
Abstract
Background and Purpose:
The dilemma in management of the distal ureter and bladder cuff during nephroureterectomy (NU) for transitional-cell carcinoma (TCC) of the upper urinary tract has delayed the development of a completely minimally invasive approach to NU in cases of TCC. Our aim is to present our technique of a purely laparoscopic nephroureterectomy performed entirely through laparoscopic ports, which mimics established principles of open surgical nephroureterectomy with bladder cuff excision. Precluding the needed for patient repositioning, complex endoscopic procedures either before or after nephrectomy and leaving the bladder cuff defect to heal spontaneously.
Patients and Methods:
Patient positioning and trocar arrangement are similar to those of radical nephrectomy. The simple addition of a 5 mm trocar in the lower abdomen (midline or lateral to the rectus muscle, according to patient build) allows the surgeon to adequately dissect the distal ureter, excise an adequate bladder cuff, and suture the bladder defect in a watertight manner without the need for transurethral and intraureteral instrumentation as well as intraoperative repositioning of the patient.
Results:
Eight cases were successfully treated. The operative time ranged from 110 to 200 minutes (mean 157 min). The median time for catheter removal was 7 days; in one patient, catheter removal was delayed to 15 days because of bladder extravasation. Average hospital stay was 10.2 days. During a mean follow-up of 12.1 months, three patients had Ta bladder recurrence, and one patient had local recurrence.
Conclusions:
A complete NU with bladder cuff excision can be accomplished using this approach, with early results comparable to the gold standard of open surgery with the simple addition of a trocar.
Introduction
Patients and Methods
Between January 2006 and October 2008, eight patients underwent NU for upper urinary tract tumors by an experienced surgeon (GJ) using our novel technique. Pertinent patient characteristics are given in Table 1.
Preoperative evaluation and preparation
The diagnosis of upper urinary tract tumors was established by imaging studies—usually a combination of upper urinary tract imaging (renal ultrasonography, helical CT) and retrograde ureteropyelography in conjunction with positive urine cytology. In addition, cystoscopy was performed in all patients to rule out bladder tumors together with retrograde ureteropyelography and barbotage cytology under general anesthesia. In cases of proven upper urinary tract cancer, either by positive cytology or radiologic findings, we proceeded with the surgical approach.
Surgical technique
Patient positioning and trocar arrangement were similar to the standard radical laparoscopic transperitoneal nephrectomy. In all laparoscopic operations, a remote-controlled robotic arm (AESOP1, Computer Motion, Goleta, CA) was used for camera guidance. For laparoscopic dissection, monopolar scissors (Wolf, Knittlingen, Germany) and a harmonic scalpel (Ethicon, Somerville, NJ) were used. Exposure is performed initially by mobilization of the bowel via an incision along the line of Toldt down to the pelvic brim. At this point, further dissection into the pelvis is only possible after insertion of an additional 5-mm trocar, at the lower abdomen, in the midline, or lateral to the rectus muscle (according to patient build) (Fig. 1). This allows the surgeon to change the direction of the camera and working trocars toward the pelvis without the need for patient repositioning. The ureter is then identified, dissected, and clipped at the pelvic brim to prevent tumor seeding into the lower tract during further mobilization of the ureter distally toward the urinary bladder.
