
Abstract
Background:
Retroperitoneal and transabdominal laparoscopic access to retroperitoneal organs became the golden standard for treatment of most adrenal and renal diseases. Natural orifice surgery is a promising concept in the evolution of minimal access surgery. The possibility of a natural orifice transluminal endoscopic surgery (NOTES) transvaginal retroperitoneal access to diagnose and perform retroperitoneal surgery was developed in our institution, aiming an alternative natural orifice less-invasive approach.
Methods:
Institutional review board approval was obtained from the institution for clinical transvaginal NOTES. A 67-year-old woman (body mass index = 35.6 kg/m2) found to have a large renal cyst situated in the lower pole with compression symptoms was subjected to the technique. Transvaginal retroperitoneal access was obtained by direct vision open technique, the space was digitally dissected, and a flexible two-channel colonoscope progressed the dissection to the left kidney. The cyst was dissected using endoscopic instruments, and resection was completed with use of two laparoscopic instruments because of peritoneal tear with loss of retropneumoperitoneum.
Results:
NOTES transvaginal retroperitoneoscopy was performed, and anatomical landmarks, such as left ureter, inferior mesenteric artery (IMA), vena cava, and aorta, were identified. Insufflation and orientation were hazardous, because of constitutional fat, and operative time was 210 minutes. Postoperative course was complicated by postoperative face and neck enphysema, which disappeared after few days. Observation was maintained for 4 postoperative days, and the patient was discharged without other complications. Follow-up at 30 days was uneventful.
Conclusion:
This first human procedure using flexible transvaginal retroperitoneoscopy showed feasibility of the access, but inadequate instruments led to technical difficulties for therapeutical purposes. However, the new concept of minimally invasive NOTES retroperitoneoscopy may open new therapeutic indications in clinical practice in the near future.
Introduction
Despite successful clinical applications of transvaginal and transgastric NOTES for abdominal surgery since 2007, 8 –16 natural orifice renal and adrenal surgery was still restricted to experimental animal sets. Transvaginal retroperitoneoscopy was successfully described with survival in swine models, 17 –19 suggesting future applications of this new access for renal and adrenal surgery. A new technique developed in our institution based on prior experimental studies by the group 17 is presented, and the first clinical case of the literature is described.
