
Abstract
Purpose:
We evaluated complications of urologic laparoscopic surgery at our institution.
Patients and Methods:
From December 1991 to January 2009, 1017 urologic laparoscopic surgical procedures were performed in Kansai Medical University, including 277 radical prostatectomies, 13 donor nephrectomies, 74 partial nephrectomies, 158 radical nephrectomies, 55 pyeloplasties, 97 nephrouretectomies, 54 simple nephrectomies, 128 adrenalectomies, 34 varicocelectomies, and 127 other procedures. Medical records of each procedure were retrospectively evaluated. The difficulty of each procedure was classified according to the European Scoring System (ESS). Intraoperative and postoperative complications were graded according to the Satava and Clavien classifications, respectively.
Results:
Among the 1017 laparoscopic procedures, 148 complications occurred in 123 patients, resulting in a total complication rate of 14.6%. Conversion to open surgery occurred in 20 (1.9%) patients. Nephrouretectomy had the highest incidence of complications at 23.7%, which was significantly higher than that of other procedures classified as “difficult” group, according to the ESS (P < 0.05). Clavien grades I and II accounted for 73.8% of all the postoperative complications. We experienced one fatality that was caused by air embolism.
Conclusion:
We evaluated the complications of each procedure using the ESS for classification of technical difficulty. Based on the results of our retrospective study, nephrouretectomy should be upgraded as “very difficult” group according to the ESS. Appropriate grading by technical difficulty is beneficial for the prevention of complications from laparoscopic surgery.
Introduction
We studied complications of laparoscopic surgery at our institution and classified the procedures by the degree of technical difficulty according to the European Scoring System (ESS) that was proposed by Guillonneau and associates 5 in 2001. To evaluate the postoperative complications in detail, we used the modified Clavien classification system that was originally proposed by Clavien and colleagues in 1992, and revised and validated by the same group in 2004. 6 We used the Satava classification to evaluate intraoperative complications. 7 We suggest modification to the ESS based on the results of our study.
Patients and Methods
A total of 1017 laparoscopic urologic surgical procedures were performed between December 1991 and January 2009 at the department of urology and andrology, Kansai Medical University, Osaka, Japan. The retrospectively collected data included procedure type and intraoperative and postoperative complications. Cases of open conversion because of technical difficulty were excluded from complications and analyzed separately. The number of each procedure performed is shown in Table 1.
European Scoring System: ED = extremely difficult; VD = very difficult; D = difficult; FD = fairly difficult; SD = slightly difficult; E = easy; Intraop = intraoperative; postop = postoperative; RPLND = retroperitoneal lymph node dissection.
We classified each procedure by the degree of technical difficulty according to the ESS. 5 We used the modified Clavien classification system and the Satava classification system to evaluate postoperative and intraoperative complications, respectively. 6 –8 We classified intraoperative and postoperative complications into major or minor complications. We defined major complications as Satava grade II or higher, and Clavien grade III or higher. We classified the procedures into three groups according to the ESS for technical difficulty. The “easy” group included varicocelectomy, diagnostic examination, and cyst decortication, and the “difficult” group included radical nephrectomy, pyeloplasty, nephrouretectomy, simple nephrectomy, adrenalectomy, sacral colpopexy, pelvic lymph node dissection, ureterolithotomy, orchiectomy, and orchiopexy. The “very difficult” group included radical prostatectomy, retroperitoneal lymph node dissection, donor nephrectomy, and partial nephrectomy. Chi-square analysis was used to compare complication rates among groups with statistical significance at P < 0.05.
Results
Of the 1017 laparoscopic surgical procedures performed at our institution, 148 complications occurred in 123 patients, resulting in a total complication rate of 14.6%. Sixty-three major complications occurred with an incidence of 6.2%, while 85 minor complications also occurred with an incidence of 8.3%. Nephrouretectomy had the highest incidence of complications of 23 (23.7%) in 21 (21.6%) cases. Relatively high complication rates were found for radical nephrectomy (16.4%), radical prostatectomy (15.9%), adrenalectomy (15.6%), and partial nephrectomy (14.8%) (Table 1).
