
Abstract
We describe a case of a splenic injury caused by a transsplenic percutaneous nephrostomy tract. The case was completed without incident and the nephrostomy tube was noted to traverse the spleen on routine postoperative imaging. This rare complication was managed by deposition of Gelfoam® pledgets along the transsplenic nephrostomy tract and placement of a ureteral stent. This novel management technique has not been previously described in the literature and was successful in the conservative treatment of the uncommon complication of splenic injury during percutaneous nephrolithotomy.
Introduction
Splenic injury is a rare but well-recognized complication of percutaneous nephrolithotomy (PCNL). Treatment options for this complication have been described in the literature, and range from observation to splenectomy. Evidence regarding iatrogenic splenic injury supports splenic preservation with either splenorrhaphy or other conservative measures. 1 We describe a case of splenic injury discovered after PCNL, managed conservatively using a novel technique of Gelfoam® (Pfizer, New York, NY) insertion along the transsplenic nephrostomy tract. In addition, we performed a review of the literature to determine risk factors for inadvertent splenic injury as well as approaches to management of this uncommon complication.
Case Report
A 62-year-old man presented with a 1-year history of left flank and back pain. His medical history was remarkable for hypertension and previous myocardial infarction. Computed tomography (CT) revealed an abdominal aortic aneurysm and a partial left-sided staghorn calculus with associated moderate hydronephrosis. The majority of the stone occupied the renal pelvis, measuring 2.7 × 2.1 cm. There were additional stones in the lower pole, the largest measuring 2.0 × 1.0 cm (Fig. 1). He underwent endoluminal repair of his abdominal aortic aneurysm before seeking definitive management of the staghorn calculus. After discussion of treatment options, the patient elected to undergo PCNL.
Left partial staghorn calculus (
Under fluoroscopic guidance, renal access was obtained through an upper pole calix above the 11th rib. A guidewire was passed and several attempts were made to negotiate it down the ureter without success. After these attempts, an Amplatz wire was coiled in the renal pelvis and the nephrostomy tract was balloon dilated to 30F. The PCNL proceeded without complication. At the end of the procedure, a 7F nephroureteral stent was placed. There was no excessive bleeding at the conclusion of the case. Nephrostomy tube placement was confirmed fluoroscopically.
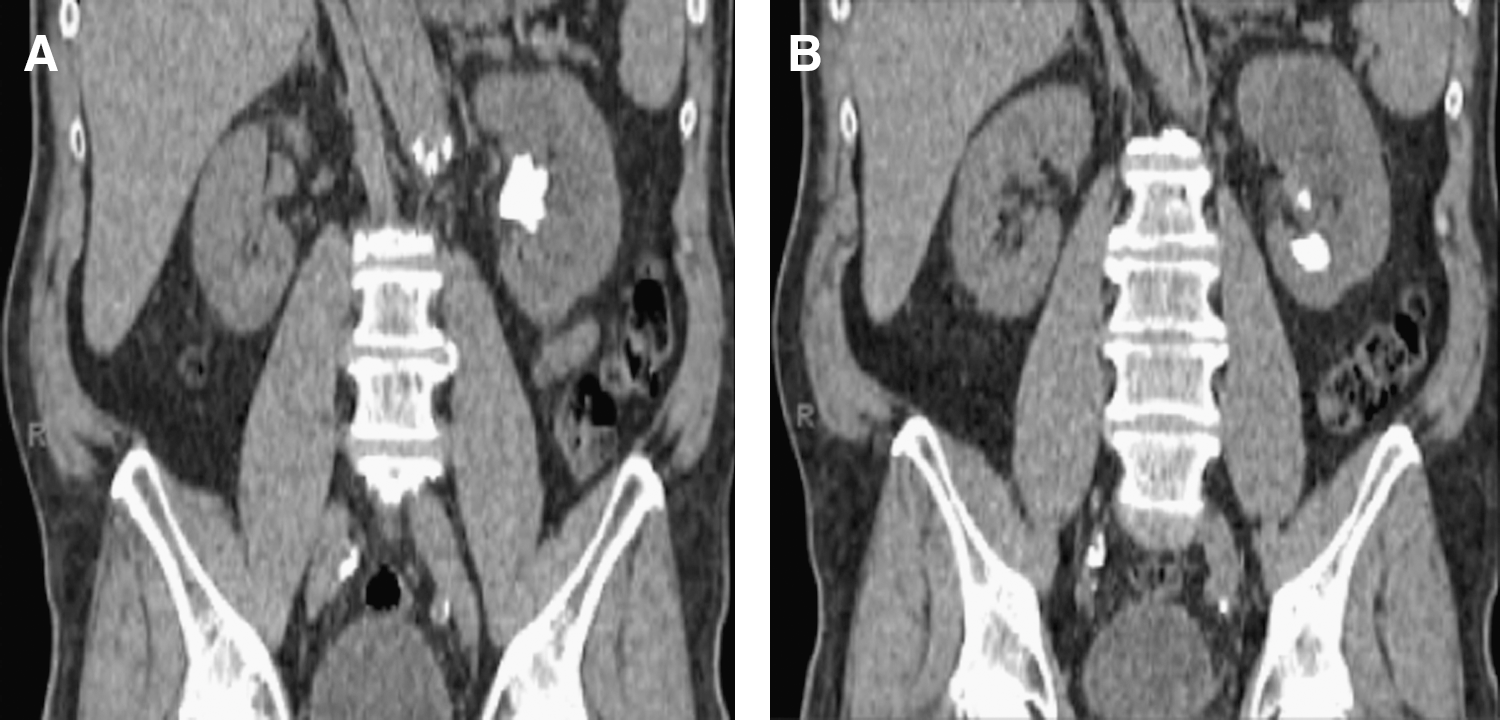
On postoperative day 1, a CT scan was obtained that showed minimal residual stone. The nephrostomy tube was noted to traverse the spleen on its course into the collecting system (Fig. 2). There was no evidence of perisplenic hemorrhage or free fluid in the abdomen. There was no intraperitoneal-free air to suggest associated injury to the stomach or bowel.

Transsplenic percutaneous nephrostomy tube.
