
Abstract
Background and Purpose:
Fluoroscopically guided techniques to access the kidney percutaneously with low exposure to radiation have been used successfully for many years in our training center. The purpose of this study was to analyze the learning process and to establish the number of procedures necessary for a nonexperienced urologist to achieve competence at performing percutaneous renal access.
Materials and Methods:
Eighty-two percutaneous renal accesses in patients with renal stones or ureteropelvic junction obstruction were evaluated. The time needed to perform a correct puncture and the fluoroscopic screening time were recorded for each renal access. Descriptive analysis, analysis of variance, and a Markov chain were used to analyze the results.
Results:
The rate of success increased from 82.5% to 97.6% after the first 40 punctures. Puncture time and fluoroscopy time decreased as the number of procedures increased. Incidence of complications was 30% for the first 20 cases, decreasing to 10% in the next 20 cases and 3.7% in the last 33 cases.
Conclusions:
The fluoroscopy-guided approach used in this study is an effective and reproducible technique. Our analysis revealed that at least 50 procedures are needed to acquire reliable competence in obtaining access to the kidney.
Introduction
Despite the fact that percutaneous nephrolithotomy (PNL) has become an increasingly common intervention for patients with stone diseases, 6 obtaining renal access still represents a challenging step for many urologists. A recent American survey showed that only 11% of all urologists obtain percutaneous access by themselves. 7 Lee and associates 8 reported that only 27% of urologists trained in percutaneous surgery gain their own renal access; the rest require involvement of a second “surgeon,” usually an interventional radiologist. Watterson and colleagues 9 compared access-related complications during PNL when access was obtained by an urologist vs a radiologist. These authors reported that access-related complications were less during urologist-acquired percutaneous access. Furthermore, they found an improvement in stone-free rates (86% vs 61%), explained as an improved placement of primary access by the urologist who is more familiar with the complexities of stone removal and the flexibility to place multiple tracts during surgery in an efficient manner.
Our group recently described a simplified fluoroscopy-guided approach for percutaneous renal access, successfully used in our training center. 10 The aim of this study was to analyze the learning curve of percutaneous renal access in an endourology fellowship program and to establish the number of procedures necessary for certification.
Materials and Methods
A total of 82 percutaneous renal accesses in 62 patients with renal stones or UPJ obstruction were prospectively evaluated in a 12-month period. All patients had undergone PRS performed by an endourology fellow without previous experience in percutaneous surgery, under the guidance of an experienced endourologist. The procedure was performed in 73 consecutive PRSs following our previously published technique. 10 The time needed to perform a correct puncture and the fluoroscopic screening time were recorded for each renal access. Puncture time was defined as the time from the instant of fluoroscopic localization of the renal unit to the moment when urine was obtained through the needle. Those cases in which access into the collecting system was not achieved or when the experienced endourologist (JGA) had to intervene were considered as failed punctures. Transoperative bleeding, renal hematoma, transfusion rate, late bleeding, and lesions to adjacent organs were considered as morbidities related to the puncture, tract creation and maintenance, and nephroscopy manipulation.
For the analysis, morbidities were enclosed in one single variable. The Statistical Package for Social Sciences, version 10.0 (SPSS Inc, Chicago, IL) was used. Descriptive analysis was performed using the chi-square test to establish the relation between variables. Independent-sample t test and one-way analysis of variance was used. Results were expressed as the mean ± standard deviation (SD) with a 95% confidence interval (CI). A P value less than 0.05 was considered statistically significant.
Results
A total of 82 punctures in 73 PRS among a cohort of 62 patients were recorded. Fifty-nine patients underwent PNL and 3 patients had anterograde UPJ incision (one case bilateral). Successful puncture was achieved in 74 cases, which represent a global success rate of 90.2%. Six failed punctures occurred in the lower calix and two in the middle calix. All attempts in the upper-pole calix were successful. The rate of success increased from 82.5% to 97.6% after the first 40 punctures (P = 0.021). Among patients with failed punctures, 50% (4 patients) had some anatomic abnormality (horseshoe kidney in one case, kidney malrotation in two cases, and retrorenal colon in one case).