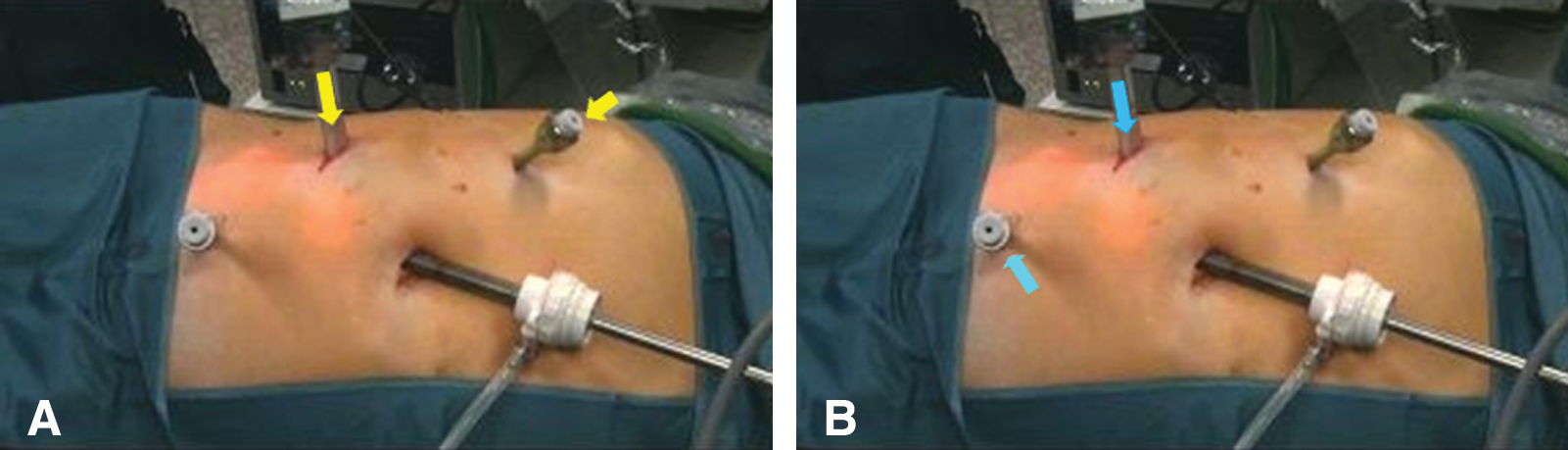
Trocar arrangement. (
After transsection of the medial umbilical ligament, dissection is continued caudally until the detrusor muscle fibers at the ureterovesical junction are identified. The ureter is then retracted cephalic and laterally, tenting the bladder wall at the ureterovesical junction. A 1-cm area of bladder adventitia around the ureterovesical junction is cleared, and a bladder incised longitudinally medial to the insertion of the ipsilateral ureter. An adequate bladder cuff is then excised with visual confirmation of the ipsilateral orifice (Fig. 2). The vesical defect is closed in a running manner using a 3-0, 15-cm polyglactin suture, secured at both ends with absorbable locking clips (Lapra-Ty, Ethicon 2, Cincinnati, OH). The bladder is filled and the repair checked for watertightness.
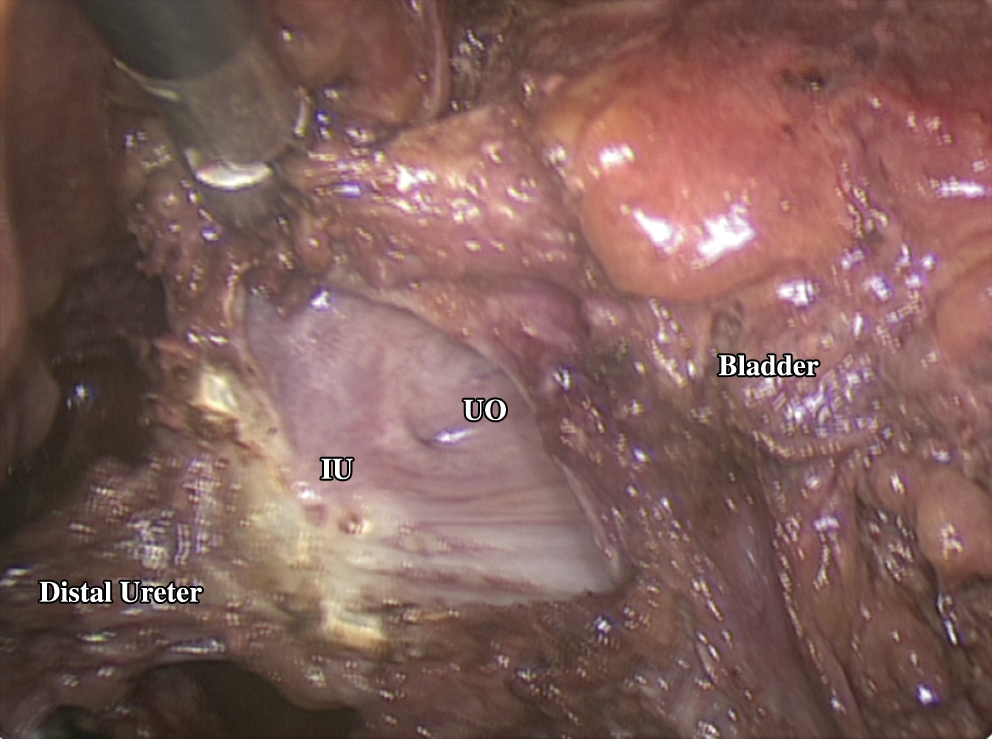
Intraoperative excision of the bladder cuff. IU = intramural ureter; UO = ureteral orifice.
