cases, complications such as intestinal obstruction and perforation may occur (De Ruysscher et al., 2019; Wang et al., 2018). Currently, the most common approach remains to reduce radiation doses, even if it means foregoing treatment of certain target areas, inevitably compromising treatment efficacy. The specific mechanisms underlying RIII are not yet fully understood, but they primarily involve damage to intestinal epithelial cells, disruption of intestinal barrier function, inflammatory responses, immune dysregulation, and microbiota imbalance (Fan et al., 2022; Ren et al., 2023). Therefore, a better understanding of the effects of radiation therapy on the intestines and the molecular mechanisms of RIII can help improve treatment effectiveness and alleviate adverse reactions (Fig. 1).
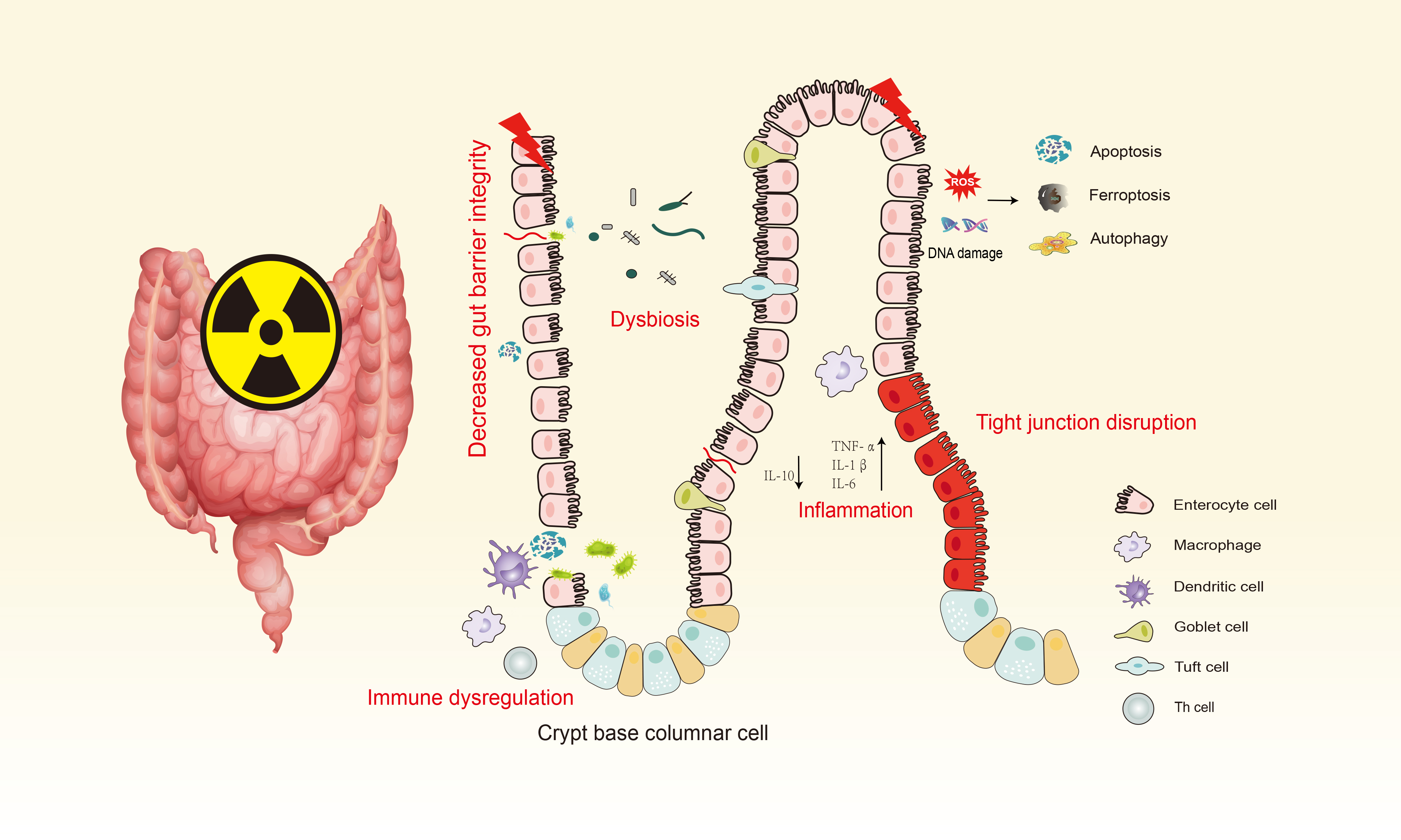
After exposure to IR, the intestine can suffer from radiation enteropathy. When IR traverses intestinal tissues, it interacts with water molecules, generating numerous free radicals, leading to oxidative stress, DNA damage, and eventually cell death. Oxidative stress and cellular damage activate the immune system, prompting the production and release of inflammatory cytokines, triggering an inflammatory response. This results in altered intestinal permeability, mutations, reduction, or loss of tight junctions between intestinal epithelial cells, increasing intercellular permeability and allowing bacteria, endotoxins, and large molecules to enter the systemic circulation. This also induces excessive activation of the immune system, exacerbating the inflammatory response and causing radiation-induced intestinal damage. IR, ionizing radiation.