Open conversion occurred in 20 (1.9%) patients, including 9 cases because of complications and 11 cases because of technical difficulty with the procedure (Table 2). Open conversion was performed during radical prostatectomy in two cases, partial nephrectomy in two, radical nephrectomy in two, pyeloplasty in one, nephrouretrectomy in five, simple nephrectomy in two, adrenalectomy in two (Table 1).
RCC = renal-cell carcinoma.
We experienced one fatality (0.09%) that was caused by air embolism during partial nephrectomy. The patient had cardiac arrest immediately after application of fibrin glue using compression air to the parenchymal defect of the tumor bed, which followed excision of the tumor, parenchymal closure using sutures, and declamping of the renal artery. Cardiopulmonary resuscitation resulted in the return of sinus rhythm. Cardiac ultrasonography revealed air bubbles in the heart during resuscitation, and several air bubbles were found in the brain by postoperative CT. The patient died on postoperative day 3. In this fatality in our series, when fibrin glue was applied to the parenchymal defect using compressed air, the renal artery had already been declamped, and the trocars were opened to prevent high intra-abdominal pressure. The intra-abdominal pressure, as recorded by the insufflation machine (UHI-3 Olympus, Tokyo, Japan) was less than 12 mm Hg during the entire procedure.
Postoperative complications classified according to the modified Clavien classification system are shown in Table 3. Grade I complications were recorded in 3.6%, grade II in 4.4%, grade IIIa in 2.3%, grade IIIb in 0.3%, grade IVa in 0.2%, grade IVb in 0%, and grade V in 0.1% of patients. Clavien grades I and II accounted for 73.8% of all postoperative complications. Complications of grade III or higher included 16 cases of urinary retention after a radical prostatectomy that were managed by Foley catheter placement using a flexible cystoscope, and 3 cases of indwelling ureteral stent for urinary leakage after a partial nephrectomy.
See Appendix 1.
RPLND = retroperitoneal lymph node dissection.
Intraoperative complications classified using the Satava classification are shown in Table 4. In 28 (73.7%) cases, intraoperative complications were grade II. The grade III complications were one air embolus, one pleural injury, three tumor injuries, and one rectal injury after a radical prostatectomy, which was diagnosed postoperatively because of an urethrorectal fistula and was managed by total parenteral nutrition.
See Appendix 2.
RPLND = retroperitoneal lymph node dissection.
The complication rates for the easy, difficult, and very difficult groups were 0% (0/57), 13.2% (71/536), and 12.8% (47/367), respectively (Table 5). The complication rate of the easy group was significantly lower than those of the difficult and very difficult groups. The complication rates of the difficult group and very difficult group, however, were not significantly different. Among procedures included in the difficult group, the complication rate of nephrouretectomy was significantly higher than that of other procedures of the difficult group (P < 0.05) (Table 6).
P < 0.05 Chi-square test: Between “easy” and “difficult”, “easy” and “very difficult” is significant difference.
*P < 0.05 Chi-square test.
