
Abstract
Purpose:
To evaluate our single institution experience with percutaneous cryoablation of renal masses ≥3 cm in diameter for complications and short-term outcomes.
Patients and Methods:
Between March 2003 and February 2009, 108 patients with 110 renal masses ≥3 cm in diameter were treated with percutaneous cryoablation therapy. Technical success of the ablation procedure, complications, and evidence for local tumor recurrence were evaluated for each patient.
Results:
Average maximal renal tumor diameter was 4.1 cm (range 3.0–8.3 cm; standard deviation 1.1 cm). A single cryoablation procedure was performed for treatment of each patient. A technically successful ablation was achieved for 107 of 110 (97%) tumors. The three technical failures all resulted from incomplete cryoablation of the deepest margin of a centrally located renal tumor. A total of 9 severe adverse events occurred in six patients, resulting in an 8% major complication rate. Two patients in whom major complications developed were part of the group of only four patients for whom ablation was performed for tumors > 7 cm in diameter. There were no procedural-related deaths. No evidence for local tumor recurrence was identified in any patients with follow-up contrast-enhanced CT or MRI obtained 3 months or longer from the time of the ablation. Follow-up in these patients averaged 15 months (range 3–42 mos).
Conclusion:
Percutaneous cryoablation of renal masses ≥3 cm in diameter can be performed with high technical success and low complication rates. Extra scrutiny is needed during cryoablation of central renal masses to make sure the ablation zone extends to include the deepest margin of the tumor. Although our experience is limited, percutaneous cryoablation of renal tumors > 7 cm in diameter may be associated with increased complications. The lack of local renal tumor recurrences seen in this study on short-term follow-up is encouraging, but long-term follow-up remains necessary to ensure treatment durability.
Introduction
Percutaneous radiofrequency ablation and cryoablation are two minimally invasive nephron-sparing techniques that are becoming increasingly used treatment options for a selected group of these patients with small renal tumors. This group consists primarily of patients with renal tumors < 3 cm in diameter who have contraindications to surgery because of significant medical comorbidities, patients who have already undergone renal surgery, or patients who have chosen ablation as an alternative to surgery.
The technical feasibility, safety, and short-term efficacy of percutaneous radiofrequency ablation and cryoablation have been well established for management of these small renal tumors. 3 –9 Long-term efficacy has yet to be established in a large study population, but as patient interest and physician acceptance continue to grow, indications for percutaneous thermal ablation are beginning to expand. This includes the increasing number of patients who present for ablation treatment with renal masses ≥3 cm in diameter.
Technically unsuccessful ablations and increased complication rates are possible with ablation of larger renal masses. Evidence for this was recently reported by Lehman and associates, 10 who noted significantly higher complications with laparoscopic cryoablation of renal tumors ≥3 cm in diameter compared with those < 3 cm in diameter. Other investigators have similarly shown that the risk of bleeding correlates with the number of cryoprobes used for the ablation, and therefore the size of the renal tumor treated. 11 Difficulties have also been reported with percutaneous radiofrequency ablation management of renal tumors ≥3 cm in diameter, including lower technical success rates and more than one ablation session frequently necessary to treat the entire tumor. 5,12,13
Percutaneous cryoablation has potential technical and safety advantages for management of renal masses ≥3 cm, which include: (1) The ability to use up to eight cryoprobes simultaneously to generate a large confluent ice ball for management of these larger renal masses, and (2) accurate three-dimensional monitoring of the size and location of the ice ball by noncontrast CT during the procedure to completely treat the target tumor and reduce the risk of injury to adjacent critical structures. For these reasons, we reviewed our experience with percutaneous cryoablation of renal masses ≥3 cm.
Patients and Methods
Approval for this retrospective study was obtained from our Institutional Review Board, and the study was compliant with the Health Insurance Portability and Accountability Act. Informed consent was waived by the IRB. Of 195 patients who underwent percutaneous renal cryoablation at our institution between March 2003 and February 2009, 108 (55%) were treated for renal masses ≥3 cm in diameter. This includes 106 patients with a single renal tumor ≥3 cm in diameter, and two patients who were treated for two renal tumors ≥3 cm in diameter in a single treatment session. These 108 patients constituted our study population, a subset of which had been included in previous publications. 6,14,15
All patients underwent formal consultation in the department of urology before treatment. Primary clinical indications for renal ablation in the study group included contraindication to surgery because of significant medical comorbidities in 62 of 108 (56%) patients, previous surgical intervention to one or both kidneys in 20 (19%) patients, and patient preference in 22 (20%) patients. Less common clinical indications for ablation included patients with von Hippel-Lindau disease and patients with bilateral renal tumors. Tumor characteristics are summarized in Table 1.