DNA Damage and Oxidative Stress
DNA damage and oxidative stress response are two primary mechanisms of IR. IR can interact directly or indirectly with DNA within intestinal epithelial cells. Direct interaction refers to high-energy particles released by IR directly interacting with DNA molecules, causing direct DNA damage. Indirect interaction involves IR interacting with water molecules in intestinal cells, generating free radicals that subsequently react with DNA. These interactions lead to alterations in DNA structure, including single-strand breaks (SSBs) and double-strand breaks (DSBs) (Kavanagh et al., 2013; Yao et al., 2018; Zhao et al., 2020). DSBs in DNA are among the most severe damages caused by IR. When cells experience DSBs, they initiate DNA repair mechanisms. If DSBs cannot be completely repaired or repair fails, these irreparable DNA damages further activate pathways leading to cell apoptosis, such as cell death, chromosomal aberrations, and genomic instability. Importantly, abnormal repair and genetic mutations following DNA damage are critical steps in tumor development (Huang & Zhou, 2020; Kavanagh et al., 2013; Yao et al., 2018). In addition, IR exhibits bystander effects, where irradiated cells transmit signals to neighboring or distant nonirradiated cells, causing various biological dysfunctions in the nonirradiated cells (Rusin et al., 2018). It activates a variety of signaling pathways in bystander cells, including NF-κB, MAPK, and Jun N-terminal kinase (JNK), leading to altered expression of stress response genes, activation of DNA damage repair, proliferation, apoptosis, and death of bystander cells (Wang et al., 2021).
In addition, when IR passes through intestinal tissues, it not only interacts with water molecules to cause DNA damage but also produces a large number of free radicals, leading to the occurrence of oxidative stress (Goldstein & Kastan, 2015). Radiation-induced oxidative stress exacerbates tissue pathological changes, macrophage and neutrophil infiltration, and increases the levels of serum pro-inflammatory cytokines and peroxidation products (Tian et al., 2020). Reactive oxygen species (ROS) is one of the most important active substances in the process of oxidative stress and participates in many important cellular activities, such as gene transcription, signal transduction, and immune response (Mittal et al., 2014). These oxygen free radicals will undergo irreversible oxidative reactions with biological macromolecules in cells, leading to cell dysfunction, lipid peroxidation, and DNA damage (Fischer et al., 2018; Philchenkov, 2018), and eventually irreversible cell damage and death. IR can directly or indirectly cause damage and death of intestinal mucosal cells and endothelial cells, making them unstable and increasing cell membrane permeability. These injuries and deaths lead to the destruction of the intestinal epithelial barrier and the imbalance of the intestinal microflora, which in turn cause symptoms such as intestinal inflammation and ulcers. A large number of ROS are produced, and cytotoxicity occurs in the hours to years after exposure to IR (Khodamoradi et al., 2020). Since 80% of the human body is water, intestinal damage is closely related to oxidative stress (Tang & Loganovsky, 2018).
Cell Death
Cell apoptosis is one of the important mechanisms underlying RIII, which is a major cause of cell death in highly radiation-sensitive organs such as the gastrointestinal system, bone marrow, testes, and skin (Ashrafizadeh et al., 2019). Cell apoptosis is a genetically regulated, energy-dependent, programmed cell death process, characterized by cell shrinkage, apoptotic body formation, and ultimately engulfment by surrounding cells, making it one of the most important types of cell death (Yang et al., 2017). Once the dose is sufficiently high, the radiation effects mostly manifest as destructive (Jiao et al., 2022). After IR, multiple signaling pathways are activated, such as the P53 signaling pathway, Bcl-2 family, and Caspase family, ultimately leading to apoptosis and loss of intestinal epithelial cells. P53 is an important transcription factor that regulates the expression of downstream genes, participating in maintaining cellular genomic stability, regulating the cell cycle and apoptosis processes (Gudkov & Komarova, 2003; Srinivas et al., 2019), and playing a crucial biological role in the occurrence of RIII (Nie et al., 2022). The Bcl-2 family is an important regulator of apoptosis. The Bcl-2 protein family includes antiapoptotic proteins (such as Bcl-2, Bcl-xL) and pro-apoptotic proteins (such as Bax, Bad). IR can affect the expression of Bcl-2 family members, thereby altering cell sensitivity to apoptosis. The Caspase family is the key executor of cell apoptosis, and IR can activate members of the Caspase family, such as Caspase-3, Caspase-8, and Caspase-9, ultimately triggering cell apoptosis.