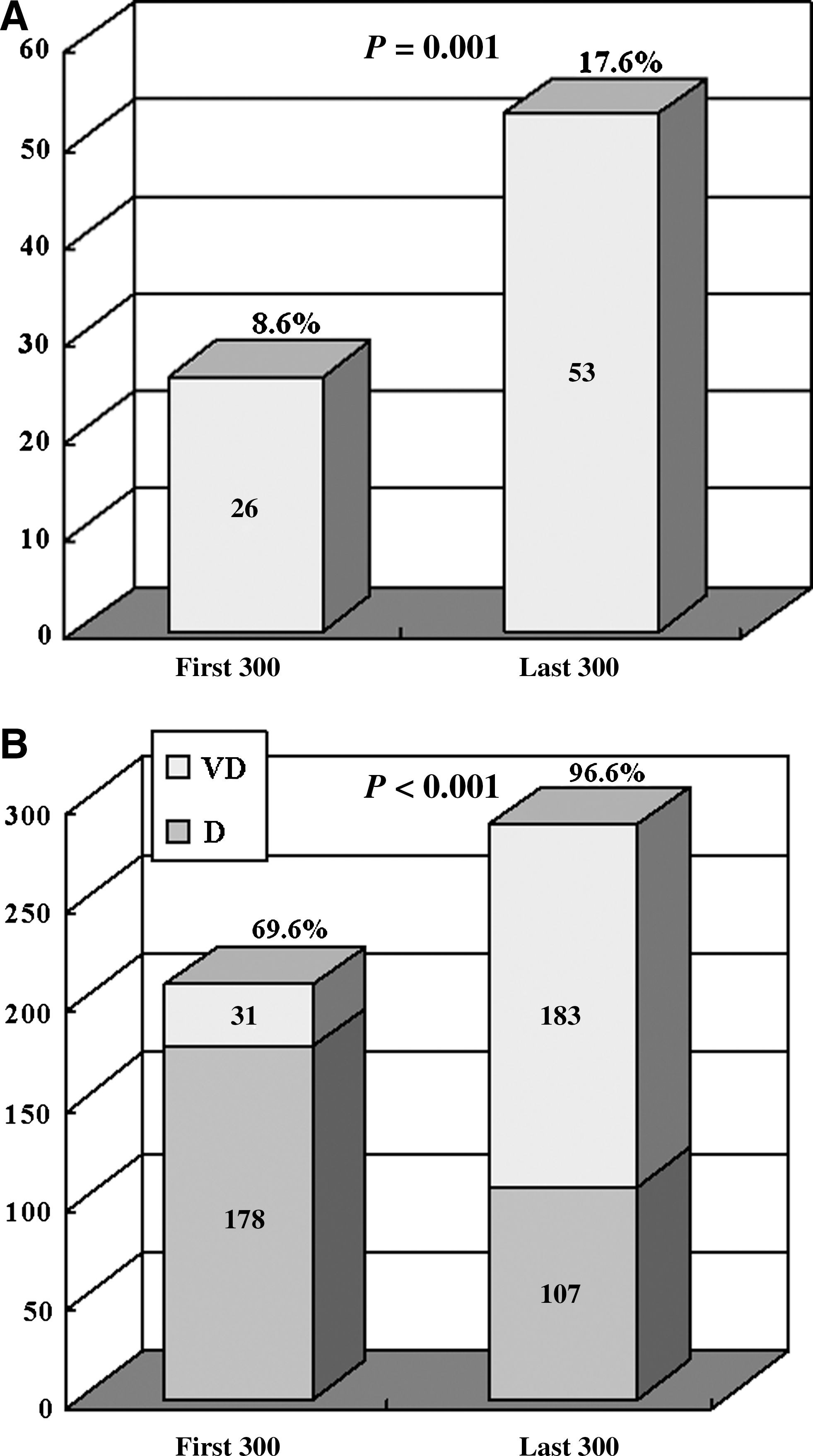
The complication rates in the first and last 300 cases were 8.6% and 17.6%, respectively (P = 0.001) (Fig. 1A). The percentage of procedures of the difficult and very difficult groups in the first and last 300 cases, however, was significantly higher in the latter period (P < 0.001) (Fig. 1B). The procedures designated as difficult or very difficult increased annually (Fig. 2A). On comparing the eras of 1991 to 1999 vs 2000 to 2008, the difficult and very difficult procedures increased from 56.6% to 93.5% (P < 0.001) (Fig. 2B).
(

(
Discussion
Since laparoscopic surgery was introduced to the field of urology in the early 1990s, various complications have been reported. In the present retrospective study, we report a total complication rate of 14.6% and a fatality rate of 0.09%. In 1994, Parra and coworkers 9 reported a total complication rate of 15.2% and no mortality in 217 laparoscopic urologic surgical procedures. In the latest report by Fahlenkamp and associates, 10 the total complication rate in 2407 laparoscopic urologic procedures was 4.4% with a mortality rate of 0.08%, which is comparable to the results for a large series of laparoscopic cholecystectomies with complication rates between 2.5% and 5.0% and a mortality rate of 0.1%. Furthermore, Soulie and colleagues 11 reported a total complication rate of 5.4% and a mortality rate of 0.3% in 350 laparoscopic urologic surgical procedures. The reported mortality rates have remained unchanged since laparoscopic surgery was introduced. It has been shown that the complication rate decreases as surgeons' experience increases.
