
Abstract
Background and Purpose:
Today's simulators are frequently limited in their possibilities to train all aspects of endourological procedures. It is therefore indicated to first make an inventory of training needs before (re)developing simulators. This study examined pitfalls encountered by residents in real-time transurethral procedures.
Materials and Methods:
First, difficulties that residents encounter in transurethral procedures (transurethral resection of the bladder tumor [TURBT], transurethral resection of the prostate [TURP], ureterorenoscopy [URS]) were identified by asking urologists and residents to complete an open questionnaire. Based on their answers a list of pitfalls was designed and tested in 28 pilot observations. Then, two raters (interrater agreement 0.72, 0.70, and 0.75 for TURBT, TURP, and URS, respectively) categorized all observed procedure-related interactions between residents and supervisors in 80 procedures as (1) (type of ) pitfall or (2) no pitfall.
Results:
Pitfalls most frequently encountered were as follows: (1) planning/anticipation on new situations (median 27.3%, 29.3%, and 31.8% of total pitfalls in TURBT, TURP, and URS, respectively); (2) handling of instruments (11.5%, 10.6%, and 20.0% for TURBT, TURP, and URS); (3) irrigation management for TURBT (7.7%), depth of resection for TURP (8.9%), and use of X-ray for URS (13.3%).
Conclusion:
Designers of endourological simulators should include possibilities to train planning/anticipation on new situations, handling of instruments in all transurethral procedures, and irrigation management in TURBT, depth of resection in TURP, and timing usage of X-ray in URS.
Introduction
Interest in the development of structured training programs and the use of simulators as training tools in surgery is rapidly growing. 1 –3 In recent years, various studies presented and examined the value of endourological simulators as educational tools. 4 –16 Similar to the first years of development of simulators for military training, endourological simulator procurement has been mainly a technology-pushed process driven by what was offered on the market. 17 Today's endourological simulators are still frequently limited in their possibilities to train important aspects of procedures. 15,18 The majority of urological training programs are still based on the traditional Halstedian master-apprentice type of training. To be able to develop simulators and to design standardized training programs that are aligned with real-time experiences, it is of paramount importance to identify the problems (pitfalls) encountered by residents when they are learning to perform real-time procedures in patients. In other words, training needs should first be defined. 17,19,20
Considering transurethral procedures, some studies have been performed to gain insight in the learning curves and pitfalls of these procedures. One research group evaluated 842 transurethral resection of the bladder tumor (TURBT) procedures, performed by five novice trainees. 21,22 Their analysis included tumor characteristics, complications, and histological results. 21,22 They thus concentrated on the outcomes of the procedure, but did not provide information on the problems or difficulties that postgraduates encountered while performing the procedure. For the transurethral resection of the prostate (TURP), several studies described the learning curves of urologists who were already experts in performing the original TURP, with new techniques such as the Holmium laser enucleation of the prostate. 23 –25 However, the original TURP remains a common practice in the majority of hospitals 25 and neither the learning curve nor the pitfalls of postgraduates concerning this procedure have, to our knowledge, been described in literature. For ureterorenoscopy (URS), TURBT, and TURP, operative steps and tips are described in the book “Manual Endourology.” 26 Although this provides tips and tricks and a good overview of steps the procedures consist of, it does not show which pitfalls postgraduates encounter at which moment in the learning process and how to anticipate on these pitfalls in a training program.
This study addressed the research question “What pitfalls do residents encounter when learning to perform TURBT, TURP, and URS procedures in patients in master-apprentice type of training?”
Materials and Methods
Design of list of pitfalls
In the preparation phase of this study, urologists and residents were asked to answer an open questionnaire about difficulties that residents encounter in TURBT, TURP, and URS procedures. They were asked for their voluntary participation in between daily practice or during a national symposium on endourological training techniques in November 2007. Nine urologists and 26 residents filled in the questionnaire about TURBT, and 10 urologists and 7 residents about TURP and URS. Based on these answers a list of pitfalls per procedure was developed. This list was then refined based on the results of a pilot study in which we analyzed 18 TURBT, 3 TURP, and 7 URS procedures.
Observation of real-time procedures
Between May 2008 and January 2009, supervised residents were observed in 37 TURBT, 22 TURP, and 21 URS procedures in three teaching hospitals in The Netherlands. The observer was present in the operating room (OR) and recorded every verbal or physical procedure-related intervention by the supervisor (urologists) and instances when the trainee (resident) asked for assistance in performing the procedure. This observer (who was the same observer for all three teaching hospitals) was trained in observing the procedures in the previously mentioned pilot study.
Afterward, this observer and a researcher who had not been present in the OR classified the noted interactions as (1) (type of ) pitfall or (2) no pitfall. Mean interrater agreement was 0.72, 0.70, and 0.75 for TURBT, TURP, and URS, respectively. The two raters discussed any differences in classification until agreement was reached.
The participating residents and supervising urologists were volunteers and we obtained their informed consent verbally and in writing. In The Netherlands, the 6-year specialist training program in urology consists of 2 years in general surgery, followed by 4 years in urology. The participants in the study were in the final 4 years of their training. Residents who functioned at consultant level, that is, who routinely performed the transurethral procedures without supervision, were excluded.
Residents' and urologists' awareness of the presence of an observer in the OR during the procedure could potentially influence their interactions. We counteracted this by performing a pilot study in which the supervisors and the residents got used to the observer being present. Moreover, the observer did not participate in the procedure but sat in a corner of the OR without interfering in the procedures.
The Medical Review Ethics Committee of The Netherlands declared that submittal of the study protocol was not required, as this study consisted of observations and thus involved no intervention in the normal treatment of patients.