In addition to apoptosis, recent studies have shown that ferroptosis (Wang et al., 2023; Zhang et al., 2022), pyroptosis (Kiang et al., 2022), and autophagy (Foerster et al., 2022; Qu et al., 2020) are also associated with radiation-induced intestinal epithelial damage. Regulating these types of cell death could serve as potential strategies to mitigate radiation injury, thereby helping reduce radiation-induced mortality (Chen et al., 2019) (Fig. 2). Ferroptosis is an iron-dependent regulated cell death mechanism characterized by lipid peroxidation, depletion of glutathione (GSH), and iron accumulation as a key event. Radiation induces the generation of ROS and oxidative stress, which may further increase lipid peroxidation and promote ferroptosis. Current findings suggest that ferroptosis enhances cancer cell death during radiotherapy but also mediates radiation-induced organ damage (Lei et al., 2020; Wang et al., 2022; Xie et al., 2020). In the study by Peizhong Kong et al. (Kong et al., 2023), IR induces ferroptosis in mouse small intestine through activation of the STAT1-IRF1-ACSL4 pathway. Another study has found that NCOA4-mediated ferritinophagy is involved in ionizing radiation-induced ferroptosis of intestinal epithelial cells (Zhou et al., 2022). Pyroptosis is a pro-inflammatory programmed cell death associated with various inflammatory conditions. Necroptotic cells release large amounts of inflammatory cytokines and damage-associated molecular patterns (DAMPs), leading to intestinal epithelial defects. Activation of inflammasomes triggers the maturation and release of IL-1β and IL-18, acting as immunomodulators in RIII, mediating the initiation of innate and adaptive immune responses, and resulting in the development of chronic inflammation (Cytlak et al., 2022). Autophagy is a conserved lysosomal degradation process that maintains cellular homeostasis by degrading cytoplasmic components and damaged organelles such as mitochondria (termed mitophagy), thereby reducing ROS levels. Autophagy plays a critical role in maintaining intestinal barrier integrity and regulating apoptosis and necrosis of intestinal epithelial cells (Foerster et al., 2022). However, research also indicates that under conditions of irreparable damage, autophagy can lead to cell death. It has been reported that inhibition of autophagy results in increased ROS in intestinal stem cells (ISCs), thereby impairing intestinal regeneration postradiation (Asano et al., 2017). During the regulation of cellular autophagy, Mammalian target of rapamycin (mTOR) kinase plays a crucial role, with the PI3K/Akt and MAPK/ERK signaling pathways activating mTOR to inhibit autophagy, whereas the AMPK and p53 signaling pathways negatively regulate mTOR to promote autophagy. IR activates PI3K/AKT signaling pathway, thereby promoting mTOR phosphorylation and inhibiting autophagy, leading to compromised intestinal barrier function (Qin et al., 2021).

IR can directly interact with DNA molecules, causing direct DNA damage. It can also interact with water molecules in cells, generating free radicals that subsequently react with DNA. These interactions lead to changes in DNA structure. These irreparable DNA damages further activate pathways for cell apoptosis. IR generates ROS, leading to activation of the NLRP3 signaling pathway, resulting in cell pyroptosis. IR activates the NF-kB signaling pathway, causing inflammation. ROS promotes lipid peroxidation, leading to ferroptosis. IR activates PI3K/AKT signaling pathway, thereby promoting mTOR phosphorylation and inhibiting autophagy. This series of reactions leads to cell death. ROS, reactive oxygen species; SSBs, single-strand breaks; DSBs, double-strand breaks; GSH, glutathione; GPX4, glutathione peroxidase 4; Cyto c, Cytochrome c.
The Disruption of the Intestinal Barrier
The intestine serves as an innate barrier to maintain the balance of the intestinal environment, and radiation therapy can lead to changes in the structure and function of the intestinal epithelial barrier. The innate barrier is divided into three layers. The first barrier is the mucous layer, which contains numerous goblet cells that secrete mucus. The mucous layer, appearing semitransparent, is continuously distributed on the surface of the intestinal mucosa to prevent direct contact of bacteria and viruses with epithelial cells (Birchenough et al., 2015). The second barrier is the tight junctions between intestinal epithelial cells, which form a multiprotein complex composed of transmembrane protein families and membrane-associated protein families, regulating the permeability of ions, nutrients, and water (Okumura & Takeda, 2017). The third barrier is the lamina propria, composed of immune cells, endothelial cells, myofibroblasts, and matrix components. Among these, the intestinal epithelium is crucial for the intestinal barrier, limiting the passage of toxic and infectious molecules from the intestinal lumen and regulating the permeability of ions, nutrients, and water (Garg et al., 2016).
The intestinal epithelium is composed of numerous repetitive crypt–villus units that undergo continuous self-renewal. Villi are covered by a layer of intestinal epithelial cells and an underlying lamina propria, facilitating absorption activities influenced by villus size and density. ISCs serve as the source of intestinal cells, responsible for maintaining epithelial renewal and repair (Lindemans et al., 2015). ISCs are capable of continuously differentiating into various types of cells, including enterocytes, goblet cells, enteroendocrine cells, and Paneth cells. These cells play a crucial role in maintaining the normal function of the intestine. The highly active cell renewal process of ISCs makes intestinal tissue more susceptible to the effects of IR, leading to a wide range of biological effects. Lgr5+ ISCs renew the epithelial layer every 4–5 days through symmetric division and neutral drift, generating transit-amplifying progenitor cells, which subsequently differentiate into absorptive or secretory cells (He et al., 2020). Lgr5+ crypt base columnar cells (CBC cells) in the intestinal epithelium play the role of main stem cells by continuously producing progenitor cells and differentiated cells in the steady-state process. Because they undergo continuous cell division, Lgr5+ CBC cells are highly sensitive to IR and other stresses (Kim et al., 2023), leading to a series of functional impairments after radiation exposure. Although the large intestine and small intestine epithelium have the same Lgr5+ stem cells, which are located at the bottom of the crypt, and the number of stem cells is similar, their radiation sensitivity is quite different. Lgr5+ colonic stem cells can withstand 30 Gy radiation, whereas small intestinal stem cells can only withstand 15 Gy dose (Hua et al., 2017).
