
Abstract
Purpose:
To assess the feasibility, describe the technique, and report our experience with use of the da Vinci S robotic surgical system in the management of pheochromocytoma.
Patients and Methods:
For four patients with metabolically active adrenal pheochromocytoma (two right, two left), standard preoperative preparation was performed. A robotic transperitoneal approach was used for all cases. Sparing of the adjacent normal parenchyma was performed in all cases. All relevant perioperative details were collected and analyzed.
Results:
Mean operative time was 77.5 minutes (range 40–140 min), and blood loss was 97.5 mL (range 50–160 mL). There were no conversions or perioperative complications. Average tumor size was 4.7 cm. There were three episodes of intraoperative hypertension necessitating therapeutic intervention. Average analgesic requirement was 150 mg of diclofenac, and patients were allowed oral intake after 6 hours. The drain was removed within 24 hours, with average hospital stay of 4 days. The histopathology report confirmed pheochromocytoma in all patients with free surgical resection margins. Average follow-up was 9 months (range 4–14 mos) with no evidence of recurrence or extra-adrenal tumor.
Conclusion:
Robot-assisted excision of pheochromocytoma is feasible, safe, and efficacious in our early experience. Sparing of the normal adjacent adrenal parenchyma is possible with little detrimental effect on the oncologic efficacy of the surgery. Long-term studies are needed to further confirm this issue.
Introduction
With our increasing experience in robot-assisted surgery, we try to assess feasibility, describe the technique, and report outcomes with the use of the da Vinci S® (Intuitive Surgical, Sunnyvale, CA) robotic surgical system in the management of adrenal pheochromocytoma.
Patients and Methods
Patients presenting from July 2006 to June 2009 with a diagnosis of metabolically active pheochromocytoma and undergoing robot-assisted tumor excision were included in the study. All diagnoses were confirmed on biochemical evaluation with urinary vanillyl-mandelic acid, catecholamines and metanephrines. The inclusion criteria for robot-assisted surgery included clinically localized disease with no previous abdominal surgery. The site, size, and extension of the lesion were assessed by preoperative abdominal MRI. A meta-iodo-benzyl-guanidine (MIBG) scan was also performed to evaluate for any concurrent extra-adrenal lesion.
All procedures were performed by a single surgeon (NPG) with experience in both open and laparoscopic surgeries of the adrenal gland. Detailed cardiac and preanesthesia evaluation was performed. Preoperative preparation included administration of alpha (prazosin) and beta blocker (propranol or atenelol) in all cases with or without other antihypertensive drugs. Hydration was given to all patients to achieve a hematocrit of 35 to 37. Preparations were made to control intraoperative fluctuations of blood pressure with sodium nitroprusside, magnesium sulphate, labetalol, dopamine, noradrenaline, and adrenaline. Details of the number of intraoperative fluctuations in blood pressure were noted from the anesthesia charts. They were defined as fluctuations of more than 20 mm Hg, necessitating administration of drugs.
Technique
Our technique for robot-assisted adrenal pheochromocytoma excision is described. All procedures were performed with robot-assisted technique through the transperitoneal route.
Patient position
After urethral catheterization, the patient is turned to a lateral decubitus position angled at 60 degrees with the floor, with the tumor side facing up. A bolster is kept underneath the contralateral flank. All pressure points are padded up.
Port position (Fig. 1)
Pneumoperitoneum is created with the Veress needle inserted through the ipsilateral lower abdominal quadrant. The same site is subsequently used for insertion of a port for one of the robotic arms. The insufflation is performed slowly to avoid sudden compression of the tumor. The paraumbilical port (12 mm) is inserted first and used for the camera. Two robotic arm ports (8 mm) are inserted, as shown in Figure 1. Overall, four ports (three robotic, one assistant) were used for left adrenal tumors and five ports (three robotic, two assistant) for right adrenal tumors. We use articulating curved monopolar robotic scissors in the right robotic arm and a Maryland bipolar robotic grasper in the left robotic arm for the entire dissection.