Mean puncture and fluoroscopy screening times are shown in Table 1. The mean puncture time gradually decreased as the number of procedures increased (Fig. 1). This decrease in puncture time ranged from a mean of 7.67 ± 2.08 minutes (SD, 95% CI) for the first 20 cases to a mean of 4.69 ± 2.87 minutes (SD, 95% CI) for cases 61 to 82 (P = 0.163). This decrease showed statistical significance after the first 60 punctures (P = 0.024). The fluoroscopy time also decreased from a mean of 4.73 ± 2.0 minutes (SD, 95% CI) for the first 20 cases to 1.77 ± 1.31 minutes (SD, 95% CI) (P = 0.007). This decrease achieved statistical significance after 40 punctures (P = 0.029), reaching a plateau. As shown in Fig. 2, no further significant drop in the mean screening time during the next punctures (41–82) was observed (P = 0.431).
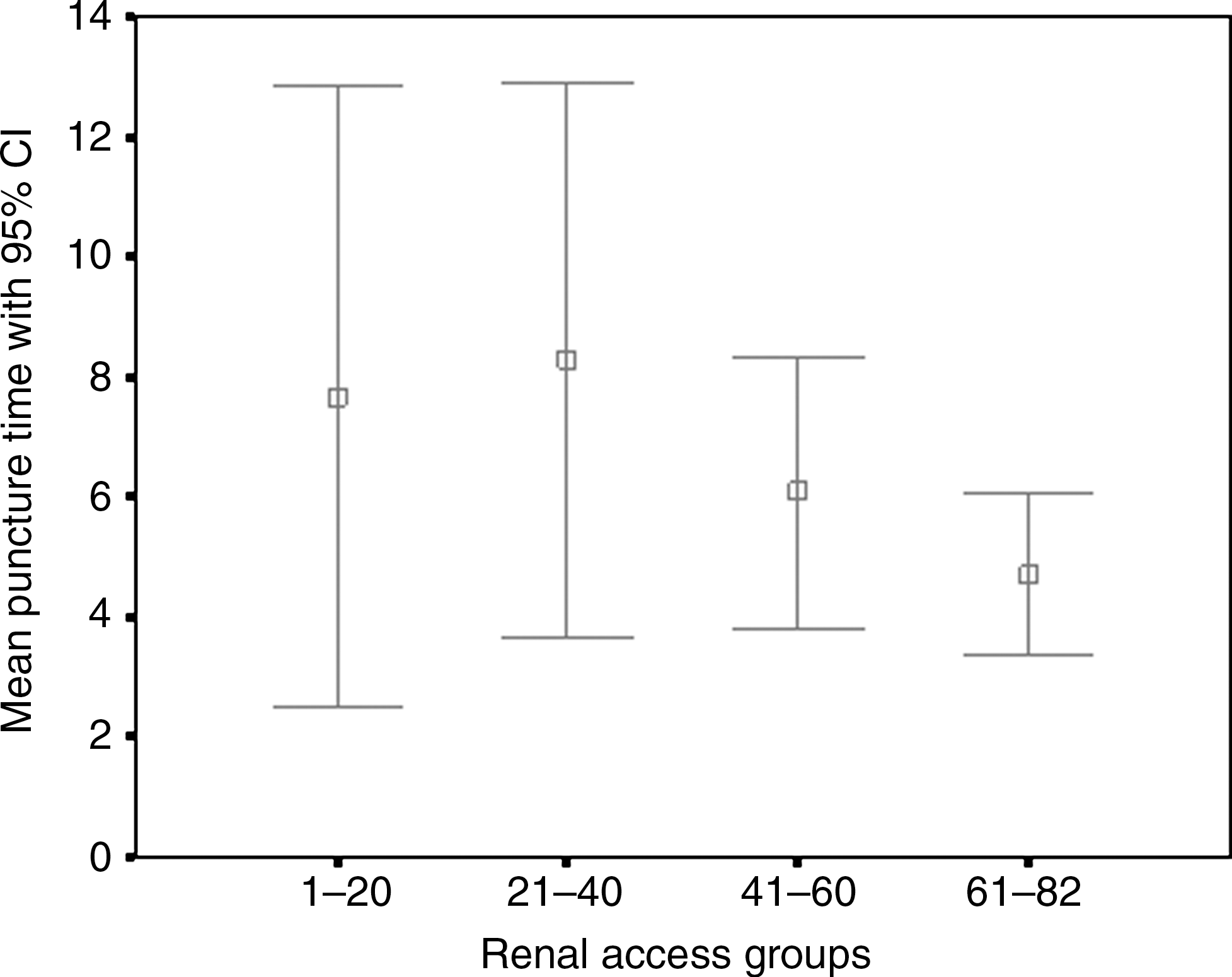
Mean puncture time in minutes (95% confidence interval [CI]). Mean puncture time with 95% CI renal access groups.