Materials and Methods
The study was performed at the Department of Surgery and Department of Urology, Hospital Municipal Lourenco Jorge (Rio de Janeiro, Brazil) and was previously approved by the institutional review board committee of the institution for transvaginal natural orifice surgery. The multidisciplinary team was composed of general surgeons, urologists, and endoscopists. The patient signed informed consent and was explained about the novelty, potential risks, and benefits of the procedure, and alternative therapy was offered by laparoscopy or open surgery.
Case report
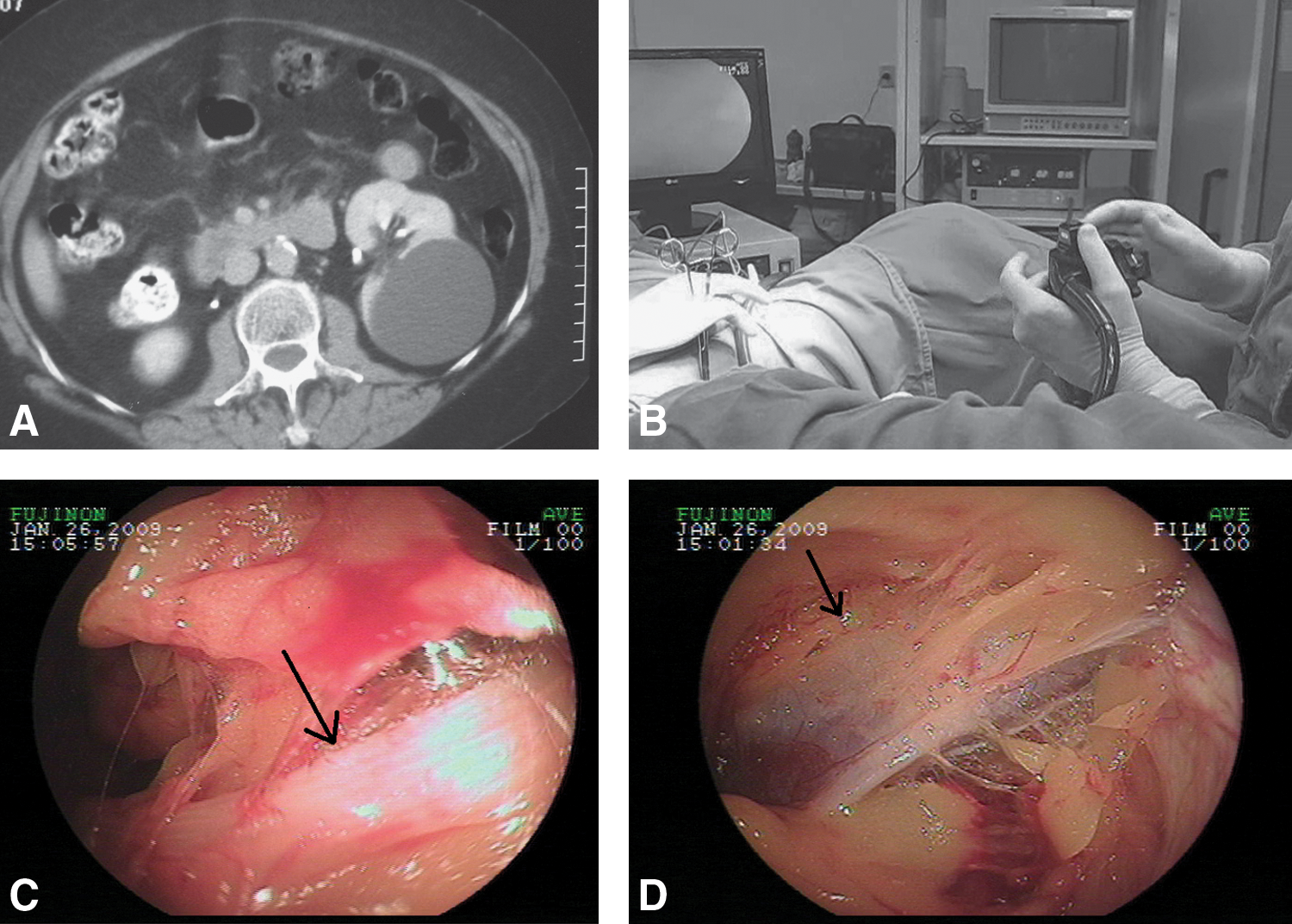
The patient was a 67-year-old woman, with compensated obstructive pulmonary disease, regular use of formoterol and beclometazone, compensated arterial hypertension with regular use of enalapril and diltiazen. Six years before, she had acute cardiac infarction and so had installation of a coronary stent in the anterior descendens artery. Abdominal operations were one cesarean incision and one tubal ligation, both performed more than 15 years before. The patient complained of chronic pain on the left flank for 6 years, and a 4-cm left renal cyst was diagnosed by abdominal ultrasonography, with conservative management. Years later, the patient presented obstructive symptoms for urinary outlet because of a progressive growth of left kidney cystic mass to diameter 9.5 × 8 cm, as measured by computed tomography (Fig. 1A). The patient was classified as American Society of Anesthesiologists II after preoperative clinical evaluation. Her body mass index was 36.8 kg/m2. Preoperative laboratory examinations were negative for renal failure or infection.
(
Surgical technique
Preoperative single-dose antibiotic prophylaxis with 2.0 g cefazolin and 400 mg metronidazol was given to control for vaginal contamination. Endoscopes were disinfected by 2-hour immersion in a peracetic acid solution. Patients were submitted to general anesthesia and were positioned in supine position, legs open, initially in a Trendelenburg inclination. Retroperitoneal insufflation with CO2 was achieved by connecting one of the working channels of the endoscope to a laparoscopic insufflator. Antisepsis was performed with iodopovidone in the anterior abdomen, perineal and vaginal area. The surgeon held the endoscope and positioned it between the legs of the patient, and the first assistant was at his left side, holding instruments for the working channels of the endoscope (Fig. 1B). A second assistant stood on the left side of the patient, for insertion of endoscopic instruments.