If ISCs function normally, they proliferate rapidly, replenishing multiple adjacent crypts and villi after injury (Tirado et al., 2021). However, if ISCs are damaged, on one hand, the missing cells cannot be replenished in time, leading to disruption of intestinal integrity. On the other hand, reduced proliferative activity of ISCs leads to shortened villi, affecting intestinal function. Intestinal epithelial cell death leads to intestinal epithelial damage, characterized by loss of epithelium, decreased crypts, shortened villi, increased bacterial colony counts in mesenteric lymph nodes, and elevated serum concentrations of FITC-dextran, indicating disruption of the intestinal mechanical barrier and intestinal dysfunction (Shim et al., 2017). Research has found that ISCs express IL-33 in response to radiation injury. Adjacent Paneth cells respond to IL-33 by increasing production of Epidermal growth factor (EGF), thereby promoting ISC recovery and epithelial regeneration (Calafiore et al., 2023). In addition, tight junctions between intestinal epithelial cells play an important role in maintaining the integrity of the intestinal barrier, which is altered by radiation, causing changes in intestinal permeability. Tight junctions regulate paracellular permeability of water, ions, and large molecules in neighboring cells (Suzuki, 2020). Under normal conditions, tight junctions seal the gaps between adjacent intestinal epithelial cells, preventing substances such as bacteria and antigens from entering the lamina propria of the intestinal mucosa, thus avoiding abnormal mucosal immune responses. Once tight junctions between intestinal epithelial cells mutate, decrease, or are lost, intercellular permeability increases, allowing bacteria, endotoxins, and large molecules to enter the systemic circulation. Researchers found changes in the levels of claudin-2, claudin-3, claudin-4, claudin-10, Junctional adhesion molecules (JAM) -1, and occludin in the radiation therapy group, disrupting the epithelial barrier and increasing intestinal permeability (Garg et al., 2016; Shim et al., 2017). Apoptosis of cells disrupts the intestinal epithelial barrier. Intestinal epithelial cells serve as a critical barrier between the intestinal environment and the external world. Their integrity is essential for preventing bacteria and harmful substances from entering the body.
The Inflammatory Response
Increasing evidence suggests that pro-inflammatory responses significantly promote the development of RIII. Based on pathological staging, characteristics, and clinical manifestations, RIII is classified into acute and chronic types. Acute injury to the intestinal epithelium is the primary cause of acute radiation enteropathy, whereas chronic radiation enteropathy is primarily caused by damage to vascular endothelium.
Acute radiation enteropathy typically occurs around 2–3 weeks after radiation therapy, and in some individuals, symptoms may appear within hours of treatment. Intestinal mucosal epithelial cell renewal is inhibited, leading to inflammatory reactions, arteriolar wall swelling, occlusion, resulting in intestinal ischemia and mucosal ulceration. Major symptoms include abdominal pain, diarrhea, increased bowel movements, bloody stools, and tenesmus. In severe cases, there may also be water and electrolyte disturbances and circulatory failure. Acute radiation enteropathy is usually self-limiting, and approximately 20% of patients undergoing radiation therapy may require temporary treatment interruption (Dahiya et al., 2022). Chronic radiation enteropathy occurs three months or more after radiotherapy or when symptoms persist beyond three months. It is primarily caused by ischemia of intestinal wall small blood vessels and intestinal wall fibrosis, characterized by vascular sclerosis and progressive intestinal wall fibrosis. Advanced stages can lead to intestinal wall necrosis, ulcers, perforation, fistula formation, intestinal wall fibrosis, and scar formation, further causing peritonitis, intra-abdominal abscess, intestinal stenosis, and obstruction (Loge et al., 2020). Chronic radiation enteropathy significantly impacts patient prognosis, with approximately 12% of patients dying from chronic radiation enteropathy and related complications within five years (Joo et al., 2020). In normal tissues exposed to radiation therapy during cancer treatment, acute immune changes can ultimately lead to chronic inflammation and radiation-induced toxicity, causing organ dysfunction (Cytlak et al., 2022).