SD = standard deviation.
Central renal masses were defined as those extending to, or within, the renal sinus fat. Exophytic renal masses were defined as those with more than 50% of the tumor circumference outside the renal capsule, and intraparenchymal renal masses were those with less than 50% of the tumor circumference outside the renal capsule.
A single cryoablation procedure was performed for treatment of each patient by one of six interventional radiologists with between 3 and 10 years of experience performing percutaneous renal ablations. The cryoablations were performed in a hospital CT suite with the patients under general anesthesia.
Ultrasonographic (Acuson Sequoia, Siemens Medical Solutions, Mountainview, CA) and/or intermittent CT guidance (GE Hispeed CT/i system, GE Healthcare, Chalfont St. Giles, Buckinghamhire, UK), or Somatom Sensation Open 40-MDCT system (Siemens Medical Solutions, Mountainview, CA) was used to place the cryoprobes into the renal mass. Probes were placed with 1.0 to 1.5 cm spacing within the mass in a configuration to achieve a confluent ice ball with at least a 0.5 cm margin around the entire tumor. One or two core biopsies were then obtained from the tumor using an 18-gauge × 2 cm biopsy device (Bard Monopty, CR Bard, Tempe, AZ). Core biopsies were not obtained in a few cases in which the renal tumor became obscured by the cryoprobes. Ablation was performed regardless of biopsy result, because it is often difficult to completely exclude malignancy with core biopsy. 16
In cases in which the bowel was within 1 to 2 cm of the target tumor, hydrodisplacement was used to move the colon or small bowel a safe distance away from the expected ablation zone (Fig. 1). This was performed by infusing sterile saline through a 19-gauge needle placed between the bowel and the renal mass using ultrasonography and/or CT guidance. 17 If the tumor was within 1 to 2 cm of the ureter, a 5F temporary externalized ureteral stent and a Foley catheter were placed before the ablation procedure. Retrograde pyeloperfusion was then performed with room temperature sterile saline during the ablation using a method similar to that shown to be protective to the ureter during renal radiofrequency ablation. 18
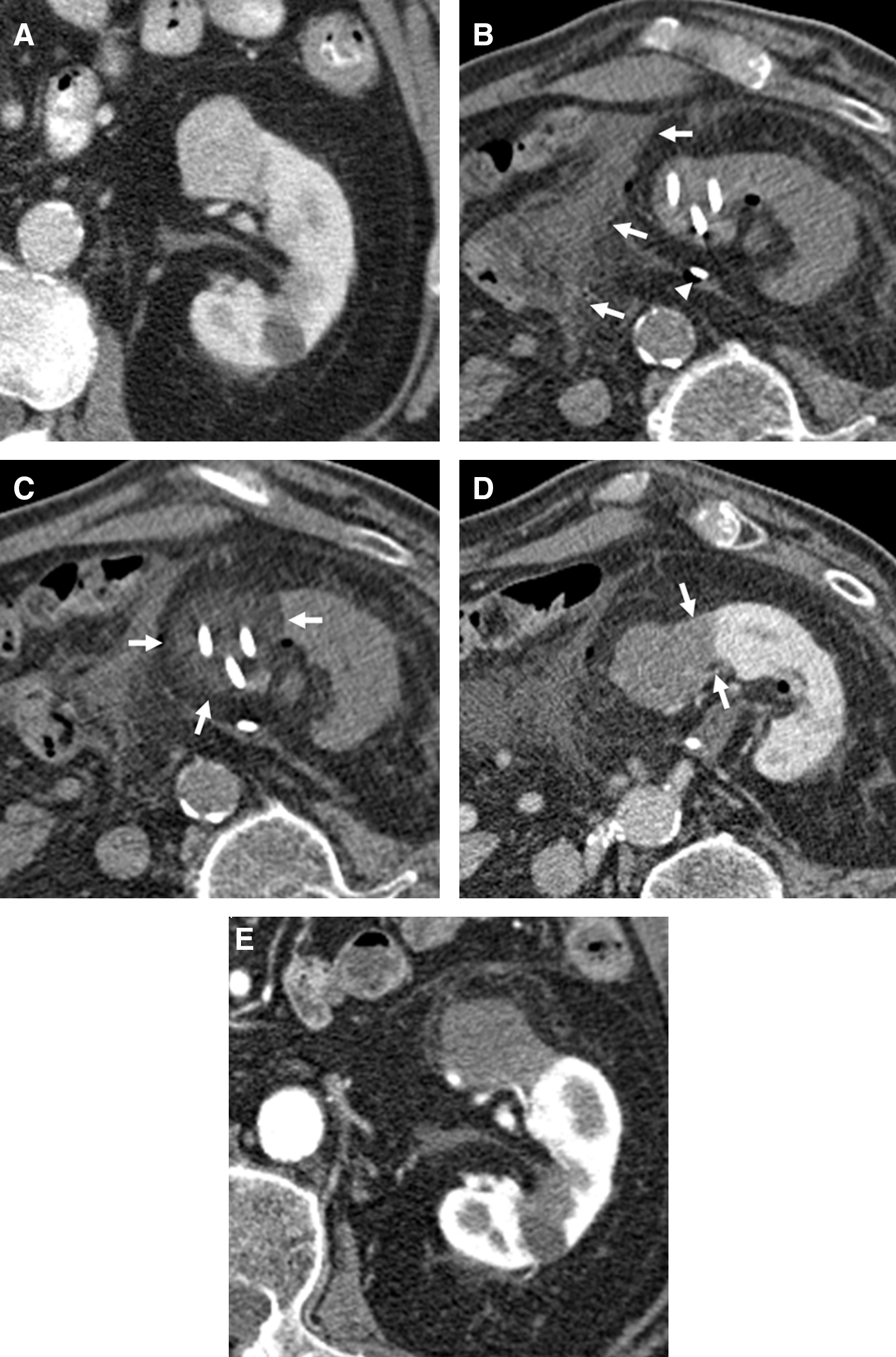
This case demonstrates the use of hydrodisplacement and retrograde pyeloperfusion during cryoablation treatment of an 85-year-old man with biopsy-proven renal-cell carcinoma. (