Rassweiler and coworkers 8 reported a total complication rate of 14% and open conversion rate of 10% in the first 50 cases of 200 laparoscopic urologic surgical procedures. In the last 50 cases, however, the total complication rate was 2% with open conversion rate of 4% by the same surgeon. In the present study, the complication rate was significantly higher in the last 300 cases than in the first 300 cases. We think that the complications in the earlier years were because of a lack of experience and poor technique, whereas the complications in later years were because of technical difficulties of the procedure. The percentage of procedures of the difficult or very difficult groups in the last 300 cases was significantly higher than in the first 300 cases.
The open conversion rate has been reported as 0.5% to 7.0% in urologic laparoscopies. 8 –13 Our open conversion rate was 1.9%. Bleeding caused by vessel injury in six cases and adhesion to the surrounding viscera caused in nine cases represented the major causes of conversion to open surgery in this study. Rassweiler and associates 8 reported that the conversion rate to open surgery was 7.5%, and that the causes were bleeding or hematoma, technical problems such as severe perinephritic adhesions, or renal trauma, complex anatomy, and obesity. There is no consensus on whether open conversions because of technical difficulty should be included as complications.
Permpongkosol and associates 14 simply reported the open conversion rate separate from the complication rate. They did not clarify, however, what percentage of the conversions were caused by intraoperative complications. In contrast, Colombo and colleagues 15 included open conversions as intraoperative complications. We did not include the 11 cases of open conversion because of technical difficulty into the complication rate in this study.
Air embolism is one of the most dangerous complications in laparoscopic surgeries. Several cases have been reported during donor nephrectomies in the literature. 16 Theoretically, an increase in abdominal pressure is translated to an increase in intravenous pressure, resulting in an avoidance of the air embolism even though a venous laceration occurred. Actually, it is recommended that the pneumoperitoneum pressure be raised to 25 mm Hg to slow venous bleeding. 17 The high solubility of CO2 used in laparoscopic surgery also prevents air embolism. If the abdominal pressure is extremely high and the venous wall with a laceration is pulled up simultaneously, however, then a large amount of CO2 will enter the vein, resulting in a gas embolism. The air embolism we experienced during the laparoscopic partial nephrectomy was caused by the direct injection of compressed air into the cut ends of the branches of the renal vein at the renal parenchymal defect. The intra-abdominal pressure, which was monitored and recorded by the insufflation machine, was less than 12 mm Hg during the procedure, including the application of fibrin glue using compressed air. The external committee that reviewed the case concluded that the compressed air entered the vein directly through the venous openings at the parenchymal defect.
Air embolism caused by using an argon beam laser coagulator has been reported in cases of laparoscopic partial splenectomies 18 and open liver biopsies. 19 In those cases, it is hypothesized that the direct injection of gas into the cut ends of the veins resulted in gas embolism. Furthermore, Sezeur and coworkers 18 reported that the principal component of a pneumoperitoneum was not soluble CO2 but insoluble argon after the use of an argon coagulator with trocars opened, resulting in a high risk of gas embolism. From our experience, it is preferable not to use compressed air or an argon beam coagulator on the parenchymal defects of a partial nephrectomy to prevent air embolism.
At present, there is no standardized classification system for urologic laparoscopic procedures according to technical difficulty. In 1999, Fahlenkamp and associates 10 classified urologic procedures according to technical difficulty as easy (diagnosis of and treatment of cryptorchidism, varicocelectomy), difficult (renal cyst resection, lymphocele fenestration, pelvic lymph node dissection, nephropexy, ureteral procedures), and very difficult (nephrectomy, adrenalectomy, retroperitoneal lymph node dissection) and compared the frequency of complications. The complication rates for easy, difficult, and very difficult procedures were 1.0%, 3.9%, and 9.2%, respectively. The complication rate for very difficult procedures was significantly higher than for the other procedures.
We classified the procedures into three groups according to the ESS for laparoscopic urologic surgery, which was proposed by Guillonneau and colleagues 5 in 2001. The ESS classification system is more detailed than other classification systems reported in the literature. Furthermore, experts in urologic laparoscopic surgery have validated this system based on their experience, and data from the international literature are supportive. In our study, the complication rates in the difficult and very difficult groups were not significantly different.