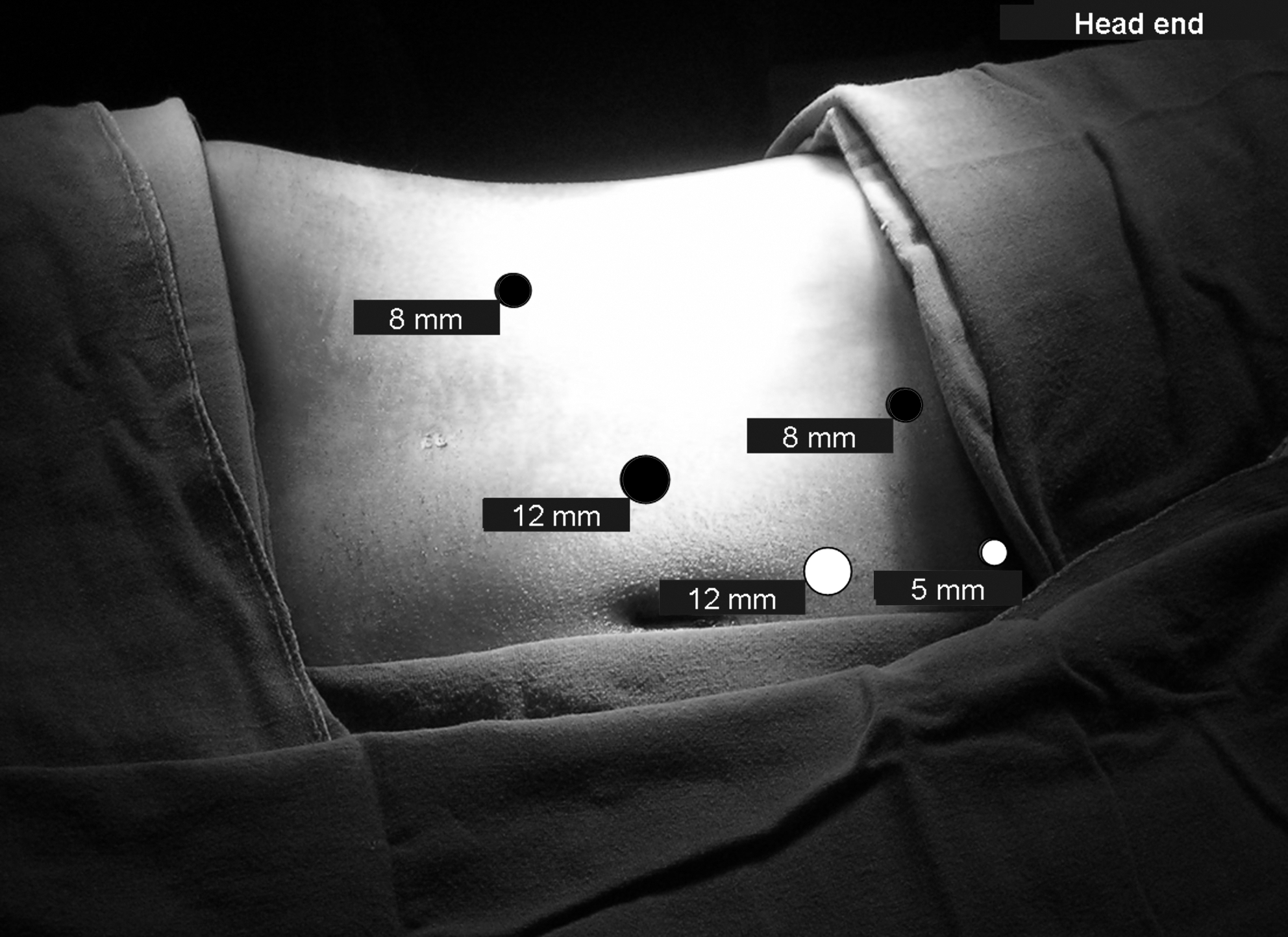
Port position used for right robotic excision of pheochromocytoma. The robotic ports (one 12-mm camera and two 8-mm instrument arms) are shown in black while assistant ports (one 12-mm and one 5-mm for liver retraction) are shown in white. The 5-mm assistant port is unnecessary on the left side.