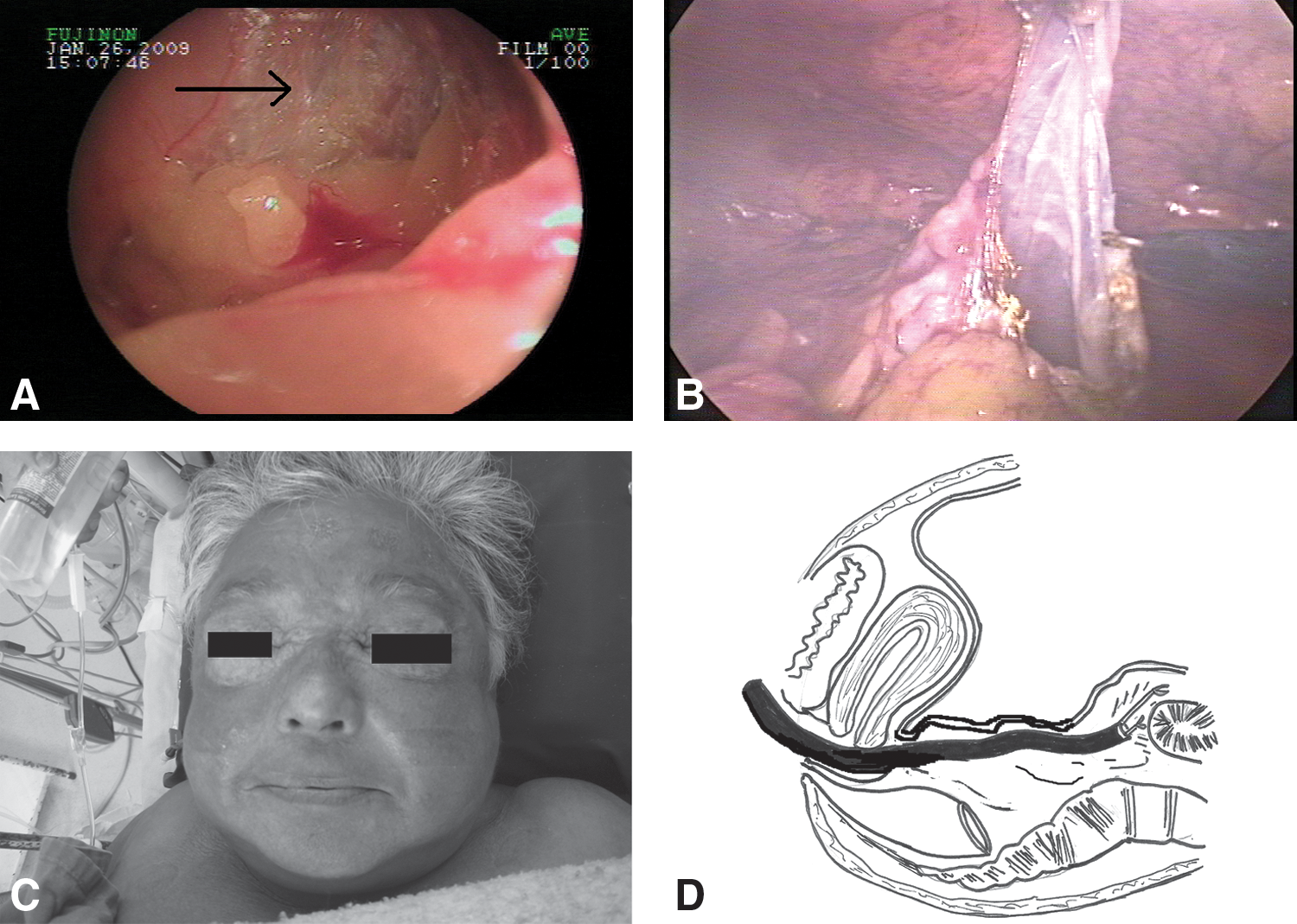
Visualization of uterine cervix was performed using direct view and conventional instruments, by visualization through vaginal speculum and Pozzi grasper retracting the uterus, and safe open access to the retroperitoneal peritoneal cavity was obtained. A full-thickness transversal incision colpotomy was made in the posterior wall of the vagina, 1 cm below the posterior reflection, and the retroperitoneal space was reached, with help of finger dissection in the direction of left retroperitoneal space. A two-channel videocolonoscope FUJINON EC 410-D (Fujinon, Saitama, Japan) was introduced and insufflation using CO2 by a laparoscopic insufflator connected to one working channel of the endoscope allowed blunt dissection of the retroperitoneal space. Retroperitoneal anatomical landmarks, such as inferior vena cava, aorta, iliac vessels, retroperitoneal lymphnodes, left ureter, and inferior mesenteric artery, were recognized (Fig. 1C, D). After sharp opening of left Gerota's fascia using electrocautery by polipectomy snare, using the instrument for dissection and liberation of attachments, dissection of the inferior pole of the left kidney was performed, with identification and dissection of the renal cyst (Fig. 2A). Hemostasis was obtained by monopolar cauterization by endoscopic flexible hot-biopsy forceps and polipectomy snare. At this point, significant leakage of CO2 to the abdominal cavity was noticed, because of a tear in the peritoneum, and final resection of the cyst was performed with the assistance of two laparoscopic 5-mm trocars inserted in the left flank (Fig. 2B), with the insufflation continued to be performed through the endoscope. Complete marsupialization of the cyst was performed by electrocautery, without suturing of the borders. Closure of the entry wound of the vagina was not performed, because retroperitoneal structures are unlikely to herniate through the small orifice.
