
Abstract
Introduction:
Laparoscopic partial nephrectomy (LPN) has not received widespread clinical application because of its technical challenge. Bovine serum albumin glutaraldehyde (BSAG) is a hemostatic agent that is independent of the clotting cascade. We evaluated the use of BSAG as the sole agent for parenchymal and collecting system closure during LPN in a survival porcine model.
Methods:
Eighteen pigs underwent hilar clamping and LPN by longitudinal excision of the lateral one-third of the right kidney. The opened collecting system was covered with oxidized cellulose to prevent BSAG seepage into the urinary tract. BSAG was allowed to set for 10 or 5 minutes. Twelve animals underwent survival LPN BSAG only closure; six control pigs were acutely studied using saline. Urinary extravasation was evaluated by injection of furosemide and indigo carmine, and then evaluating the renal surface and bladder catheter drainage for dye. A subjective bleeding score was assigned after hilum unclamping. At 6 weeks, BSAG kidneys were harvested for burst pressure testing and histopathological analysis.
Results:
All 12 pigs survived for 6 weeks. No pigs had urinary extravasation. Mean percentage of kidney removed by weight was 19%. Mean warm ischemia time was 29 minutes. Five pigs required a second BSAG application to achieve a bleeding score of 0. Mean arterial and collecting system burst pressures were 301.8 and 322.4 mm Hg, respectively. Mean postoperative creatinine increase was 0.07 mg/dL.
Conclusion:
BSAG for completely sutureless LPN in a survival porcine model was feasible.
Introduction
Methods
This study protocol was approved by our Institutional Animal Care and Usage Committee. Eighteen female Yorkshire pigs weighing 25–56 kg were used for this study. The pigs were allowed to acclimate to their pens for 3–5 days before surgery. All animals received preoperative antibiotic prophylaxis with IV enrofloxacin, and had antibiotic coverage for 24 hours after surgery. Baseline serum measurements were drawn to evaluate electrolytes, blood urea nitrogen, creatinine.
Technique of the Deane lateral hemi-nephrectomy
After induction of anesthesia, the animals were secured in left lateral decubitus position. Four laparoscopic 12-mm ports were placed in a typical configuration for renal transperitoneal laparoscopy. The right renal hilum was dissected to expose the renal artery and renal vein. The peritoneum was not reflected off the kidney laterally to hold the kidney in place on the abdominal side wall. The path of the lateral hemi-nephrectomy through the renal capsule was scored using hook cautery. A laparoscopic bulldog clamp was used to clamp the artery first, and then a second bulldog clamped the vein. Warm ischemia time began once the renal artery was clamped. Laparoscopic scissors were then used to excise the lateral one-third to one-half of the kidney (Deane lateral hemi-nephrectomy) making sure to enter the collecting system throughout the length of the kidney (Fig. 1). The opened collecting system was then precisely covered with oxidized cellulose to prevent BSAG seepage. Prior studies have shown BSAG to occlude the collecting system. 7 The cut wound surface was then dried with a gauze sponge in preparation for the BSAG. The excised portion of kidney was removed via a port site for immediate weighing.
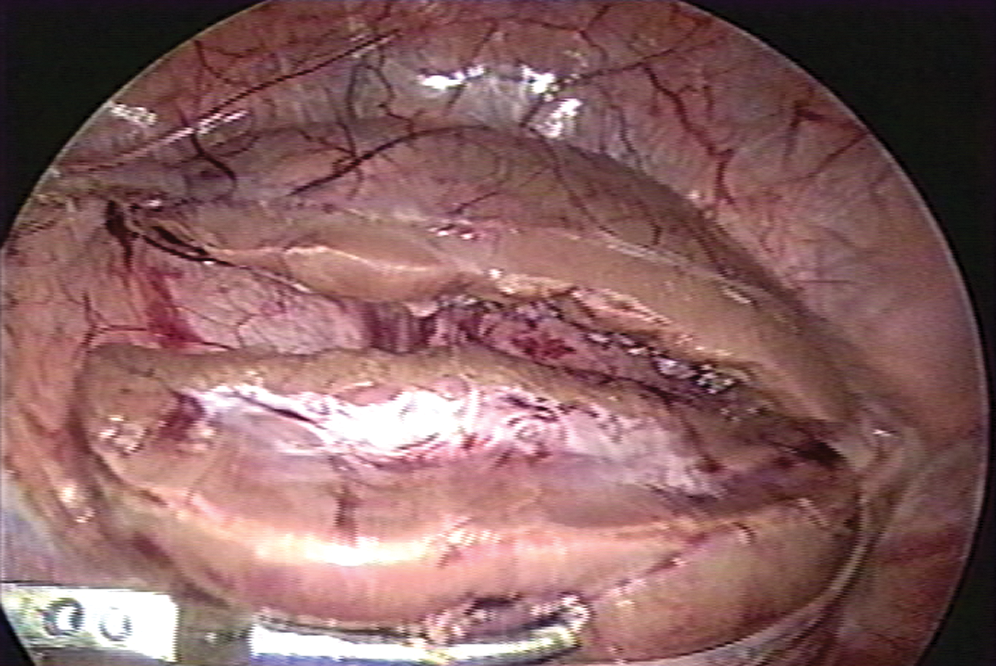
The Deane lateral hemi-nephrectomy. Lateral one-third of the right kidney has been excised to reveal the length of the collecting system and large segmental vessels. Bulldog clamps on renal artery and vein.