Reflection of colon
The splenic or hepatic flexure of the colon is reflected down with sharp and blunt dissection to expose the renal and adrenal surface until the lateral margin of the great vessels.
Adrenal dissection
Dissection is first performed on the medial side of the adrenal, and all draining veins are clipped. Classically, the right-side vein lies at the anterosuperomedial aspect of the adrenal while the left one lies at the anteroinferomedial aspect of the adrenal. 3 More often, however, several small draining veins may be identified. We prefer to individually clip all these veins and cut. The maneuvering capacity of the robotic instruments is immensely helpful at this step. Gentle rolling of the vena cava by the assistant also helps to keep the draining veins at stretch to aid in dissection on the right side. Care is exercised in the small space between the right adrenal, vena cava, and the liver where a vein may sometimes be identified draining the caudate lobe of the liver into the vena cava. Similarly on the left side, injury to the pancreas should be avoided. Care is also taken to minimize tumor handling until medial dissection is completed, after which handling becomes somewhat more benevolent. This helps in minimizing release of catecholamines and hemodynamic fluctuations.
The Gerota fascia is then opened if it is not already thinned out from the pressure effect of the tumor. The tumor can then be excised by dissecting all around it with an effort to spare the adjacent normal parenchyma (Fig. 2), at the same time taking care not to breach the tumor pseudocapsule. All intraparenchymal vessels are individually ligated with clips.
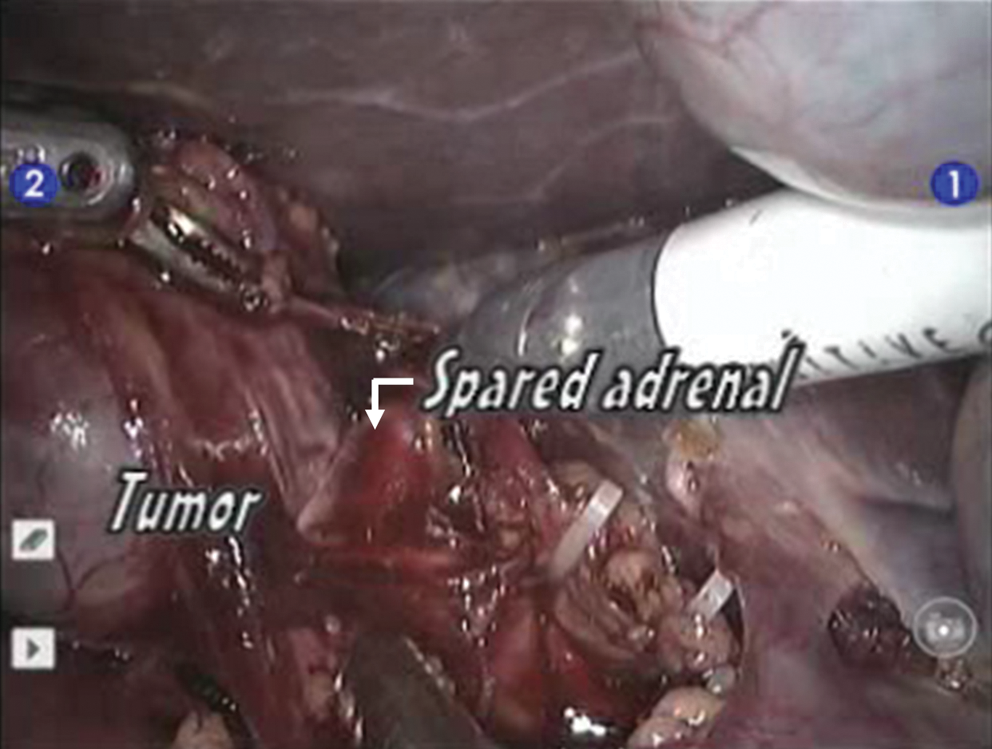
Operative photograph showing sparing of adrenocortical tissue in a case of robot-assisted surgery for right-sided pheochromocytoma.
Hemostasis, specimen retrieval, and port closure
Hemostasis is assured by observing the surgical field with reduced abdominal insufflation pressure for some time. The specimen is then entrapped in an endocatch bag and removed by extending the umbilical port. A Jackson-Pratt drain is placed in the peritoneal cavity, and the port sites are then closed.