In a few cases, preablation selective arterial embolization of the tumor was performed with 150 to 250 micron polyvinyl alcohol particles (Ivalon, Uniport Industries, High Point, NC). The goal of this procedure was to eliminate as much arterial flow to the tumor as possible to reduce the amount of bleeding during the subsequent cryoablation procedure. At the same time, the embolization was performed as selectively as possible to preserve as much normal kidney as possible. Although preablation tumor embolization is not uniformly implemented across our practice, it is typically performed the day before the ablation procedure in patients with tumors larger than 5 cm in diameter. Decisions about preablation tumor embolization and temporary externalized ureteral stent placement for pyeloperfusion were made together by the specific interventional radiologist and urologist involved in each case.
The Endocare cryoablation system and Perc-24 cryoablation probes (Endocare, Inc, Irvine, CA) were used in all cases. The Perc-24 cryoablation probes are 2.4 mm in diameter (13-gauge) and will generate an ice ball approximately 3 cm in diameter × 5 cm along the shaft. Rapid expansion of argon gas within the sealed cryoprobe results in freezing of the tissues around the uninsulated tip of the probe. The rate of growth and maximal size of the ice ball is controlled by the rate and length of time argon gas is delivered into the probe during the ablation procedure.
A freeze-passive thaw-freeze cryoablation cycle was performed on each tumor, using a method pathologically proven to be effective for management of renal masses. 19 The length of each freeze time was based on the size of the ice ball necessary to completely encompass the mass. Noncontrast CT monitoring of the size and location of the ablation ice ball was performed at approximately 2-minute intervals during each freeze cycle. The CT images were obtained at 2.5 to 5.0 mm slice thickness and were often reconstructed in different planes during the ablation to ensure that the ice ball completely encompassed the tumor and did not extend to involve adjacent critical structures, including the bowel and ureter. After the second freeze, the ice ball was actively thawed by replacing the argon gas in the cryoprobes with helium gas, and the cryoprobes were removed.