ROS is one of the causes of inflammatory reactions (Lavelle & Sokol, 2020). Activation of inflammation promotes the expression of inflammatory-related genes, secretion of inflammatory cytokines and prostaglandin E2, and further activates NF-κB signaling, ultimately stimulating neutrophils and macrophages, increasing intestinal cell permeability, causing tissue congestion, and leading to immune damage and inflammatory necrosis (Zhang et al., 2020). This results in more severe oxidative stress and inflammatory responses (Steinway et al., 2020), which are primary reasons why intestinal inflammation is difficult to alleviate (Fan et al., 2021). Exposure to high doses of IR (over 1 Gy) leads to the release of cellular contents, such as DAMPs. After IR, toll-like receptors (TLR2, TLR4, TLR5, and TLR9) play a central role in the activation of the inflammatory pathway by recognizing DAMPs (Multhoff & Radons, 2012; Yahyapour et al., 2018). TLRs upregulate inflammatory mediators, triggering the secretion of inflammatory cytokines, including IL-1, IL-6, IL-8, TNF, IL-33, and IFN-γ. Zheng et al. (Zheng et al., 2021) found that mice subjected to whole-body irradiation showed decreased survival rates and body weight, increased expression of inflammatory factors in serum, and changes in intestinal flora. Neutrophils are the first white blood cells recruited to inflammation sites to defend against infection or inflammation (Kraus & Gruber, 2021). In recent years, increasing evidence suggests that neutrophil infiltration plays an important role in intestinal inflammation and tumor progression, and excessive recruitment of neutrophils can lead to tissue and organ damage (Chan et al., 2021; Nemeth et al., 2020; Xiong et al., 2021). JingHu et al. (Hu et al., 2022) demonstrated that the expression of CXC chemokine receptor 2 and its ligands increased after irradiation, promoting neutrophil chemotaxis and intestinal damage after irradiation.
Furthermore, DNA damage caused by IR can induce cellular senescence (Wang et al., 2019). The hallmark of this state is changes in cellular metabolism, lysosomal activity, and factor secretion collectively known as the senescence-associated secretory phenotype. A key feature of senescence is low-level chronic inflammation. Following senescence, intestinal epithelial cells, including ISCs, exhibit prominent inflammatory characteristics. Along the crypt–villus axis, different cells present varying inflammatory senescence states. Inflammatory senescence of ISCs is characterized by upregulation of MHC-II expression, thereby enhancing interaction with CD4+ T cells. Organoid studies demonstrate that senescent ISCs are an intrinsic cause of organoid inflammatory senescence, initially marked by open chromatin of inflammation-related genes, which subsequently leads to elevated expression of inflammatory senescence marker genes dependent on STAT1 signaling. Chromatin changes in inflammatory senescent ISCs are propagated through cellular memory, leading to inflammatory senescence (Funk et al., 2023).
Inflammation response is a protective reaction of the body to injury and infection. However, when the inflammation response is excessive or persists, it can lead to damage of cells, tissues, and organs, and even trigger diseases. In general, the inflammation response induced by radiation therapy is achieved through the release of inflammatory cytokines and their destructive effects on the intestinal epithelial barrier.
Dysbiosis of the Intestinal Microbiota
The intestinal microbiota is a microbial community distributed in the cavities and mucosal surfaces of the human gastrointestinal tract. These microbes play crucial roles in nutrient absorption and immune regulation (Singh et al., 2017). The gut microbiota, along with microbiota-derived metabolites such as short-chain fatty acids (SCFAs), regulate host metabolism and immunity while preventing continuous bacterial invasion following damage to the intestinal barrier, thus maintaining internal balance and environmental stability (Guo et al., 2020; Xing et al., 2020). IR can disrupt the normal gut flora, significantly reducing beneficial probiotics such as Lactobacillus and Bifidobacterium, while increasing harmful pathogenic microbes like Clostridium and Enterobacter. This disruption ultimately leads to gut dysbiosis, manifesting in symptoms such as constipation and diarrhea (Jian et al., 2021).
The dysbiosis of intestinal microbiota caused by radiation therapy serves as a trigger in the pathogenesis of RIII (Liu et al., 2024). Following radiation exposure, there is a decrease in beneficial bacteria and an increase in harmful bacteria, rendering the intestinal mucosa more susceptible to radiation-induced damage (Zhao et al., 2023). Zhang et al. (Zhang et al., 2021) found that IR increases the abundance of Shigella and Bacteroides, whose proliferation leads to the disruption of intestinal barrier structure and function, promoting intestinal inflammation, indicating that changes in the intestinal microbiota contribute to RIII. Wang et al. (Wang et al., 2015) demonstrated that the diversity of microbial composition decreases in both radiation-induced diarrhea and nondiarrhea groups, with a significantly greater reduction observed in the diarrhea group. He et al. (He et al., 2023) found a notable decrease of Akkermansia muciniphila in the intestines of mice exposed to abdominal radiation, paralleled by similar reductions in fecal samples from patients receiving abdominal radiotherapy. Administration of A. muciniphila significantly alleviated radiation-induced intestinal damage. Liu et al. (2021) analyzed fecal samples from patients with chronic radiation proctitis (n = 32) and found significantly increased relative abundances of Peptostreptococcaceae, Eubacterium, and Allisonella in patients experiencing rectal bleeding compared with nonbleeding patients. These findings suggest that these bacteria may pose a potential risk for rectal bleeding in patients with radiation proctitis. Changes in gut microbiota are closely associated with RIII and correlate with the onset of pelvic radiation disease symptoms.