Laparoscopic application of BSAG
BSAG is dispensed as a dual syringe cartridge with one syringe containing the bovine serum albumin and the other the glutaraldehyde. The laparoscopic applicator tip consists of a proprietary mixing chamber at the proximal end and tapers to a long plastic tube. Figure 2 shows our modification of the laparoscopic applicator plastic tube to accommodate a fan-like applicator available only to the open BSAG kit. This modified laparoscopic fan applicator allowed for a thin layer of BSAG to be applied. Without this modification, the applicator tip is simply a tube that unevenly drips BSAG onto the wound. The uneven coverage of the wound defect causes more usage of BSAG, increases warm ischemia time, and leads to areas of hemostatic weakness. After covering the defect with BSAG, we waited 10 minutes in the first six animals and 5 minutes in the second six animals for the BSAG cross linking to fully develop or set (manufacturer's recommendation is 2 minutes). The renal vein bulldog clamp was released first. If there was any bleeding with release of the renal artery bulldog clamp, the artery was reclamped and a second layer of BSAG was placed. This reclamp time was then added to the warm ischemia time and another subjective bleeding score was assessed. A subjective bleeding score of 0, 1, 2, and 3 was given after the release of the renal artery bulldog clamp indicating no bleeding, mild, moderate, and severe bleeding, respectively.
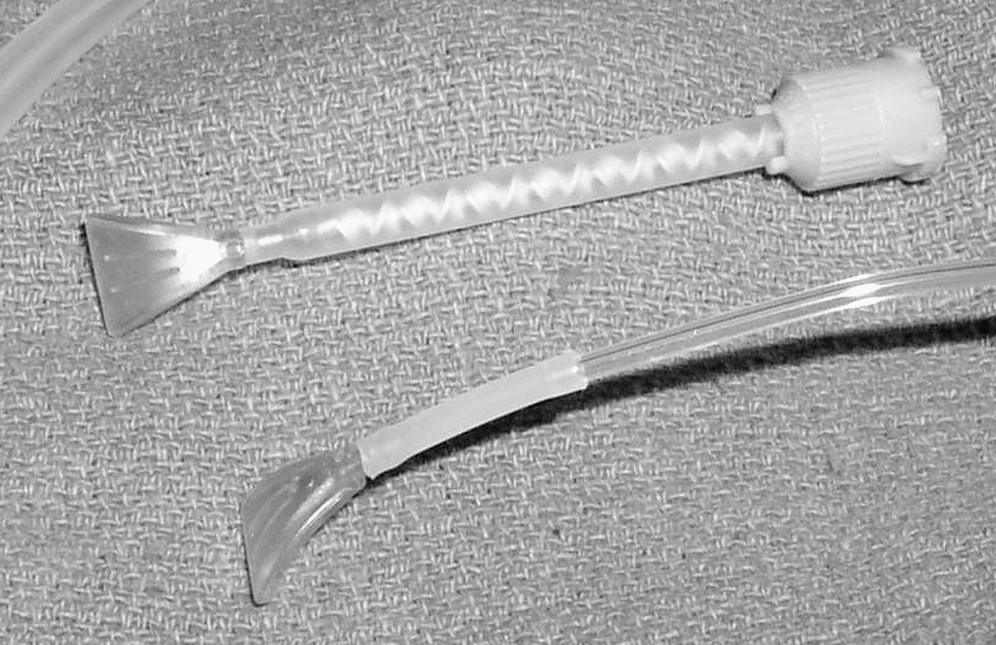
Modification of the laparoscopic applicator. The original fan tip applicator for open surgery is shown at the top with the proprietary mixing tube. We modified our laparoscopic applicator by attaching the fan tip to the original laparoscopic tube tip. The fan tip fits through a 12-mm laparoscopic port.