The patient did not demonstrate signs of bleeding or hemodynamic instability. However, because of the course of the nephrostomy tube through the spleen, a general surgery consult was obtained; per their recommendations, the patient was placed on bed rest and continuous cardiovascular monitoring. Moderate gross hematuria was noted postoperatively, but the patient's hematocrit level remained stable and blood transfusion was not required.
On postoperative day 2, the patient was taken to the interventional radiology suite for stent internalization and removal of the nephroureteral stent. Specifically, the nephroureteral stent was exchanged for a 9F vascular sheath, and an 8F, 24 cm Double-J ureteral stent was placed over an Amplatz guidewire with the proximal and distal ends coiling in the renal pelvis and bladder, respectively. A sheet of Gelfoam was cut into pieces and rolled into torpedo-shaped pledgets. Approximately five pledgets were deployed along the transsplenic nephrostomy tract under fluoroscopic guidance using the inner dilator to push them through the vascular sheath as the sheath was slowly withdrawn.
The patient remained hemodynamically stable throughout the remainder of hospitalization and did not require blood transfusion. He was kept on bed rest until the hematuria resolved, and was discharged on postoperative day 5. The ureteral stent was removed several weeks postoperatively without incident. CT scan performed 1 month postoperatively showed minimal perinephric stranding and urothelial thickening. The patient did not experience any long-term sequelae or permanent disability as a result of the splenic injury.
Discussion
Risks associated with splenic injury
Iatrogenic splenic injuries are a known complication of left renal surgery. Splenic injury can result in increased operative time and blood loss, as well as a longer period of convalescence. In addition, splenic injury is associated with an increased risk of infection, a near doubling of the rate of morbidity, and increased risk of mortality. 1 Recent trauma literature supports splenic preservation because of the lifetime risk of infectious complications that results from asplenism. 2 –4 Indeed, the syndrome of overwhelming postsplenectomy sepsis is the most serious complication of splenectomy; mortality is associated with splenectomy in 0.026% of adults and 0.052% of children. 5 Prophylactic vaccinations while protective may not offer complete immunity because of both vaccination failure and the presence of other bacteria in at least 50% of overwhelming postsplenectomy sepsis cases. 6
Splenic conservation has been increasingly utilized in both adults and children without adverse outcome. 7 If operative management is warranted, however, most are salvageable by splenorrhaphy or partial resection. 2,4 In cases where additional placement of sutures is not optimal, the use of hemostatic agents such as FloSeal® (Baxter, Deerfield, IL) has been described. 8 In the current case and those of previously described iatrogenic splenic injuries, hemostatic agents have been effectively used.