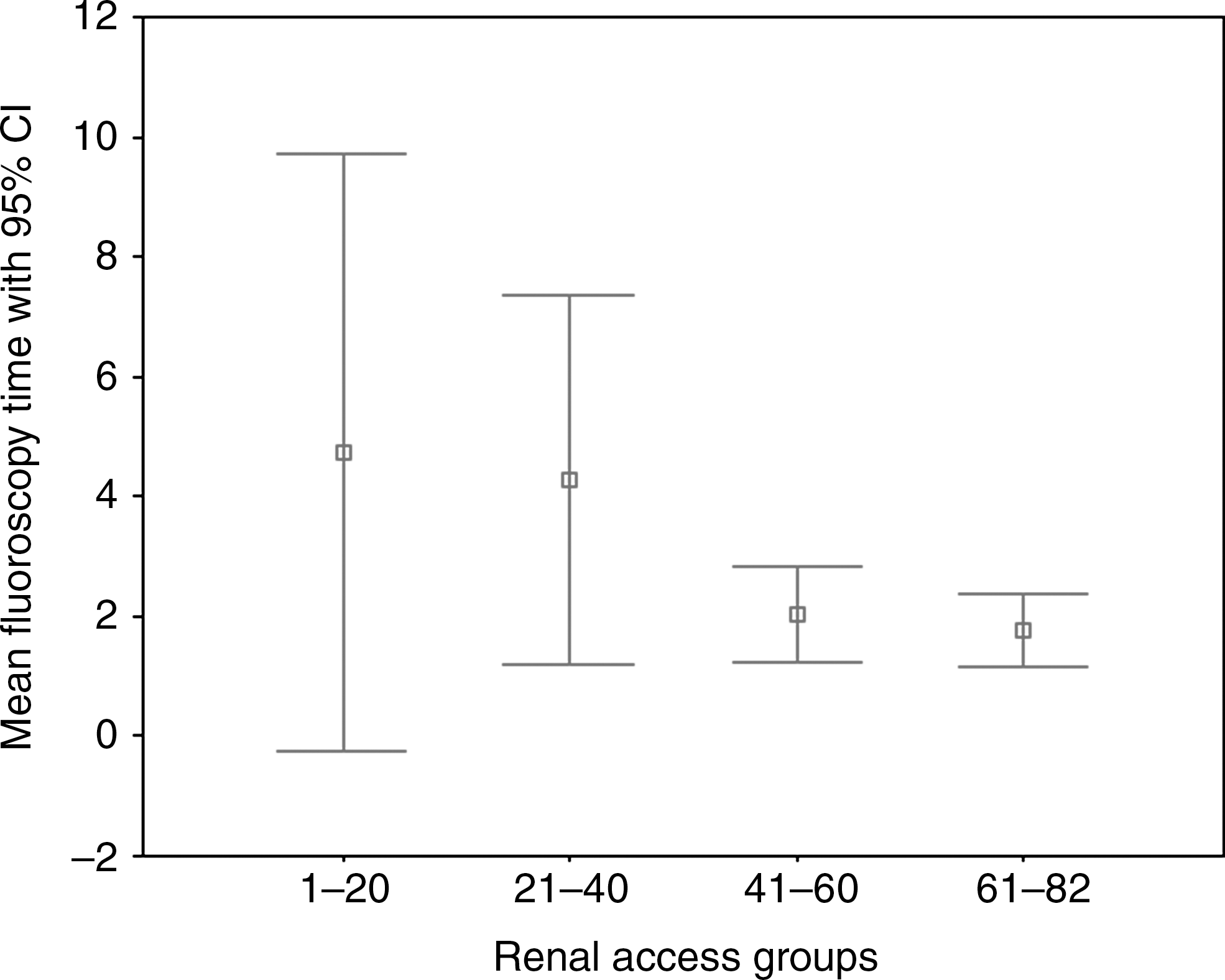
Mean fluoroscopy screening time in minutes (95% confidence interval [CI]). Mean fluoroscopy time with 95% CI renal access groups.