Although there is a synergistic effect on the size of the ice ball created by using multiple cryoprobes, overlapping ablations were necessary for management of the largest renal tumors. Probes were initially placed into the tumor in a configuration to cryoablate (freeze-thaw-freeze) the deepest portion of the tumor. After active thawing of the initial ice ball, the cryoprobes were pulled back and/or readjusted, and a second overlapping cryoablation (freeze-thaw-freeze) was performed to cover the rest of the tumor.
A noncontrast CT was obtained immediately after removal of the cryoprobes to assess for potential complications. In cases in which the patient did not have a contraindication to iodinated contrast, a triphasic contrast-enhanced CT was then performed to further evaluate for technical success of the ablation. Alternatively, MRI was obtained (usually within 24 hours of the procedure) without and with intravenous gadolinium enhancement on a 1.5T system (Signa Excite, GE Healthcare, Chalfont St. Giles, Buckinghamhire, UK).
A contrast-enhanced CT or MRI was performed in 104 of 108 (96%) patients within 3 months of their ablation. Patients who did not undergo enhanced examination included those with iodine and/or gadolinium contrast allergies, and those with significant renal dysfunction (estimated glomerular filtration rate < 30 ml/min), which would have put them at risk for contrast-induced nephropathy or nephrogenic systemic fibrosis.
Technical success was defined as extension of the ice ball at least 0.5 cm beyond the margins of the tumor on monitoring noncontrast CT that was performed during the procedure and/or extension of the ablation zone beyond the margins of the tumor on contrast-enhanced CT or MRI performed within 3 months of the ablation. Local tumor recurrence was defined as a new hyperenhancing or enlarging tissue nodule in, or around, the ablation zone on contrast-enhanced CT or MRI performed 3 months or later after the ablation.
Clinically significant complications were determined according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 3.0. 20 Any grade 3 or greater (severe) adverse events were considered major complications. Postprocedural pain and self-limited nausea and urinary retention related to anesthesia were excluded, but other grade 1 or 2 (mild or moderate) adverse events were reported as minor complications.
After recovery from anesthesia, all patients were admitted to the urology hospital service. Evaluation of statistical significance for the change in patient creatinine level after ablation was performed using the Wilcoxon signed-rank test. P < 0.05 was considered statistically significant.
Results
During the 6-year study period, 108 patients with 110 solid renal tumors ≥3 cm were treated with percutaneous cryoablation. The study group consisted of 75 men and 33 women. Patients averaged 73 years of age (range 24–93 yrs). Average maximal tumor diameter was 4.1 cm (range 3.0–8.3 cm; standard deviation 1.1 cm). Biopsy was performed in 91 of 110 (83%) tumors. Pathology findings were consistent with renal-cell carcinoma in 60 of 91 (66%) cases, oncocytic neoplasm in 7 (8%) cases, oncocytoma in 11 (12%) cases, thyroid metastasis in one (1%) case, and nondiagnostic in 12 (13%) cases. Oncocytic neoplasms were considered those tumors in which the pathologist could not confidently differentiate between an oncocytoma and a renal-cell carcinoma.
A single ablation procedure was performed for treatment of all 108 patients (including the two patients with two tumors each). On average, three cryoprobes were used to ablate each tumor (range 2–8). Initial freeze times averaged 11 minutes (range 6–15 min), passive thaw times averaged 6 minutes (range 5–10 min), and final freeze times averaged 10 minutes (range 4–15 min). Preablation selective arterial embolization was performed on 10 of 110 (9%) tumors, hydrodisplacement of the bowel was necessary in 21 of 108 (19%) patients, and retrograde pyeloperfusion was performed in 11 of 108 (10%) patients.
A technically successful ablation was achieved for 107 of 110 (97%) tumors. All three treatment failures resulted from incomplete tumor ablation along the deepest margin of a centrally located renal mass (Fig. 2). These central renal tumors measured 3.6 cm, 4.0 cm, and 4.4 cm in maximal diameter, respectively. One of the three patients with residual tumor was subsequently treated with laparoscopic radical nephrectomy, a second elected to be treated for his residual tumor at a different institution and was lost to follow-up, and the third was not re-treated because of significant comorbidities. Her residual disease remained stable by CT until she died 1 year later of causes unrelated to renal-cell carcinoma. Local tumor recurrence was not identified in any of the 82 of 108 patients who had follow-up contrast-enhanced CT or MRI performed 3 months or longer after the ablation procedure. Follow-up in these patients averaged 15 months (range 3–42 mos).