We performed tumor excision with sparing of the adjacent adrenal in all four patients. The relevant perioperative details were collected and analyzed.
Results
Four patients (two men, two women) underwent robot-assisted adrenal-sparing excision for metabolically active adrenal pheochromocytoma (two right, two left). Relevant demographic and perioperative details of the patients are in Table 1. The average size of adrenal tumors was 4.7 cm (range 3–6.8 cm) in longest dimension (Fig. 3). All cases were completed robotically with no perioperative complications.

(
Intraop = intraoperative; BP = blood pressure; postop = postoperative.
The average operative time was 77.5 minutes (range 40–140 min) with blood loss of 97.5 mL (range 50–160 mL). Intervention for hemodynamic fluctuations was necessary for one episode of hypertension in a case of large left adrenal tumor. Postoperative hypotension was seen in two patients, lasting for a few hours. It was managed with dopamine infusion. Resumption of oral feeds occurred after 6 hours in all patients. The drain was removed within 24 hours in all patients, and average hospital stay was 4 days. Average analgesic consumption was 150 mg of diclofenac sodium. Histopathology results confirmed pheochromocytoma in all cases with free surgical resection margins. Average follow-up was 9 months (range 4–14 mos) with no evidence of recurrence or extra-adrenal tumor on 3-month MIBG scan. The repeated biochemical functional evaluation was also normal in all cases.
Discussion
Ever since its introduction into the surgical armamentarium, the use and indications of robot-assisted surgery have been expanding. Robot-assisted adrenalectomy for pheochromocytoma was first reported in 2001 by Horgan and Vanuno. 4 Subsequently, other groups have assessed feasibility and efficacy of robot-assisted adrenalectomy in short case series with good outcomes. 5 –7 Benincà and associates 8 reported poor results in their early experience, with four of nine cases needing conversion to an open procedure.
In early series, direct comparisons between laparoscopic and robotic techniques of adrenalectomy concluded in favor of pure laparoscopic technique, with better operative time, morbidity, cosmesis, and cost. 9,10 More recent literature has, however, shown equal and good outcomes with the use of robotic technology, 11 –13 Stress has been on previous laparoscopic expertise, first assistant's skills, and tumor side/size on the perioperative results. 11,14 Robotic technique definitely also provides ergonomic advantage in terms of surgeon comfort, intuitive instrument handling, and seven degrees of movements. In addition, the da Vinci system has provided a means for laparoscopically naïve surgeons to offer the benefits of minimally invasive surgery to their patients with safety and ease. More studies are necessary to assess the overall efficacy of robot-assisted adrenalectomy.
Our experience in this short case series has shown excellent results. The chief operating surgeon had extensive experience in both open and laparoscopic adrenalectomy before embarking on the robot-assisted surgery.
Overall, we could achieve good short-term surgical outcomes with an attempt to preserve the normal adrenal parenchyma. Our results corroborate well with some other published series with adrenal-preserving laparoscopic surgery. 15 A recent comprehensive literature review for partial adrenalectomy has shown acceptable early outcomes. 16 Walz and colleagues 17 reported no difference in the perioperative or long-term oncologic outcomes between total (224 cases) or partial adrenalectomy (96 cases) for patients with a variety of indications for surgery. Their study included 33 cases of partial and 50 cases of total adrenalectomy for pheochromocytoma.
An exact estimation of the residual gland volume is difficult in the postoperative period. 18 There is as yet no defined modality to estimate the viability and functioning of the remaining adrenal tissue in patients with a normal opposite adrenal gland. A relative adrenal residual volume of 10% to 15% has been shown to provide an intact stress capacity. 18 A partial excision of adrenal is usually practiced in cases of von Hippel-Lindau syndrome, multiple endocrine neoplasia type-2, bilateral diseases, and benign adenomas. 18
Pheochromocytoma is a tumor that arises from the adrenal medulla, and the cortical tissue remains uninvolved. It is not possible, however, to differentiate between the involved adrenomedullary tissue and the uninvolved adrenocortical tissue during the surgery. Therefore, subtotal or partial adrenalectomy is not universally accepted, given the availability of oral replacement therapy for the hormones produced by the adrenal gland. 18 Its role or benefit in cases with a normal contralateral gland has never been studied, given the absence of any apparent advantage. The exact worth of partial adrenalectomy in such cases still needs to be deduced by studying the stress responses of the patients preoperatively and postoperatively.