Control animals
Control pigs were obtained from other acute animal studies not utilizing the kidneys for study. Six pigs underwent the laparoscopic lateral hemi-nephrectomy, but had saline irrigation of the cut wound surface after hilar clamping. Removal of the clamp after 10 minutes of dwell time showed significant persistent hemorrhage. These pigs then underwent eutha-nasia.
Harvest of the BSAG kidneys at 6 weeks
At 6 weeks, the pigs underwent open harvest of the BSAG kidney (Fig. 3). BSAG kidneys were weighed. The ex vivo BSAG kidney then underwent burst pressure testing of the arterial system and collecting system by cannulation of the main renal artery and ureter, respectively, with a 5F open-ended ureteral catheter fixed with silk ties. The burst pressure testing incorporated a constant flow injector (1.5 mL/second) and a 5-bar pressure transducer. The maximum pressure at bursting was automatically recorded by the transducer. After burst pressure testing, the kidneys were sectioned and mounted for histopathological analysis.

Harvested bovine serum albumin glutaraldehyde kidney at 6 weeks. (
Results
All 12 study animals survived for 6 weeks without incident. The six control animals were euthanized at the end of their procedures. Table 1 summarizes the animal and study characteristics and results. Significant differences were seen with the mean weights of the animal (p = 0.01), and of the resected portion of kidney (p = 0.004). The resected portions of kidney increased in size from the 10-minute BSAG set time, the 5-minute BSAG set time, and finally to the 10-minute control animal because of the increasing size of the pig, and the increase in the familiarity of the surgeon performing the lateral hemi-nephrectomy. A second application of BSAG was deemed necessary if there was any ooze from the wound. There was no significant difference in the number of animals requiring a second application of BSAG between the 10 minute (three animals) and 5 minute (two animals). No BSAG animals exhibited urinary extravasation. There were no significant differences seen for the warm ischemia times (p = 0.91), mean arterial burst pressures (p = 0.39), mean collecting system burst pressures (p = 0.82), or BSAG kidney overall preoperative versus postoperative creatinine (p = 0.55). Most notable was that the mean arterial burst pressure and the mean collecting system burst pressure for both the 10-minute and 5-minute set times were all above normal physiologic ranges at the 6-week harvest.
BSAG = bovine serum albumin glutaraldehyde.
Histological analysis showed an intense foreign body giant cell reaction to the glue, dystrophic calcifications, and organizing scar. Gross examination of the specimens at harvest showed a fibrotic pseudocapsule surrounding the BSAG wound. Several animals had adhesions from the retroperitoneum to the bowels; however, there were no signs or symptoms of bowel obstruction.
Discussion
LPN is technically challenging because of the necessity of intracorporeal laparoscopic suturing while under the constraints of warm ischemia. Even in the best of hands, rates of urine leakage and hemorrhage are not negligible. However, large, prospective, long-term studies have shown a clear benefit of nephron-sparing surgery over radical nephrectomy for the preservation of renal function while maintaining oncological equivalence. Laparoscopic nephrectomy has disseminated well within the general urological community, but the challenges of LPN have quelled enthusiasm for the procedure. Despite the development of adjunctive hemostatic agents, none have shown complete hemostasis by themselves. This study examining the use of BSAG as the sole agent for collecting system and renal parenchyma closure shows that this may be feasible.