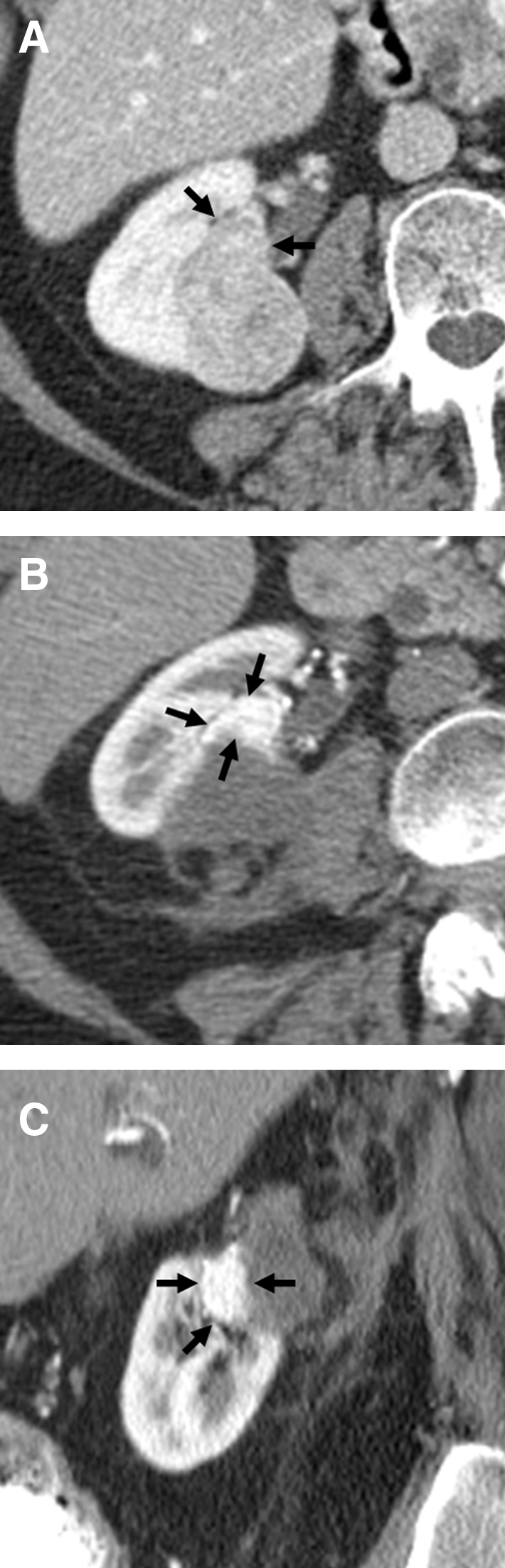
This case demonstrates residual tumor after cryoablation in an 88-year-old man with biopsy-proven renal-cell carcinoma. (
A total of nine severe adverse events occurred in six patients, resulting in an 8% major complication rate in the study group. Significant bleeding after removal of the cryoprobes from the ablated tumor was the cause of one or more major complications in four of these six patients. Each patient went immediately for angiography while still under anesthesia; three needed arterial embolization for active bleeding, and two received blood transfusions (two units each). Two of these four patients also had periprocedural myocardial infarctions, and in addition, acute on chronic renal failure developed in one. The other two patients with major complications unrelated to bleeding included a patient with a periprocedural myocardial infarction, and a patient in whom a pulmonary embolism (diagnosed on CT angiogram 8 days after the cryoablation procedure) developed. All six of these patients recovered from these major complications, and there were no procedural-related deaths.
Of note, two of the patients in whom one or more major complications related to postprocedural bleeding developed were part of a group of only four patients we have treated for a renal mass > 7 cm in diameter (7.2 cm and 8.3 cm in diameter, necessitating 7 and 8 cryoprobes, respectively). In addition, the bleeding complication in the patient with the 8.3 cm renal mass developed despite selective arterial embolization of the tumor on the day before the ablation procedure.
Minor complications in the study group included development of postablation gross hematuria and/or urinary obstruction in nine (8%) patients. Five of these patients needed bladder irrigation via an indwelling Foley catheter, and three also needed cystoscopic clot evacuation and temporary externalized ureteral stent placement. A corneal abrasion developed in one patient caused by adhesive tape placed to hold the eyes shut during general anesthesia. No ureteral or bowel injuries occurred in the study group.