(
Results
Transvaginal NOTES retroperitoneoscopy was possible using available technology, the identification of retroperitoneal space and digital dissection did not represent technical difficulty, and essential anatomical landmarks were identified. There was no significant bleeding during the procedure and it was estimated to be less than 50 mL. A multidisciplinary team with endoscopists, urologists, and general surgeons was necessary for performing the technique.
Total operative time was 210 minutes, and anesthesiology time was 300 minutes. Colpotomy access time was 8 minutes, and no fascial closure was needed. Intraoperative abdominal pressure oscillated between 12 and 16 mmHg of CO2, because of exposure difficulties in some instances. End-tidal expiratory CO2 ranged from 35 to 40 mmHg.
Postoperative course needed hospital stay observation for 4 days because of study protocol. Immediately after the procedure, the patient presented facial and cervical subcutaneous emphysema (Fig. 2C), and because of previous pulmonary disease the patient stayed in the intensive care unit overnight. Although the patient was hemodynamically stable, SatO2 was 91%, and so oxygen mask therapy, 5 L/minute, was offered during the initial 12 postoperative hours. The therapy was effective, and tracheal intubation was not needed. Postoperative radiology showed a small pneumomediastinum, which disappeared in the next 3 days with conservative management. Postoperative blood laboratory examinations showed no significant decrease in red blood cell values, but a leukocytosis of 12,000 on the second postoperative day. Renal function values were not altered postoperatively. Prophylactic antibiotics were given only at anesthesia induction on the first day and then discontinued. At 30-day follow-up, the patient was asymptomatic, with total regression of the emphysema and good laboratory results. There was no postoperative vaginal discomfort or pain.
Discussion
Retroperitoneal and transabdominal laparoscopic access to retroperitoneal organs became the golden standard for treatment of adrenal and renal diseases. 20 –23 The first laparoscopic nephrectomy was performed by Clayman 24 in 1991, and first laparoscopic adrenalectomy was described by Gagner et al 25 in 1992. In 1992, Gaur 26 described a method for retroperitoneoscopy that allowed the retroperitoneal expansion through a balloon to create an artificial abdominal cavity. In this case, the peritoneal cavity was not penetrated, avoiding manipulation and injury of abdominal organs and enabling rapid return of peristalsis. 27 –30 Despite this refinement and some advantages, retroperitoneal laparoscopy did not gain popularity in the surgical community, because of unfamiliarity to the anatomy and restricted working space.