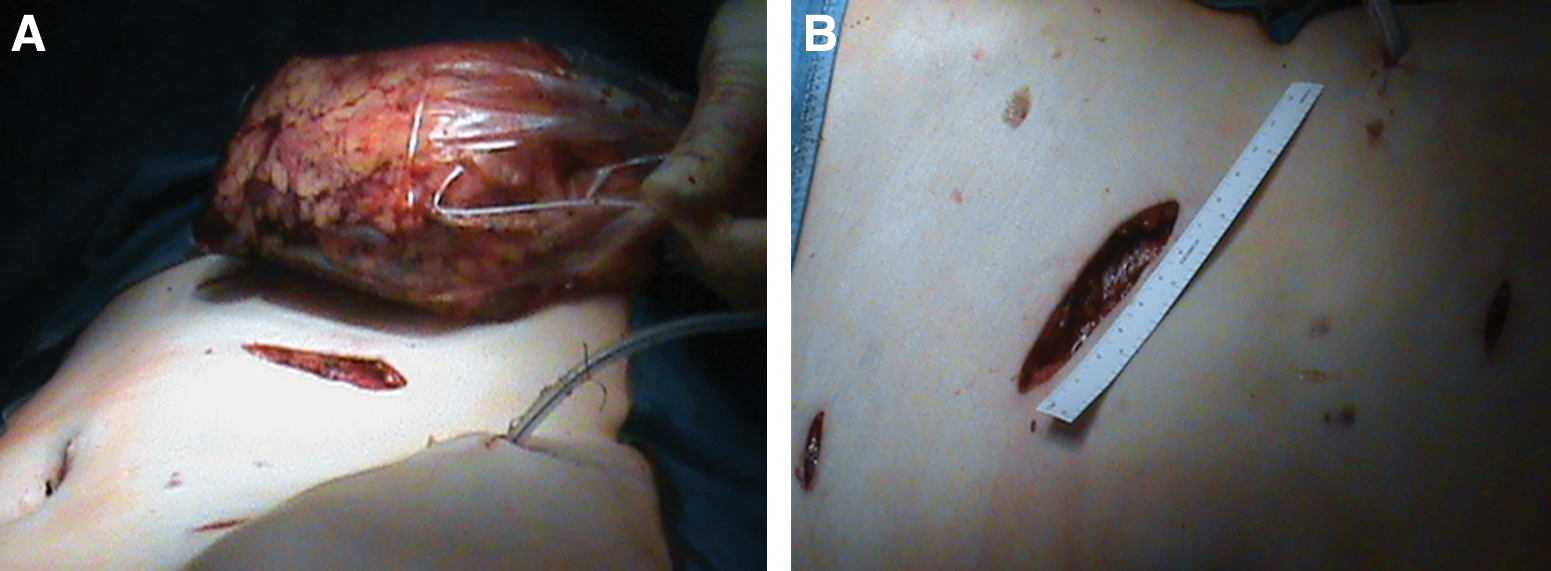
A classic radical laparoscopic transperitoneal nephrectomy is then performed and the entire specimen extracted en bloc within an impermeable organ bag, through a muscle-splitting lower abdominal incision (Figs. 3 and 4). An indwelling 16F Foley catheter is left in place, and a 21F silicone drain is placed laterally to the bladder.
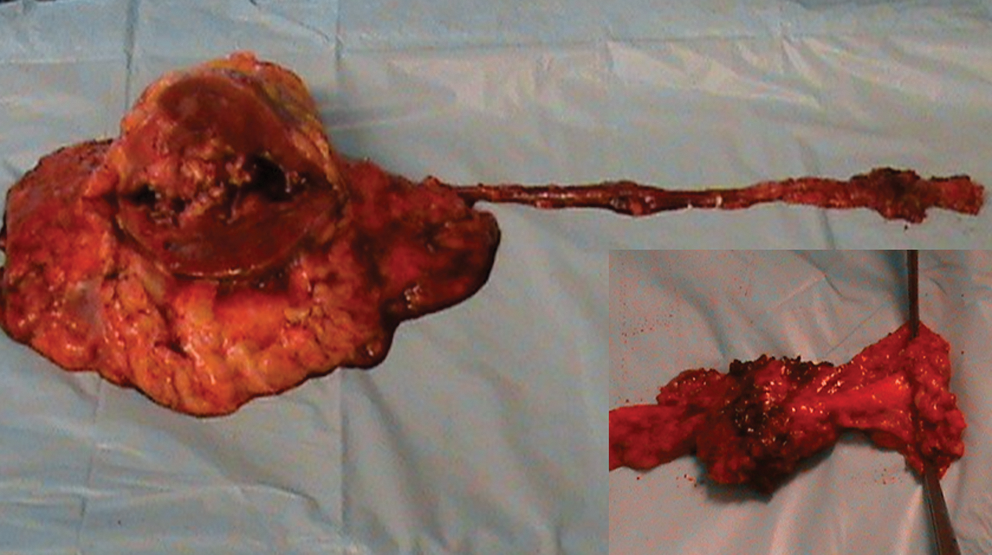
Intact radical nephroureterectomy specimen. Inset: Resected bladder cuff.