Immune Dysregulation
Due to the intestine being one of the crucial immune organs in the human body, it plays a vital role in maintaining immune homeostasis. IR affects the immune system in multiple ways, reflecting the complexity of the immune system itself, which may be influenced by the host immune environment, radiation dosage, and intensity. Radiotherapy can exert immunomodulatory effects on surrounding tissues, forming the basis for distant effects (Cytlak et al., 2022). Radiation therapy has a dual effect of immune stimulation and immune suppression. Radiation induces immune responses through DAMPs and their corresponding pattern recognition receptors. This stimulates the production of type I interferons (IFNs) and IFN-stimulated genes through activation of the cGAS/STING pathway and activates antigen-presenting cells, including dendritic cells and macrophages (Storozynsky & Hitt, 2020). Radiation therapy also suppresses immune responses through upregulation of IFN-mediated immune checkpoint molecules (such as PD-L1) and induction of immunosuppressive populations, including myeloid-derived suppressor cells (Tuomela et al., 2022). Persa et al. (2015) suggested that following radiation therapy at different doses, regulatory T cells (Tregs) increase production of immunosuppressive cytokines such as transforming growth factor β (TGF-β) and interleukin-10 (IL-10). By secreting TGF-β and IL-10, Tregs further enhance the immunosuppressive effects of myeloid-derived suppressor cells, thereby attenuating both innate and adaptive immune responses of lymphocytes (Brandmaier & Formenti, 2020; Wang et al., 2023). In addition, radiation triggers changes in immune cell subsets, thereby reprogramming the immune ecosystem and mediating systemic bystander effects. These radiation-specific immune cells participate in extensive intercellular communication events. Specifically, radiation-specific CD8+ T cells appear to be central to communication and persist in vivo after completion of radiotherapy (Han et al., 2022). Furthermore, radiation can directly kill immune cells, thereby modulating immune responses. In cancer patients undergoing pelvic radiation therapy, B cells are the most sensitive, whereas NK cells are the least sensitive lymphocytes (Louagie et al., 1999). Belka et al. (1999) evaluated lymphocyte subsets after radiation therapy and found that B cells and T cells appeared to be most affected. The recovery rate of CD8+ cells is significantly faster compared with CD4+ cells. Studies have shown that with increasing radiation doses, CD44 on macrophages is activated, providing receptors for macrophage migration inhibitory factor signaling, initiating inflammatory cascades that ultimately lead to cytokine storms (Yuan et al., 2023).
During the process of RIII, the balance of immune cells and immune cell factors is disrupted. A study found that compared with healthy controls and cervical cancer patients without RIII, patients with radiation proctitis had lower levels of CD25 hi Foxp3+ Treg cells. In addition, inflammatory factors associated with Treg cell function, such as CTLA-4, IL-10, and TGF-β, were significantly reduced in patients with RIII. This suggests a negative correlation between the number and function of Treg cells and the risk of RIII. Clinically, the characteristics of Treg cells could be considered to assess the incidence of RIII (Gong et al., 2020). Garg et al. (2010) found that a single dose of 8 Gy gamma radiation delivered to the entire abdomen of mice resulted in a decrease in neutrophils, macrophages, and B and T lymphocyte numbers within 4 h. Fractionated radiation therapy in Wistar rats induced increased expression of IL-1β, TNF-α, MCP-1, and iNOS in the distal colonic mucosa postirradiation. Wang et al. (2022) reported that radiation enhanced the levels of immune-related factors IFN-γ and TGF-β mRNA, while reducing the levels of IL-17 mRNA, indicating that IR damages intestinal immune function, leading to aberrant immune status of the intestinal immune system.
Treatment Methods for RIII
Drug therapy
According to clinical symptoms and pathogenesis of RIII, its pharmaceutical treatments mainly include the following categories.
Anti-inflammatory drugs: Commonly used anti-inflammatory drugs in clinical practice include nonsteroidal anti-inflammatory drugs (sulfasalazine, balsalazide, mesalazine, olsalazine) and corticosteroids (prednisolone, betamethasone, hydrocortisone).
Antibiotics: Radiation-induced damage to the intestinal mucosal barrier may lead to dysbiosis of intestinal flora, altered proportions of bacterial species, and abnormal proliferation of intestinal bacteria, which may be associated with symptoms such as bloating and diarrhea. Targeted antibiotic therapy may be considered in cases of severe bloating and small intestinal bacterial overgrowth (Amieva-Balmori et al., 2020).
Antioxidants: IR can induce the production of a large number of oxygen free radicals, which subsequently cause cellular damage. Tetrahydrobiopterin, an important cofactor in endothelial nitric oxide synthesis, significantly reduces the incidence of vascular damage and ischemia when supplemented, potentially serving as a novel target for preventing RIII (Yan et al., 2020). In addition, antioxidants such as vitamin A, vitamin C, and vitamin E, which can scavenge oxygen free radicals, are also used in the treatment of RIII (Safaei et al., 2018).
Antidiarrheal Treatment: Diarrhea is a primary clinical manifestation of RIII. Loperamide, an opioid receptor agonist, significantly reduces intestinal motility frequency, slows intestinal transit, and increases bile salt absorption. However, its use is limited by abdominal distension and nausea. For refractory pelvic radiation-related diarrhea unresponsive to loperamide, subcutaneous injection of somatostatin analogs such as octreotide may provide better therapeutic outcomes.
Enema: Medications primarily act by locally retaining enemas to ensure sufficient contact with rectal lesions. Commonly used rectal medications include aluminum potassium sulfate, corticosteroids, SCFAs, metronidazole, and compound enema formulations. Aluminum potassium sulfate (Berntsson et al., 2024) can alleviate radiation-induced intestinal inflammation and bleeding, promoting mucosal protection and ulcer healing. SCFAs provide significant short-term relief of rectal bleeding.