The use of BSAG in the kidney has been previously studied. Hidas et al 8 compared open sutured partial nephrectomy (n = 143) with sutureless open partial nephrectomy closed with BSAG (n = 31). Specifically, the authors did suture the collecting system and the interior of the defect, but did not close the parenchyma with suture. They found BSAG closure reduced warm ischemia time by 8.8 minutes (17.2 vs. 26 minutes, p = 0.002), mean estimated blood loss by 66.6 mL (45.1 vs. 111.7 mL, p = 0.001), blood transfusions (1 patient vs. 24 patients in the suture group, p = 0.014), and urinary fistula (0 vs. 3 patients). Nadler and coworkers 9 reported eight cases of BSAG as an adjunct for renal parenchyma bleeding after suturing the collecting system for an LPN. The series showed that the use of BSAG was clinically possible; unfortunately, further follow-up was not reported. Recently, Derweesh et al 10 performed sutureless LPN in five pigs. Their procedure was much different than our sutureless procedure. They performed a lower pole heminephrectomy with a bipolar device, used Argon beam to coagulate the cortical parenchyma, used thrombin gelatin matrix, and then covered the entire defect with BSAG. On top of the BSAG this group used bovine pericardial patch to cover the entire wound surface, and then used another BSAG layer to cover the patch. Besides these extra hemostatic steps, they used a novel proprietary laparoscopic applicator that allowed mixing of the bovine serum albumin and glutaraldehyde close to the wound as opposed to the standard laparoscopic applicator, which mixes the material at the syringe level before sending the BSAG down a plastic tube applicator. Our experience showed that the standard laparoscopic applicator was quite difficult to use as the BSAG would start to set within seconds in the plastic tube applicator, and multiple applicators needed to be exchanged for each wound treated. Our study also confirms that the application technique is very important in decreasing the warm ischemia time, minimizing the amount of BSAG needed to cover the defect, and maintaining adequate hemostasis. Once we switched over to our own homemade laparoscopic tip, we decreased the time to apply the BSAG and allowed minimal amounts of BSAG to be applied to the surface, therefore decreasing the amount that was left in the patient. Unfortunately, the proprietary laparoscopic applicator made by CryoLife, Inc., is currently unavailable commercially.
Regarding our decision to use different set times, initially we chose 10 minutes for all the animals based on experience with the product, but as we performed the experiment on the first few animals, it was clear that the BSAG required less time to fully cross-link. In the end, decreasing the set time to 5 minutes did not affect the warm ischemia time, postoperative creatinine, or bleeding score.
One of the concerns of BSAG is seepage into the collecting system causing obstruction. Kim and associates 7 showed that BSAG caused urinary obstruction in the in vivo porcine model if directly injected into the collecting system in 8 of 12 kidneys (66%). For our study, we used small strips of oxidized cellulose (Surgicel®; Ethicon, Somerville, New Jersey) to cover the opened collecting system. We did not believe this would help close the urinary tract, but acted as a convenient method to prevent BSAG from entering the collecting system. No harvested kidneys showed BSAG or oxidized cellulose within the collecting system.
One of the most interesting findings from this study was the great adherence of the native tissues and renal defect to the BSAG on gross inspection. A fibrotic coating had formed across the entire kidney. Whether this was a specific immunogenic response from the pig to the BSAG or whether this occurs in humans as well is unknown. Mean arterial burst pressure and mean collecting system burst pressure for the BSAG kidneys at the 6-week harvest showed supraphysiological holding strength. No urinomas were found during exploratory laparotomy to harvest the kidneys. Some of the animals had small adhesions to the retroperitoneum and to the BSAG-covered kidneys, but there were no bowel obstructions or volvulus seen.
The shortcomings of this study are that no retrograde pyelograms were performed and that the pig kidney has a propensity to resist any traumatic injury. Retrograde pyelograms would be of interest when comparing the preoperative anatomy with the postoperative anatomy after the lateral hemi-nephrectomy. One of the critiques has been whether or not calyces are excluded from the lateral heminephrectomy. Although this scenario is possible for the mid-renal calyces, it is unlikely to occur in the polar calyces, especially the medial calyces. In unpublished results from our laboratory, investigation of another hemostatic agent using this lateral hemi-nephrectomy technique shows that calyces are not excluded by retrograde pyelogram. A postoperative retrograde pyelogram could confirm the lack of urinary extravasation, but after manipulation from the harvest and burst pressure testing, we found that the resultant scarring on the kidney could withstand any physiological pressures. Finally, in regard to using the porcine model as opposed to a calf or dog model, the porcine model has been shown to emulate the anatomy of the human kidney most reliably. The calf model is cost and care prohibitive at our medical campus. The dog model of the kidney provides only a unipapillate collecting system, but the kidney is more sensitive to warm ischemia and hemorrhage according to other animal studies. 11 As such, the dog model would not be appropriate for our proposed entry into the collecting system.
Conclusion
LPN is a challenging procedure because of the necessity of hemostasis, prevention of urine leakage, and oncologic control all within the constraint of warm ischemia time. Our simple two-step (oxidized cellulose and BSAG) closure method is a reproducible, completely sutureless technique to perform LPN. Further clinical studies are currently being established.
Footnotes
Acknowledgment
CryoLife, Inc., for providing Bioglue.®
Disclosure Statement
No competing financial interests exist.