A creatinine level was obtained within 1 week before the procedure and within 1 week after the procedure in 90 of 108 (83%) patients. Mean basal creatinine level for the study patients was 1.3 mg/dL (range 0.5–3.0 mg/dL), and mean postablation creatinine level was 1.4 mg/dL (range 0.5–4.3 mg/dL). This resulted in a mean increase in creatinine of only 0.1 mg/dL (range 0.4–2.0 mg/dL) for these patients, but this was a statistically significant change (P = 0.0004). The single patient with a 2.0 mg/dL rise in serum creatinine level was one of the patients in whom a significant bleeding complication developed and who needed postablation angiography, but no embolization. This patient's preablation creatinine level was 2.3 mg/dL. His creatinine peaked at 4.3 mg/dL 5 days into his hospital admission but then began to improve and was below baseline at 2.0 mg/dL when he was dismissed from the hospital 12 days after the ablation procedure. He did not need dialysis for this episode of acute on chronic renal failure.
All patients were observed in the hospital overnight after the ablation treatment. Average length of hospital stay was 1.8 days (median 1 d; range 1–22 d). 83 Of 108 patients, 83 (77%) were dismissed from the hospital the next day, 14 (13%) patients needed 2 days of hospitalization, and 11 (10%) needed 3 or more days.
Discussion
Nephrectomy (radical or partial) remains the most proven effective treatment for patients with renal-cell carcinoma, with excellent long-term freedom from recurrence and cancer-related death. 21 Image-guided thermal ablation is an excellent treatment option for patients who are poor candidates for open or minimally invasive surgical approaches, including patients with significant medical comorbidities or a history of renal surgery.
Lehman and colleagues 10 published the only laparoscopic renal cryoablation study to date that specifically looks at treatment of patients with renal masses ≥3 cm in diameter. Lehman's group concluded that “laparoscopic cryoablation should be performed only for smaller than 3 cm lesions,” while our study would indicate that percutaneous cryoablation of these larger renal tumors can be performed with a low rate of significant complications. The major complication rate in the laparoscopic renal ablation study by Lehman and coworkers for masses ≥3 cm was 62%, compared with only 8% in this study. There were also two periprocedural deaths (9.5% mortality) in the 21 patients in the Lehman study group, compared with 0% mortalities in this study. Evidence for residual/recurrent tumor was similar in the two study groups (5% in the laparoscopic renal cryoablation study and 3% in this study).
Cryoablation was chosen for treatment of the patients in this study group primarily because their renal tumors were ≥3 cm in diameter. In three of the largest percutaneous radiofrequency ablation studies (combined total of 285 patients), treatment was technically successful in 99% to 100% of patients who were treated for a renal tumor < 3 cm in diameter. 4,13,22 In contrast, technical success was achieved in only 60% to 81% of cases in which radiofrequency ablation was used to treat a renal mass ≥3 cm in diameter. Although this is significantly lower than the 97% technical success rate seen in this study, the relatively poor performance of radiofrequency ablation in the management of renal masses ≥3 cm reflects treatment before multiple-electrode radiofrequency ablation systems became available, and use of newer systems may lead to more effective management of larger renal tumors.
Having a centrally located renal tumor was a secondary reason for choosing cryoablation in many of these cases. In two of the largest radiofrequency ablation studies (combined total of 150 patients), treatment of peripheral renal masses was technically successful in 106 of 106 (100%) patients, but treatment of central renal masses was technically successful in only 33 of 44 (75%) cases. 4,13 Although all of the technical failures in our study were also seen with treatment of central renal tumors, a technically successful ablation was achieved in 64 of 67 (95%) cases.
Choosing cryoablation rather than radiofrequency ablation also has potential safety advantages for managing renal masses in close proximity to the ureter and/or bowel. It is relatively easy to follow the size and location of the ablation zone (ice ball) by noncontrast CT during a percutaneous cryoablation, while determining the size and location of a radiofrequency ablation zone is more difficult by imaging.
Despite our success with percutaneous cryoablation of renal masses, we still perform radiofrequency ablations for treatment of some renal tumors. Radiofrequency ablation of small peripheral renal masses can be performed more quickly than cryoablation, and with almost identical technical success rates. Radiofrequency ablation also allows cauterization of the ablation needle tracks.