Hemostatic agents
Hemostatic agents are designed to provide hemostasis by accelerating the blood clotting process. Gelfoam, the hemostatic agent used in this case, is a topical agent consisting of porcine gelatin formed into a sponge that adheres to sites of bleeding. Platelets are trapped in the uniform pores and the clotting cascade is activated. In the case described herein, Gelfoam pledgets were deployed along the previously developed tract allowing adherence to bleeding sites along the tract and activation of the clotting cascade. An internal ureteral stent was also left in place to allow healing of the collecting system. The authors chose Gelfoam because of its ease of deployment through a sheath and proven effectiveness in hemostasis of liver biopsy tracts. 9 The use of this hemostatic agent has also been described for laceration of the right renal artery during PCNL. 10 FloSeal, composed of a gelatin matrix in combination with a thrombin component, would have also been a feasible alternative. The crosslinked gelatin granules in the matrix expand approximately 20% when it comes into contact with bodily fluids, thus slowing the flow of blood. The thrombin component then activates the coagulation cascade. In this case, it would expand to fill the splenic tract upon contact followed by activation of the coagulation cascade and formation of a hemostatic plug. The use of FloSeal has proven effective in managing small-vessel bleeding associated with partial nephrectomies. 11,12
Other hemostatic agents that have been described in urologic surgery include fibrin glue and BioGlue® (CryoLife, Kennesaw, GA). The use of fibrin glue, also known as fibrin sealant, marketed as Tisseel® (Baxter) and Hemaseel™ (Haemacure, Sarasota, FL) has been described in a series of partial nephrectomies after suture ligation of transected vessels. 13 Fibrin glue has also been successfully used for persistent urine leakage after renal reconstruction after a gunshot wound and partial nephrectomies. 14 –16 BioGlue, a liquid adhesive that rapidly polymerizes to form an impermeable seal, has been successfully employed during partial nephrectomy to address minor splenic injuries, including capsular tears and even mild laceration. 17
Preventing splenic injury
Because of the anatomic relationship of the kidney with the colon, duodenum, liver, spleen, and pleura, these structures are at risk for injury during percutaneous renal access. 18 Injuries to the liver and spleen, however, are extremely rare. Liver injuries, in all probability, are not likely a cause of major morbidity as large drainage tubes are routinely placed during biliary procedures. In addition, transhepatic PCNL has been performed intentionally in cases of anatomic aberrancy. 19 Splenic injuries, however, require at the very least conservative management, or possibly splenectomy in the event of significant hemorrhage. Early diagnosis of this complication is critical to prevent adverse outcomes. The possibility of splenic injury should be an immediate consideration in the event of hemodynamic instability after left-sided PCNL, even in patients without significant hematuria.
For PCNL, a supracostal approach is preferred for the treatment of upper pole stones, staghorn or complex calculi, and stones in the proximal ureter 20 ; however, the risk for visceral injury is greater for tracts placed above the 12th rib. To assess the safety of a supracostal approach, Hopper and Yakes evaluated the potential course of a percutaneous access tract on CT scans obtained during full inspiration and expiration, finding that in the prone position, an 11th to 12th intercostal approach would not be expected to puncture the liver or spleen during expiration. However, in 14% and 29% of cases, the tract would be expected to traverse the left and right lung, respectively. A 10th to 11th intercostal approach during expiration was associated with a risk of hepatic and splenic injuries of 14% and 33%, respectively; in addition, the risk of pleural injury increased to a rate of 86% for the left side and 93% for a right-sided puncture. These findings suggested that punctures above the 11th rib carry a low risk of solid organ injury, especially when placement is coupled with expiration. 21
For subcostal punctures, the likelihood of splenic injury is low. The presence of splenomegaly, however, increases the risk of injury. Ultrasound guidance during needle placement significantly reduces the risk of splenic injury. 22 In addition, preoperative cross-sectional imaging with CT or MRI can further clarify structures adjacent to the kidney when a supracostal puncture is planned. 23
In general, the skin incision for puncture should lie between the posterior axillary line and the spine to protect adjacent organs from injury. The puncture site for percutaneous access in thin patients should be more medial and superior. 24 One must also consider the chance for injury related to needle placement along the horizontal axis of the body. A more lateral placement of the catheter increases the possibility of injury to the colon, liver, and spleen. 25,26 Shah and colleagues 27 recommend initial puncture medial to the posterior axillary line during full inspiration to place the kidney in a subcostal location, followed by needle insertion during exhalation to shift the lung and spleen cephalad, thus avoiding the needle path.