(
Postoperative care
All patients were mobilized within 24 hours after surgery, and fluids were given orally and intravenously. On the second postoperative day, wound drainage was removed, and bowel function was stimulated. The 16F Foley bladder catheter was removed a week later if cystography excluded urinary leakage. Data collected for this study included patient sex, age, operative time, postoperative hemoglobin drop, complication rate, and hospitalization time. For evaluation of tumor recurrence, patients were followed every 3 months including physical examination, obtaining complete red blood cell count and serum creatinine value, renal ultrasonography, chest radiography, flexible cystoscopy with urine cytology, and abdominal CT scan at 3, 12, and 24 months postoperatively. In cases of a recurrent bladder tumor, a formal resection was performed with the patient under general anesthesia.
Results
Eight patients (six men, two women; age range: 53–75 years, mean 65.3) with suspected upper-tract tumors underwent surgery using this technique. The operative time ranged between 110 and 200 minutes (mean 157 min). Mean postoperative decrease in hemoglobin was 1.25 mg% (range 0–3 mg%). The tumor was located on the right or left side in four and four patients, respectively. Tumor locations within the urinary tract were: pelvicaliceal, four; upper ureter, one; and lower ureter, one. Multiple locations (two or more) were present in two patients. The tumor type was papillary in five patients, adenocarcinoma in one patient, poorly differentiated in one patient, and sarcomatoid in one patient. Pathologic stages were T1 in three patients, T2 in one, T3 in three, and T4 in one; high-grade tumor was found in two patients and low-grade in six. Pathologic evaluation of the specimen showed a positive margin at the resected end of the ureter in one patient with a pT3, multifocal lesion (pelvis and lower ureter).
Mean hospital stay was 10.2 days; range was 7 to 15 days. One patient had bladder extravasation, which was managed conservatively by prolongation of the urinary catheter up to 2 weeks. This patient had a lower ureteral metastasis, which was associated with severe perivesical adhesions and prevented an adequate bladder cuff excision or closure of the vesical defect. During a mean follow-up of 12.1 months (range 3–18 mos), local recurrence occurred in the patient with positive tumor margins. In three patients, Ta bladder recurrence was detected away from the bladder cuff scar. The ipsilateral ureteral orifice was absent in all patients on control cystoscopy 3 months after the surgery (Table 2).
Discussion
LNU has been established as a safe and reproducible, mini-invasive technique for treating patients with upper-tract TCC in medical centers worldwide. 7 –11 LNU, compared with ONU, has been shown to result in decreased blood loss, postoperative pain, and hospitalization. 3,12 –15 In addition, LNU is associated with a more rapid recovery time and return to normal activities. Oncologic efficacy, in terms of tumor-free margins and short- to intermediate-term recurrence rates, parallels that of the open approach. 12,13 Overall recent data demonstrate that LNU can be feasibly and safely performed, with favorable perioperative outcomes, regardless of the type of laparoscopic approach used. 7,13,16 The technique of distal ureterectomy and bladder cuff excision, however, has not yet been standardized. 7
The five major approaches in current practice include an open technique, a transurethral resection of the ureteral orifice (“pluck” technique), an intussusceptions technique, a transvesical laparoscopic detachment and ligation technique, and laparoscopic stapling of the distal ureter and bladder cuff. 17,18 Each technique has distinct advantages and disadvantages, and differs not only in technical approach, but in the observation of oncologic principles as well.