The results of this percutaneous renal cryoablation study are slightly better than those published from other groups. 7 –11 Reasons for this may include: (1) We have an experienced multidisciplinary team of urologists and radiologists who carefully select ablation cases that are highly likely to be successful; (2) we have a lot of experience with performing percutaneous renal cryoablations; (3) real-time ultrasonographic guidance is used for the procedures in addition to CT, which allows precise placement of the cryoprobes within the renal tumor; and (4) we perform all renal cryoablations with the patients under general anesthesia, which has been shown to improve results compared with those performed with moderate sedation. 23
Although commonly accepted criteria for a technically unsuccessful ablation (residual disease) and locally recurrent tumor (recurrent disease) were used in this study, the 3-month cutoff between residual and recurrent tumor is still somewhat arbitrary and confusing. 24 Initial determination of a technically unsuccessful ablation was actually made on the 3-month follow-up CT for all three patients in this study group. Retrospective review, however, of the immediate postablation CTs revealed residual hyperenhancing tumor outside the ablation zone in all three patients. Because the hyperenhancing tumor was not new, these cases were considered technical failures rather than local tumor recurrences. In no cases did the findings of the immediate postablation contrast-enhanced CT result in re-treatment of the renal tumor. If the residual renal tumor had been identified by the interventional radiologist immediately after the procedure in the three failed ablation patients, reablation of the residual tumor would have been performed at that time while the patient was still under general anesthesia.
Two relatively unproven prophylactic techniques used for treatment in some of the study patients were retrograde pyeloperfusion via an externalized ureteral stent and preablation selective tumor arterial embolization. The use of retrograde pyeloperfusion has been adopted for renal cryoablation primarily because of the apparent efficacy of this technique for protecting the ureter during renal radiofrequency ablation. 18 It is proposed that circulating fluid within the ureter creates a thermal sink effect that may be protective of the ureter during radiofrequency ablation and possibly cryoablation procedures. 25
A small retrospective study from our institution suggests that there is less bleeding during cryoablation of tumors ≥5 cm if they are pretreated with selective arterial tumor embolization. 26 Additional studies are certainly necessary, however, to establish the efficacy of preablation arterial tumor embolization and retrograde pyeloperfusion for renal cryoablation.
A major limitation of this study is the relatively short patient follow-up. We practice at a tertiary care center and, unfortunately, many patients do not return to our institution for long-term follow-up after renal ablation. Also, many of the ablations of larger renal masses have been performed more recently, and these patients therefore have shorter follow-up. Finally, 6 of the 108 study patients have died since their ablation procedure of causes unrelated to their renal tumors, which obviously shortens follow-up in this group. A second limitation of the study is that evidence for local disease progression (residual or recurrent tumor) relies on radiographic findings only. Determining technical success of a cryoablation by extension of the ice ball 0.5cm or greater beyond the edges of the renal tumor can be difficult to confirm with noncontrast CT. Performing a contrast-enhanced examination immediately after the cryoablation also helps evaluate for technical success of the procedure, but it is sometimes difficult to confidently exclude residual tumor on these images as well.
A third limitation of the study is the lack of pathologic proof of renal tumor type in 28% of cases. One major reason for this was the difficulty in obtaining good core biopsy specimens from the tumor after placement of the cryoprobes. Unfortunately, even a small amount of bleeding associated with a biopsy can obscure visualization of the tumor for placement of the probes by real-time ultrasonographic guidance. Because we perform ablation of any solid renal mass regardless of pathology, we would generally like to assure optimal placement of the cryoprobes and struggle with a good biopsy specimen, rather than get a great biopsy specimen and risk getting a suboptimal ablation.
Conclusions
Percutaneous cryoablation of solid renal masses ≥3 cm in diameter can be performed with high technical success, low complications, and high local tumor control rates (based on short-term follow-up). When compared with published data, results of this study would suggest that percutaneous cryoablation of renal masses ≥3 cm can be performed with higher technical success rates than percutaneous radiofrequency ablation and with lower complication rates than laparoscopic renal cryoablation. It is important when treating central renal tumors to make sure the cryoablation zone extends to include the deepest margin of the tumor. Although our experience is limited, percutaneous cryoablation of renal masses >7 cm in diameter may be associated with an increased risk of bleeding complications.
Footnotes
Disclosure Statement
No competing financial interests exist.