SD = standard deviation.
Time in minutes.
There were 64 lower-pole accesses, 11 middle calix, and 8 punctures with upper-pole access. The mean times registered for access route and groups of punctures did not show statistical significance (Fig. 3). We found 17.6% cases of mild transoperative bleeding; however, none necessitated stopping the procedure. The incidence of renal hematoma, transfusion rate, and late bleeding were 6.8%, 2.7% and 2.7%, respectively. In one case a colonic perforation occurred. The global incidence of complications related to the access tract and nephroscopy manipulation was 30% for the first 20 cases, decreasing to 10% in the next 20 cases and 3.7% in the last 33 cases (P = 0.023).
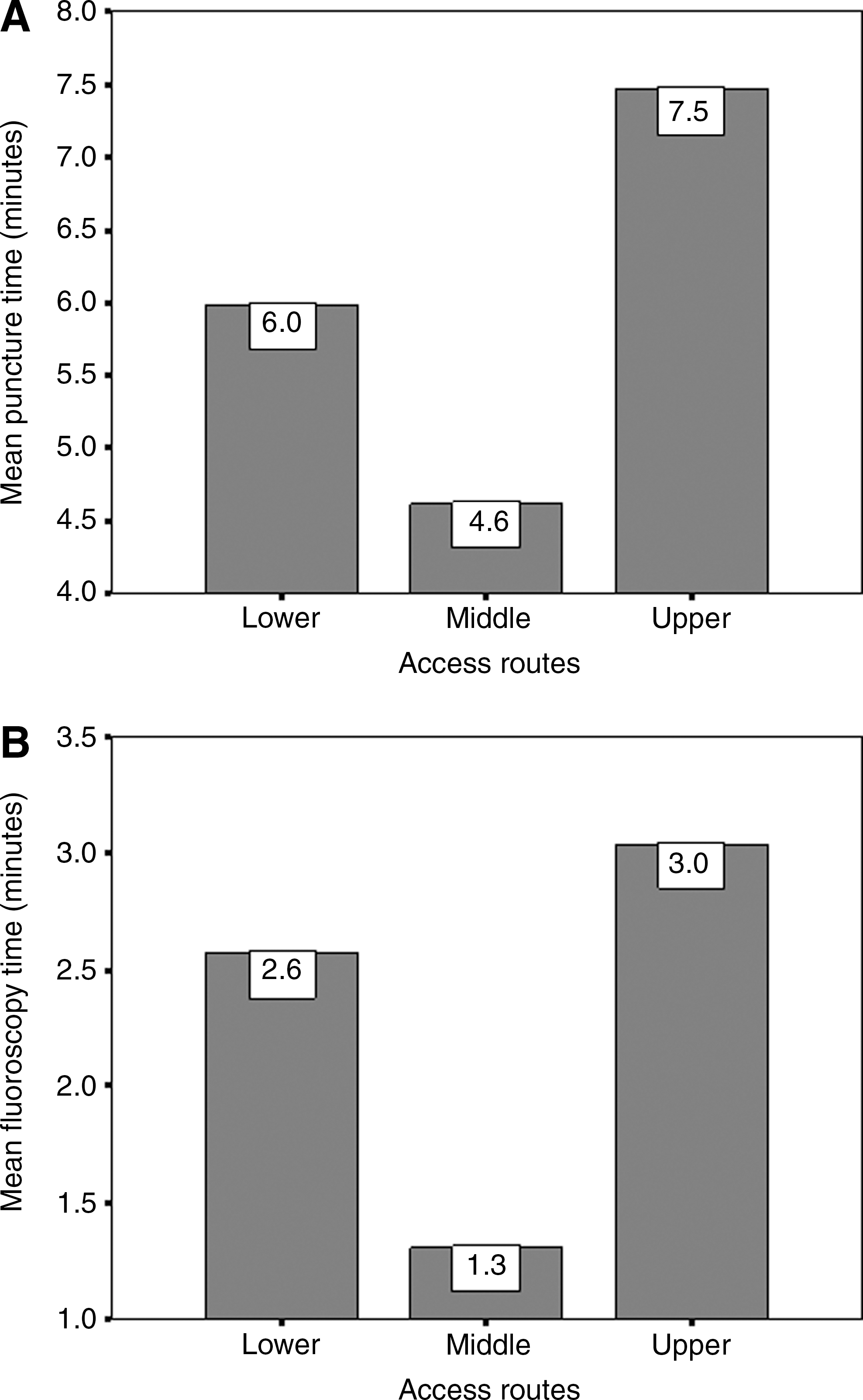
Mean times according to different access routes: (
Defining “1” as a successful puncture and “0” as a failure, the training record can be seen as a Markov chain with the ad hoc defined four states: 11 meaning previous success/current success; 01 meaning previous failure/current success; 10 meaning previous success/current failure; and 00 meaning previous failure/current failure. The transition probabilities estimated considering these four states are shown in Table 2.
1 = successful procedure; 0 = failure.