Probiotics: Due to prolonged diarrhea in patients with acute radiation enteritis, there is varying degrees of dysbiosis, which exacerbates diarrhea, creating a vicious cycle. Therefore, regulating intestinal microbiota is a crucial step in the treatment of radiation enteritis. Supplementing probiotics during and after radiotherapy helps alleviate diarrhea symptoms. Commonly used probiotics in clinical practice include lactobacilli, bifidobacteria, enterococci, and lactococci. Lacticaseibacillus casei alleviates RIII by enhancing mucosal barrier and reshaping gut microbiota structure and metabolic activity (Hua et al., 2023). Treatment with Lactobacillus acidophilus promotes intestinal organogenesis and budding, maintains stem cell niche, and facilitates recovery of goblet cells in irradiated mice (Sittipo et al., 2020). Zhou et al. (2022) found that bacteroides fragilis strain promoted intestinal crypt proliferation, stem cell regeneration, mucus secretion, and tight junction integrity by upregulating the signal transducer and activator of transcription 3 (STAT3) signaling pathway. In addition, dysbiosis can be restored by fecal microbiota transplantation (FMT) to rebalance intestinal microbiota. Previous studies have shown that FMT effectively alleviates radiation toxicity, improving diarrhea and constipation symptoms in patients with chronic radiation enteropathy (Ding et al., 2020; Xiao et al., 2020).
Traditional Chinese medicine monomers
Traditional Chinese medicine has a certain research foundation in the prevention and treatment of radiation enteropathy. The following is the mechanism of action of Chinese herbal monomers in radiation enteropathy (Table 1).
The Mechanism of Action of Chinese Herbal Monomers in RIII
ROS, reactive oxygen species; MDA, malondialdehyde; SOD, superoxide dismutase; GPx, glutathione peroxidase; CAT, catalase; NQO-1, NADPH quinone oxidoreductase-1.
Currently, there are numerous research reports on the use of Chinese herbal monomers for preventing and treating radiation enteropathy. However, there is a lack of effective treatment strategies in clinical practice, and current research primarily focuses on symptomatic and supportive care. Most studies on Chinese herbal monomers only investigate partial mechanisms, lacking systematic and comprehensive exploration.
Other treatments
Surgical treatment: When necrosis and infection of the rectum cause persistent rectal and anal pain, or severe complications such as uncontrollable rectal bleeding, intestinal obstruction, or radiation-induced rectal fistula, consideration may be given to resection of the diseased bowel segment. Mesenchymal stem cell therapy: Studies have found that extracellular vesicles derived from mesenchymal stem cells suppress inflammation in mice, enhance the expression of stem cell markers, and maintain intestinal epithelial integrity (Yang et al., 2023). Hyperbaric oxygen therapy: Hyperbaric oxygen therapy can deliver sufficient oxygen to reach the sites of radiation injury, aiding in the growth of cells and surrounding capillaries and promoting tissue repair. For radiation enteropathy refractory to medication/endoscopic treatment, hyperbaric oxygen therapy can be considered (Moreira Monteiro et al., 2023). Recent research has proposed a novel intestinal-targeted drug delivery system, including hydrogels, microspheres, and nanoparticles, which prolongs drug residence time in the intestine and offers new therapeutic directions for radiation enteropathy treatment (Liu et al., 2023) (Fig. 3).
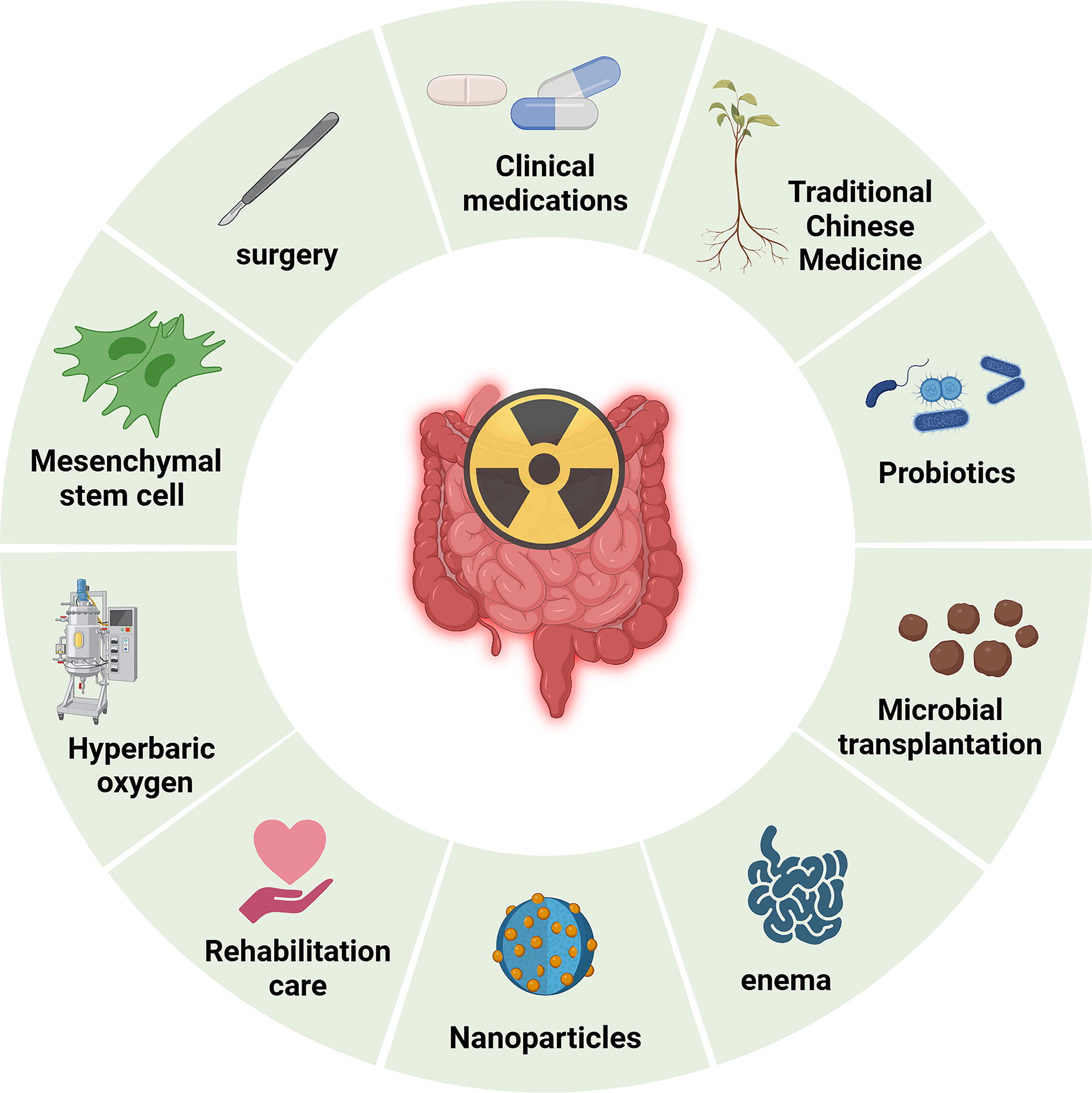