Stapling approach
A clear advantage to the stapling approach to the distal ureter is the maintaining of a closed urinary system with minimal tumor spillage or urinary extravasation into the retroperitoneum. Some concerning aspects of this approach include difficulty in handling of the laparoscopic stapling device, the need for patient repositioning, the risk of injury to the contralateral ureter, which is not visualized, and the inability to access adequate cuff resection. The most concerning aspect includes the potential for leaving viable urothelial tissue within the staple line. 19 This tissue, in addition to being at risk for tumor recurrence, may not be visible with cystoscopic evaluation. Indeed, a number of authors retrospectively compared various methods of distal ureteral excision and reported a higher incidence of positive surgical margins (up to 25%) and local recurrence (up to 15%) in the pure LNU with laparoscopic stapling cohort. 8,20,21 This highlights the adequacy of this technique in removal of the whole ureter, ipsilateral orifice, and bladder cuff. Stone encrustation on the staple line has also been reported postoperatively. 22,23
Pluck technique
The transurethral resection of the ureteral orifice (pluck technique), although considered a rapid and straightforward technique, has serious drawbacks. Adequacy of this technique is accomplished by deep, thorough resection of the intramural ureter to facilitate its plucking; this could inadvertently lead to leakage of malignant-cell–laden urine from the upper tract into the retroperitoneum and increase the risk of extravesical recurrence, as reported by some authors. 24 –27 With no identifiable mark placed on the resected end of the ureter, the potential for leaving part of the ureter unplucked is also very likely.
Intussusceptions technique
The intussusceptions technique is technically demanding, necessitating extensive transurethral manipulation. Exposure of the bladder mucosa to the ureteral mucosa with potential for tumor seeding as well as inability to close the large bladder defect are some of the drawbacks to this technique. This technique also hinders pathologic evaluation by producing two separate surgical specimens. Moreover, there is no guarantee of adequate excision of the stripped ureter, potentially resulting in tumor recurrence; this makes this technique unlikely to gain universal acceptance after LNU. Laguna and associates 17 in their review found bladder carcinoma recurrence of 19.3% and 24% for ureteral stripping and pluck technique, respectively. The complication rate for endoscopic ureteral removal was 10.3%.
Transvesical laparoscopic detachment and ligation technique
On the other hand, transvesical laparoscopic detachment and ligation technique adheres to the general oncologic principles of intact, en-bloc excision, with controlled occlusion and confirmation of complete excision. Complete excision of the distal ureter and bladder cuff is confirmed by intraoperative visualization of the Endoloop tie, which also minimizes the risk of tumor seeding during renal and ureteral dissection. While this technique has been successful, it has not been readily accepted because of the concerns of additional tumor spillage and urine leakage from the percutaneous bladder port, lengthening the operative time by 60 to 90 minutes, and the steep learning curve.
Open extravesical approach
Finally the open extravesical approach carries a risk of contralateral ureteral orifice compromise, because the contralateral trigone may be inadvertently included in the clamp or suture line. In addition, an open extravesical technique does not necessarily guarantee adequate excision of the entire ureter with bladder cuff, particularly when performed in a blind manner. 28 Although it lacks novelty, the open technique from an oncologic point of view remains one of the most reliable and sound procedures. The optimum technique for management of the distal ureter and bladder cuff excision would be a technique that has the ability to completely remove the distal ureter and adequate bladder cuff with visual confirmation of a resected orifice, minimize tumor extravasation, and allow adequate closure of all bladder openings. Our novel technique fulfills the tenets of this philosophy—first by insertion of an additional trocars, the distal ureter can be clipped early in the procedure, preventing upper-tract seeding. This access also allows excision of the entire distal ureter and bladder cuff laparoscopically without the need for patient repositioning. Visual confirmation of the resected orifice allows excision of an adequate bladder cuff without the risk of injury to the contralateral orifice. Furthermore, the ability to secure the vesical defect in a watertight manner minimizes the risk of urinary extravasation and local recurrence. Finally, the simplicity of the technique precludes the need of a steep learning curve.
We previously published our technique of a modified LNU in which the distal ureter and bladder cuff were excised via an open intravesical approach after a radical laparoscopic nephrectomy and compared with a similar cohort of patients who underwent a classic ONU. The results showed that the modified LNU offered the same cancer control as open procedures with the advantages of laparoscopy and without an increased risk of tumor recurrences. 13 This technique is a mere minimally invasive duplication of the previously mentioned open technique using a smaller incision for extraction of the specimen, with minimal functional trauma to the abdominal wall.
Conclusion
The ultimate goal of minimally invasive techniques is duplication of the standard of care via a minimally invasive approach while still adhering to all the established principles of the procedure. Our technique offers a completely LNU that adheres to oncologic principles without the need for patient repositioning, complex endoscopic procedures either before or after nephrectomy, or leaving the bladder cuff defect to heal spontaneously. Although the technical efficiency and initial results are promising, a larger patient series with long-term results are needed to confirm the oncologic efficacy of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.