Transitions matrices were obtained, dividing the training record in periods. An interesting trait shown in Table 2 is that after a training of 82 punctures (total training), the estimated probability of going from success in the past (state 11: previous, current) to success in the future (state 11: current, next) reaches a value around 0.9. The reduction of the estimated probability of going from success in the past (11: previous success, current success) to failure in the future (10: current success, next failure)—ie, 0.31, 0.07, and 0—demonstrates that the fellow is becoming more reliable. From another perspective, Fig. 4 shows that the estimated probability of success (relative frequency of success) is wavering before fulfilling a well-trained status, and that a fellow should not be considered adequately trained after fewer than 50 punctures. Furthermore, there is a statistically significant relationship between the puncture time and the fluoroscopy time (Fig. 5).
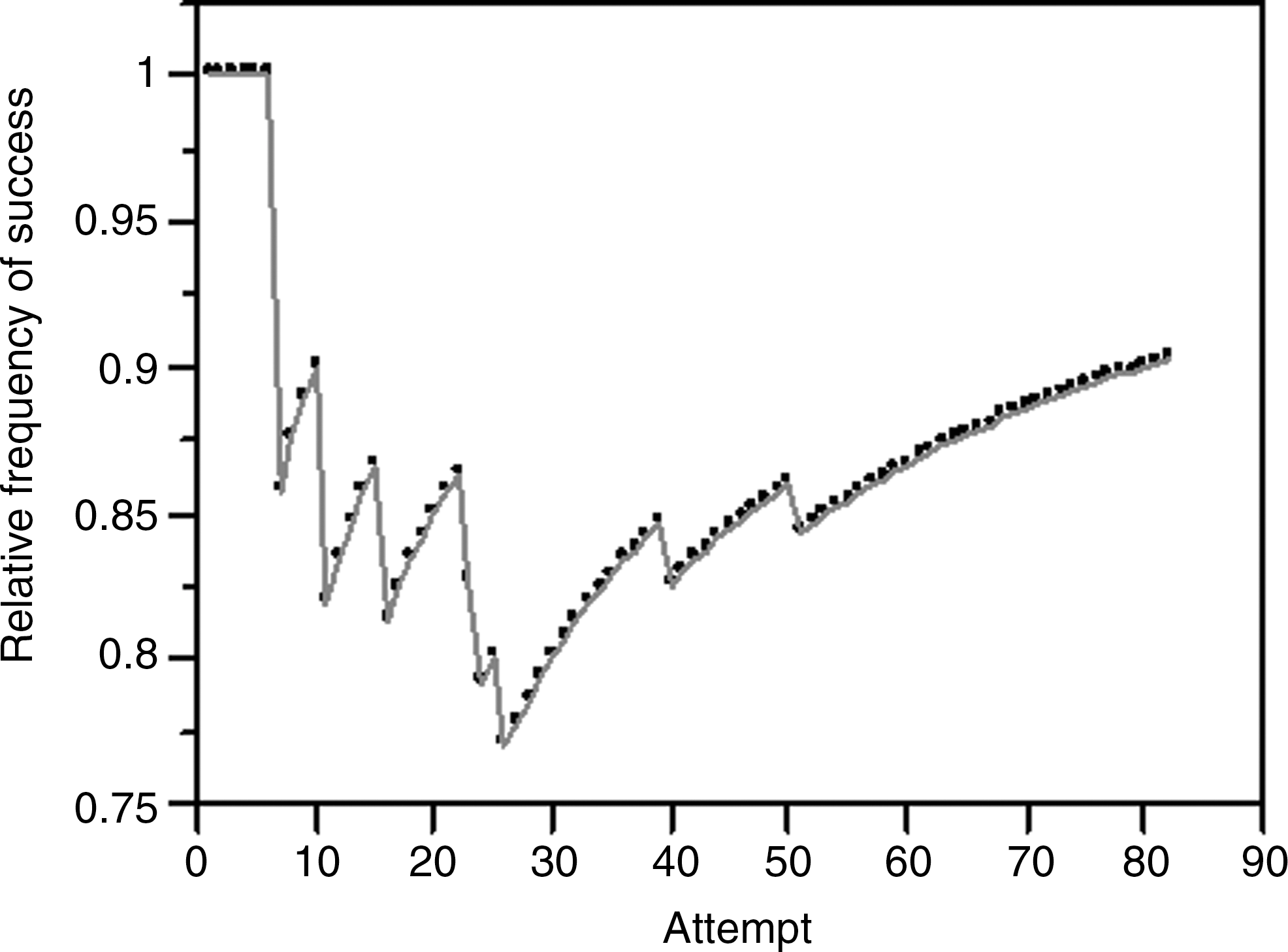
Estimated probability of obtaining a successful percutaneous access as a function of the number of attempts performed by a urologist in training.

Relationship between fluoroscopy time and puncture time.
Discussion
It is important for urologists in training to learn how to perform percutaneous renal access with confidence and a high level of efficacy; however, parameters defined to indicate that a surgeon is well trained in renal access are still needed.
Results reveal that successful punctures increased from 82.5% to 97.6% after the first 40 punctures (P = 0.021). These results are comparable with previous findings. 9,11 As expected, both total puncture time and fluoroscopy screening time gradually decreased throughout the training program. Our analysis shows how a nonexperienced urologist acquires skills as the number of performed punctures increases, supporting previous publications that report the learning curve in percutaneous nephrolithotomy (PCNL). Allen and coworkers 12 suggest that competence at performing PCNL is reached after 60 cases and excellence after 115. Taniverdi and associates 13 also reported that competence in PCNL is obtained after 60 cases.
A Markov chain—ie, a stochastic process—was used to analyze the probability of going from one state in the past (either success or failure) to another state in the future (success or failure). Using this model, future states could be reached through a probabilistic process instead of a deterministic one. We demonstrated that the skill of the surgeon changed its state according to a certain transition probability distribution.
A shortcoming of our study is that the learning process of a single surgeon was analyzed. Further studies to confirm our findings, following the same protocol, are necessary.
Conclusions
According to our results, the simplified fluoroscopy-guided approach used in this study is an effective and reproducible technique that can be taught to nonexperienced urologists. Our analysis revealed that a certified training program should consist of at least 50 percutaneous renal access procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.