Natural orifice surgery is a new modification of minimally invasive therapeutic interventions that may evolve into another field of procedures that may improve patient care. The decrease rates of hernias, adhesive disease, wound infections, and other incision-related complications as well as better cosmesis are the proposed potential benefits of NOTES. 4 –7 Preliminary NOTES series in experimental set were reported since 2004 by Kalloo 1 and Kantsevoy 2 (transgastric peritoneoscopy and liver biopsies), and the group of Park performed the first experimental series of transgastric cholecystectomy with survival. 3 Transvesical and transcolonic accesses have been advocated by some researchers as being more suited to access upper abdominal structures which could be more difficult to work with using a transgastric procedure. 31,32 Human NOTES series were first published since 2007 for transvaginal cholecystectomy by our research group, 8,9 and soon NOTES cases were recorded internationally for many indications. 10 –16 Reddy and Rao from India presented successful human transgastric NOTES in surgical meetings in 2005. 33 Since then, various studies are being performed to evaluate the implementation of NOTES techniques. Medical societies and research groups are making efforts to establish ethics and parameters to the process of translating new natural orifice surgery possibilities to clinical practice. 34,35
Vaginal extraction is an alternative to minimize the size of abdominal incisions for female specimen extraction. Gettman et al 36 reported transvaginal laparoscopic nephrectomy in 2002. They used a porcine model to perform six transvaginal nephrectomies in four animals: five using a single laparoscopic port and one was completed entirely transvaginally by using conventional instrumentation. However, they noted that the limitations of laparoscopic instrumentation made the procedure cumbersome and time consuming. Breda et al 37 and Gill et al 38 have also described transvaginal extraction of nephrectomy specimens. Recently, Clayman et al 39 presented their experience associating single-port umbilical and NOTES transvaginal nephrectomy with purpose-built equipment. An alternative to NOTES is single-access surgery that uses articulating laparoscopic instruments. Such instrumentation would obviate the need to space trocars for triangulation, allowing for the creation of a small, solitary portal of entry into the abdomen.
Lima et al, 40 in 2007, assessed the feasibility of combined transgastric and transvesical approach for performing nephrectomy in a nonsurvival study in porcine models, although it is hazardous for removing the specimen with current instruments. In 2008, Isariyawongse et al 41 performed pure NOTES nephrectomy using standard laparoscopic instruments in the porcine model. In their study, transgastric and transvaginal NOTES accesses were easily achieved, and bilateral nephrectomies were performed. In 2007, Branco et al 42 performed a nephrectomy by transvaginal hybrid NOTES using the endoscope through vaginal access and two additional 5-mm trocars in the abdomen. The patient had an uneventful postoperative course and was discharged 12 hours after the procedure. Transvaginal NOTES retroperitoneoscopy was first presented in 2007 by our research group, 17 and experimental access to the adrenal gland and kidney was published by Zacharopoulou et al 18 and Perretta et al, 19 showing feasibility of flexible retroperitoneal NOTES access. However, transvaginal access, orientation, and retroperitoneal dissections are more hazardous in human than swine anatomy.
NOTES transvaginal flexible retroperitoneoscopy in humans has not been described until now in the literature. This study demonstrates the feasibility of the new technique that combines the advantages of retroperitoneal access with natural orifice surgery. In the case reported, the access was easily performed through a direct view incision, retroperitoneal space was entered by digital and endoscopic dissection, and insufflation was reasonable. Although confusion in spatial orientation occurred eventually, anatomical landmarks were identified, and dissection of inferior pole of the kidney was performed, with long operative time. Postoperative complications (subcutaneous and mediastinal emphysema) were possibly due to high-pressure insufflation of CO2 through laparoscopic insufflator inserted in the working channel of the endoscope. At 30-day follow-up, the patient had a good postoperative recovery. In fact, many recent studies have been performed to research the effects of pneumoperitoneum in NOTES, and better ways of insufflation and infection prevention have also been suggested. 43 –46 The insufflation itself should never be provided by the endoscope's insufflation channel, because it provides air instead of CO2, and so there is no possibility of pressure control. However, a better understanding of the physiology of NOTES, specifically retroperitoneal insufflation, is needed to avoid complications such as subcutaneous and mediastinal emphysema as described here.
There are many reasons to stimulate the potential wide use of transvaginal NOTES in current surgery. The access is also known to be safe except few infectious and other complications based on gynecologic surgery done in the past. Transvaginal retroperitoneal NOTES may avoid incision-related complications and uses an approach that possibly eliminates somatic pain. The vaginal access and closure itself can be done easily and fast, with a short learning curve. However, retroperitoneal flexible dissection and progression is hazardous, because of difficulties in insufflation and spatial orientation, with potential dangerous complications related to retroperitoneal emphysema.
This new technique requires further development in the fields of instruments and surgical expertise, before it can be routinely applied to clinical series. NOTES might be a better option to approach the retroperitoneal space. Retroperitoneal natural orifice surgery—NOTES retroperitoneoscopy—may provide additional benefits related to postoperative pain, recovery, and cosmetic results in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.