Superior pole access was utilized in this case based largely on surgeon preference. Contemporary studies demonstrate improved stone-free rates with a low incidence of pleural injuries with upper pole access. 20,28 As such, we feel that the risk of pleural injury should not impede selection of upper calyceal access if deemed appropriate to maximize stone clearance. Although a multiple-access approach is advocated by some to avoid a supracostal puncture, its use has been found to be associated with an increase in bleeding complications. 28 –31 Both upper pole and multiaccess approaches have been found to be viable with only a small increase in the incidence of acceptable complications. 28
A synchronous bidirectional approach that combines the use of flexible instruments in a retrograde fashion as well as through the nephrostomy tract to avoid multiple percutaneous punctures has also been described. 32 We prefer to use a single-access approach, utilizing the upper pole when necessary, with the liberal use of flexible nephroscopy and retrograde intrarenal surgery to achieve optimal stone-free rates. In general, each case should be individualized; the choice of access, whether single or multiple, should be weighed against potential risks without compromising stone clearance.
Conservative management
Although there are relatively few reports of splenic injury during PCNL in the literature, several case reports have identified spleen-preserving treatment options (Table 1). Conservative management, including observation in a monitored unit and serial measurements of hemoglobin or hematocrit levels, has been described. 10,33
Management of Splenic Injury Detected After Left-Sided Percutaneous Nephrolithotomy
Santiago et al reported a case of small bowel and splenic injury detected on CT obtained for abdominal pain, fever, and postoperative anemia. The patient underwent exploratory laparotomy for the small bowel injury, and the splenic hematoma was confirmed. The splenic injury was managed expectantly. 24 In cases where injury was discovered before nephrostomy tube removal, some authors have left the drainage catheter in place for 12 to 14 days. 33,34 Schaeffer et al 33 reported nephrostomy tube removal followed by observation with serial hemodynamic and hemoglobin measurements for 72 hours, whereas Carey and colleagues 34 removed the nephrostomy tube after a negative antegrade nephrostogram. Shah and associates reported two cases of splenic injury, both requiring exploratory laparotomy; however, only one required splenectomy for ruptured hematoma. In the second case, there was no active bleeding noted intraoperatively and fibrin glue was placed over the laceration. 27 Lastly, splenectomy after PCNL for injuries not amenable to conservative management has been reported because of splenic perforation, ruptured hematoma, and excessive bleeding. 27,35
In the series reported by Schaeffer et al, 33 the greatest degree of blood loss was in the patient whose injury was unrecognized until the time of nephrostomy tube removal; the other two injuries were incidentally detected before nephrostomy tube removal, allowing prolonged catheter drainage, and presumably decreased blood loss. The authors speculated that a postoperative CT scan may be advisable after upper pole puncture to avoid premature nephrostomy tube removal in case of inadvertent injury. Others argue that routine postoperative CT scanning is not cost effective considering the low incidence of visceral injury overall. 27
Although extended nephrostomy tube drainage for transsplenic catheter placement has proven successful, it can be disadvantageous for the patient. Prolonged placement of a nephrostomy tube may be burdensome for the patient in terms of increased postoperative pain as well as the inconvenience of caring for an external drainage device. In the case described herein, this injury was successfully managed without the need for prolonged catheter drainage or blood transfusion. This would undoubtedly improve patient quality of life as well as decrease the risk of problems related to external drains and complications associated with the transfusion of blood products.
Conclusions
Although relatively uncommon, iatrogenic splenic injury is a recognized complication of PCNL. The lifelong risks associated with asplenism suggest that splenic preservation and nonoperative management should be strongly considered for the hemodynamically stable patient. The use of hemostatic agents for splenic injury is expanding, supporting prior reports of success in managing a wide variety of splenic and hepatic injuries. Although it is unclear whether a hemostatic agent was necessary in this case, its use appears prudent when potential bleeding cannot be controlled by other means and when hemostasis is not assured. Prospective studies comparing observation, various hemostatic agents, and nephrostomy tube drainage are lacking, likely because of the exceedingly low incidence of this complication.
Footnotes
Disclosure Statement
No competing financial interests exist.