Usually the tumor nodule in the adrenal medulla stretches the overlying cortical tissue at one pole while the normal tissue at the opposite pole remains unstretched. It is at this unstretched pole that the surgeon can dissect along the tumor pseudocapsule while preserving the normal cortical tissue. An intraoperative ultrasound probe may help to ensure complete tumor removal.
When selecting patients for partial adrenalectomy, the potential risks of tumor spillage, recurrence, and malignancy should be balanced carefully against the potential problems of lifelong steroid replacement and addisonian crisis. Adrenal tumors more than 6 cm are more prone to be malignant. Also, the risk of tumor spillage is correspondingly higher and the possibility of finding normal tissue is lower with the increasing size of the tumor. This group of patients, therefore, should be selected very cautiously for partial adrenalectomy. A repeated subtotal adrenalectomy for recurrence after an initial partial adrenalectomy has also been reported in the literature with good results. 19
In our short series, we found no detrimental effect on oncologic or functional outcomes with the technique of adrenal-sparing surgery. The average follow-up period, however, is not very long, and continued follow-up is essential to further confirm oncologic adequacy.
Another peculiar finding was more blood loss and longer operative time for left-sided surgery than surgery for the right side. This might be explained by larger left-sided tumors in this series. Even after taking this into account, however, left-sided surgery has been reportedly technically more difficult and time consuming. 11
In regard to anesthetic considerations, reports that focused specifically on management of pheochromocytoma have shown better results with laparoscopy compared with the open technique.
2
Robot-assisted surgery is a further extension of laparoscopy, and anesthetic implications should be more or less similar. Our early results have shown very few hemodynamic fluctuations necessitating therapeutic interventions on the part of anesthetists in cases of metabolically active pheochromocytoma. Factors that may have helped in achieving such results and avoiding surgery-induced catecholamine storm include: Good preoperative preparation with hydration, alpha/beta blockers, and antihypertensive drugs. Intraperitoneal pressure of pneumoperitoneum that may compress the small adrenal veins. Good surgical technique with minimal tissue handling. Medial dissection of the adrenal being the first step of surgery to clip and cut the draining veins.
The expertise of the treating anesthetists is also important in this regard. Also, the robotic instruments allow the surgeon to follow open surgical principles by providing seven degrees freedom of movement and exactly replicating the surgeon's movements inside the patient's body. This is in stark contrast to pure laparoscopic instruments that provide only four degrees of freedom of movement with fulcrum effect necessitating significant tumor manipulation to dissect around it.
The occurrence of only trivial fluctuations in the hemodynamic parameters during the surgery is attestation to the precision and range of mobility offered by the robotic system. It allows dissection into the critical region between the adrenal and inferior vena cava with relative ease. Some authors caution against the high cardiovascular risk at the time of induction of pneumoperitoneum. 20,21 We did not encounter any such event in this series. We start insufflation with low flow rates to achieve gradual increase in intra-abdominal pressure and avoid sudden compression of the tumor and release of catecholamines into the systemic circulation.
Our series represents results of robot-assisted surgery from a tertiary care center, but we believe that with wider availability of this technology, more and more laparoscopy naïve surgeons shall be able to practice minimally invasive surgery in the near future. The cost of the robot surely remains one prohibitive factor for the application of this technology in widespread practice.
Conclusion
Robotic management of functionally active pheochromocytoma is safe and feasible. It has shown efficacious results in our short early experience. Sparing of the normal adjacent adrenal parenchyma is possible with little detrimental effect on the oncologic efficacy of the surgery. Long-term studies with a larger number of patients are essential to establish robot-assisted surgery as a widely acceptable treatment modality for patients with pheochromocytoma.
Footnotes
Disclosure Statement
No competing financial interests exist.