Treatment methods for RIII. RIII, radiation-induced intestinal injury.
Currently, rehabilitation care for RIII faces significant challenges and constitutes a highly complex clinical issue, especially postoperative rehabilitation care for chronic radiation enteropathy. This patient group often experiences a progressive worsening of symptoms, with potential late-stage development of severe complications that profoundly impact physical health and quality of life (Ma et al., 2023). There is a pressing need for personalized management centered around the patient as a whole, with clinical practitioners and nursing teams better positioned to assist and support patients in achieving improved quality of life. However, the primary approach to preventing RIII is through advancements in radiotherapy techniques. Since the turn of the century, radiotherapy technology has made significant strides, with precise radiotherapy techniques such as Intensity-Modulated Radiation Therapy becoming mainstream. This technology offers significant advantages over previous three-dimensional conformal radiotherapy in terms of target area conformity and protection of normal tissues. With the application of new technologies like TOMO and proton therapy, the side effects of radiotherapy can be further reduced. In addition, drugs can be used during radiotherapy for prevention purposes. Radioprotective agents like amifostine can scavenge radiation-induced oxygen free radicals, thereby protecting normal tissues without compromising the efficacy of radiotherapy, serving a preventive role to some extent.
Conclusion
In summary, IR induces and promotes the occurrence of radiation enteritis through various mechanisms, such as generating oxygen free radicals that activate oxidative stress reactions. This process leads to the expression and secretion of multiple cytokines, signaling molecules, and immune-inflammatory responses, disrupting the intestinal epithelial barrier and altering intestinal microbiota balance. During radiotherapy, aside from minimizing the irradiated area of the intestines and enhancing radiotherapy techniques, it is crucial to maintain the integrity of the intestinal mucosal barrier function and preserve the normal intestinal microbiota. These measures are essential for both preventing and treating RIII. Although clinical applications of probiotic preparations, Kangfuxin liquid, intestinal mucosal protectants, anti-inflammatory drugs, traditional Chinese medicine preparations, and other drugs have shown good efficacy in preventing and treating RIII, there is still no standard treatment regimen. Exploring effective medication strategies for the prevention and treatment of radiation enteritis remains an urgent issue, which will have significant implications for improving the quality of life and prognosis of cancer patients.
Footnotes
Acknowledgments
We gratefully acknowledge Dr. Wang for his valuable suggestions and discussions.
Authors’ Contributions
Conceptualization, D.G. and H.W. (Hui Wang); writing—original draft preparation, D.G.; writing—review and editing, D.G. and W.S.; supervision, H.Z. and H.W. (Hui Wang); and project administration, H.Z. and H.W. (Huaqing Wang). All authors have read and agreed to the published version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by the Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-053B), National Natural Science Foundation of China (81573089,81972847), Natural Science Foundation of Tianjin Municipal Science and Technology Commission (21JCYBJC01830), and Tianjin Union Medical Center hospital-level project (2022ZLXK07).