If nephroureterectomy is included in the very difficult group, the complication rate of the very difficult group would be 17.6% and the difficult group would be 14.5%. The difference between these two groups would still not be statistically different. The very difficult group, however, would show a higher complication rate than the difficult group. Among procedures included in the difficult group, the complication rate of nephrouretectomy was significantly higher than that of other procedures (P < 0.05). Nephrouretectomy could be classified in the very difficult group based on the complication rate. Meta-analysis of complications of laparoscopic renal surgery in 2006 showed that the complication rate for nephrouretectomy was 18.8%. 4 Permpongkosol and coworkers 14 have also reported that a complication rate (40.9%) for nephrouretectomy was higher than that of other laparoscopic procedures.
ESS is classified mainly on a subjective scoring of the technical demands, operative risk, and the attention necessary. 5 The complication rate is substantially related to the operative risk and should be one of the factors that affect the technical difficulty. A higher complication rate is also a factor in upgrading the procedure. Colombo and colleagues 15 recommend that the ESS be prospectively and externally validated before widespread implementation.
We also compared the operative time, estimated blood loss (EBL), and blood transfusion rate between radical nephrectomy and nephroureterectomy, which are classified into the difficult procedure according to the ESS. The average operative time, EBL, and transfusion rate in a radical nephrectomy and nephroureterectomy were 305 minutes and 432 minutes (P < 0.001), 174 mL and 355 mL (P = 0.0012), and 5.0% and 8.2% (P = 0.308), respectively. These findings also indicate that nephroureterectomy is more technically demanding than radical nephrectomy. We did not analyze operative time or EBL in this study; these factors are also useful to validate the system.
The modified Clavien classification system for complications has become more widely used recently. This system, however, defines only postoperative complications and cannot be used for intraoperative complications. 20,21 National Cancer Institute Common Toxicity Criteria (NCI-CTC) version 2.0 are also used to evaluate postoperative complications. We used the modified Clavien classification system because it is a more detailed system than NCI-CTC version 2.0. We also used the Satava classification for intraoperative complications. 7,22
We defined the major complications as Satava grade II or higher and Clavien grade III or higher. There is no consensus on how to classify major or minor complications. For example, Permpongkosol and coworkers 14 defined major complications as enough morbidity to necessitate significant additional treatment and at least 2 more days of hospitalization. Bachmann and associates 23 defined that a severe disadvantage for the donor, including conversion, reoperation, transfusion, or effects on graft function were major complications in donor nephrectomy. Donnez and associates 24 defined conversion to laparotomy, hemorrhage necessitating blood transfusion, or a second surgical procedure to perform adequate hemostasis and the repair of urinary tract injuries or bowel perforation as major complications.
Classification systems for intraoperative and postoperative complications are still not unified in the urologic field. Establishment of a classification system for complications in the urologic field is needed for uniform evaluation.
Conclusion
We reported complications in 1017 urologic laparoscopic surgical procedures performed at our institution. The complication rate of nephrouretectomy was significantly higher than that of other procedures in the difficult group. Nephrouretectomy should be classified in the very difficult group of the ESS. Understanding the degree of technical difficulty and the potential complications for each procedure is important to prevent the occurrence of complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
Appendix
| Grade | Definition |
|---|---|
| I | Any deviation from the normal postoperative course without the need for pharmacological or surgical, endoscopic, or radiological intervention |
| II | Minor complications requiring pharmacological treatment, including blood transfusion and total parenteral nutrition |
| III | Requiring surgical, endoscopic or radiological intervention |
| IIIa | Intervention not under general anesthesia |
| IIIb | Intervention under general anesthesia |
| IV | Life-threatening complication (including CNS complication) requiring ICU management |
| IVa | Single organ dysfunction (including dialysis) |
| IVb | Multiorgan dysfunction |
| V | Death of a patient |
CNS = central nervous system; ICU = intensive care unit.
Appendix
| I : | An error without consequence or near miss |
| II : | An error with immediate identification and correction, also referred to as recovery |
| III : | An error that is unrecognized that leads to a significant consequence or complication |