In all participating hospitals a display showing internal endourological images was used during transurethral resections. Included in the study were TURBT procedures, with resection using a resectoscope, of bladder tumors of all sizes and all usual types of invasiveness. Only conventional TURP procedures were included and thus no alternative nonablative treatment options such as laser, thermo, and cryo treatment were used. Diagnostic URS procedures and URS procedures involving stone and/or tumor treatment were included. In all hospitals, flexible as well as semirigid URS procedures could be performed. Fiberoptic scopes were used for flexible URS procedures; procedures with digital ureteroscopes were excluded. New techniques such as digital URS and other TURP procedures than the conventional ones were excluded because most urologists were in the learning curve of this technique themselves. Also, results would be too diverse and heterogeneous and therefore not comparable when including too many different techniques. Whenever an Otis or Sachse urethrotomy was part of a procedure, this part of the procedure was not included in the study, because this is considered another type of endourological procedure than the three that we aimed to investigate (TURBT, TURP, and URS).
After the procedure the supervisors completed a questionnaire with items to rate the procedure's complexity using a predefined complexity scale (Table 1a–c). This scoring list had been developed by consulting five urologists who were experienced in all three procedures (having performed >100 procedures of each type). They were asked to indicate the different levels of difficulty of the procedures and the list was discussed until all five experts agreed on this scoring scale. As shown in Table 1a–c, the complexity ranges from 3 (least complex) to 15 (most complex) for TURBT, from 3 to 10 for TURP, and from 1 to 25 for URS.
Classification of the Level of Difficulty in Transurethral Resection of the Bladder Tumor
*Ta/CIS/T1/T2 according to official European TNM classification.
Classification of the Level of Difficulty in Transurethral Resection of the Prostate
EBRT = external beam radiotherapy; TURP = transurethral resection of the prostate.
Classification of the Level of Difficulty in Ureterorenoscopy
UPJ = ureteropelvic junction.
Statistics
Individual urologists have different styles of verbal guidance and supervision, that is, some supervisors have the tendency to talk and provide tips and tricks nonstop during the procedure, while others have a more restrained manner of supervising trainees. Therefore, for the analysis we used relative numbers (for each procedure we divided the number of occurrences of each type of pitfall by the total number of pitfalls) instead of absolute numbers. The Mann–Whitney U or chi-square test was used to compare demographic data between groups. Spearman correlation was used to evaluate correlations between the three most frequently occurring types of pitfalls and the level of complexity of the procedure/level of experience of the trainee. A p-value of <0.05 was used for all tests to indicate statistical significance. All statistical analyses were performed using SPPS version 15.0 (London, United Kingdom).
Results
Design of list of pitfalls
The designed list of pitfalls, based on the open questionnaire among urologists and residents and the pilot observations, is shown in Table 2. Pitfalls are not arranged according to importance, but are arranged in chronological order as far as possible as they occur during a given intervention. In real time, one pitfall may be more important or have more consequences for the patient than another pitfall. However, this estimation of importance is generally dependent on multiple individual patient- and doctor-related circumstances, such as sex and thickness of bladder wall, medical history, and usage of anticoagulantia. Moreover, opinions about importance may differ among experts. For this reason, no classification of importance was used.
List of Pitfalls
Translated from original Dutch version. P1 to P16 in chronological order as far as possible.
P = pitfall; 3D = three-dimensional; TURBT = transurethral resection of the bladder tumor; URS = ureterorenoscopy.
Analysis of pitfalls in real-time procedures
The general demographics of the residents and urologists are presented in Table 3. Urologists were significantly older than residents. One TURBT operation was excluded because it turned out that the pathology consisted of stitches from a previous gynecological operation. One TURP was excluded because it was a “cold TURP,” involving removal of necrotic prostate tissue after brachytherapy without warm resection. One URS was excluded because URS indicated an Acucise procedure for ureteropelvic junction stenosis.
General Demographics
Median operating time for TURBT, TURP, and URS was 29 minutes (range, 8–115), 50 minutes (24–105), and 64 minutes (21–134), respectively. The median levels of complexity of TURBT, TURP, and URS procedures were 4.0 (range, 3–13), 2.5 (2–10), and 11.0 (1–23), respectively.
Median number of interactions between supervisor and trainee was 26 (range, 2–85) for the TURBT procedures, 32 (11–116) for the TURP procedures, and 44 (24–134) for the URS procedures. During all three types of procedures, the number of times the supervisor provided verbal guidance was significantly larger than the number of times the trainee asked for guidance (all p-values <0.0001). The median numbers of pitfalls identified for TURBT, TURP, and URS were 21 (1–78), 28 (5–104), and 32 (15–110), respectively. In all three procedures, the most frequently encountered pitfall was “planning/anticipation on a new situation” (median percentage of the total number of pitfalls was 27.3%, 29.3%, and 31.8% for TURBT, TURP, and URS, respectively; Figs. 1 –3). A frequent example of a situation in the pitfall category was a moment in which the resident did not know what the next step was in the procedure and asked the supervisor how to continue with the procedure. Another example of “planning/anticipation on a new situation” was the occurrence of a blurred vision, for example, by blood, in which the resident needed verbal guidance to regain vision before he/she was able to proceed with resection of the prostate or tumor. The second most frequently encountered type of pitfall for all procedures was “handling of instruments” (median was 11.5%, 10.6%, and 20.0% for TURBT, TURP, and URS, respectively). The third most frequently encountered type of pitfall was “irrigation management” for TURBT (median, 7.7%), “depth of resection” for TURP (median, 8.9%), and “timing of usage of X-ray” for URS (median, 13.3%). No significant correlations were found between the three most frequently encountered pitfalls and the complexity of the procedure or the trainee's level of experience.
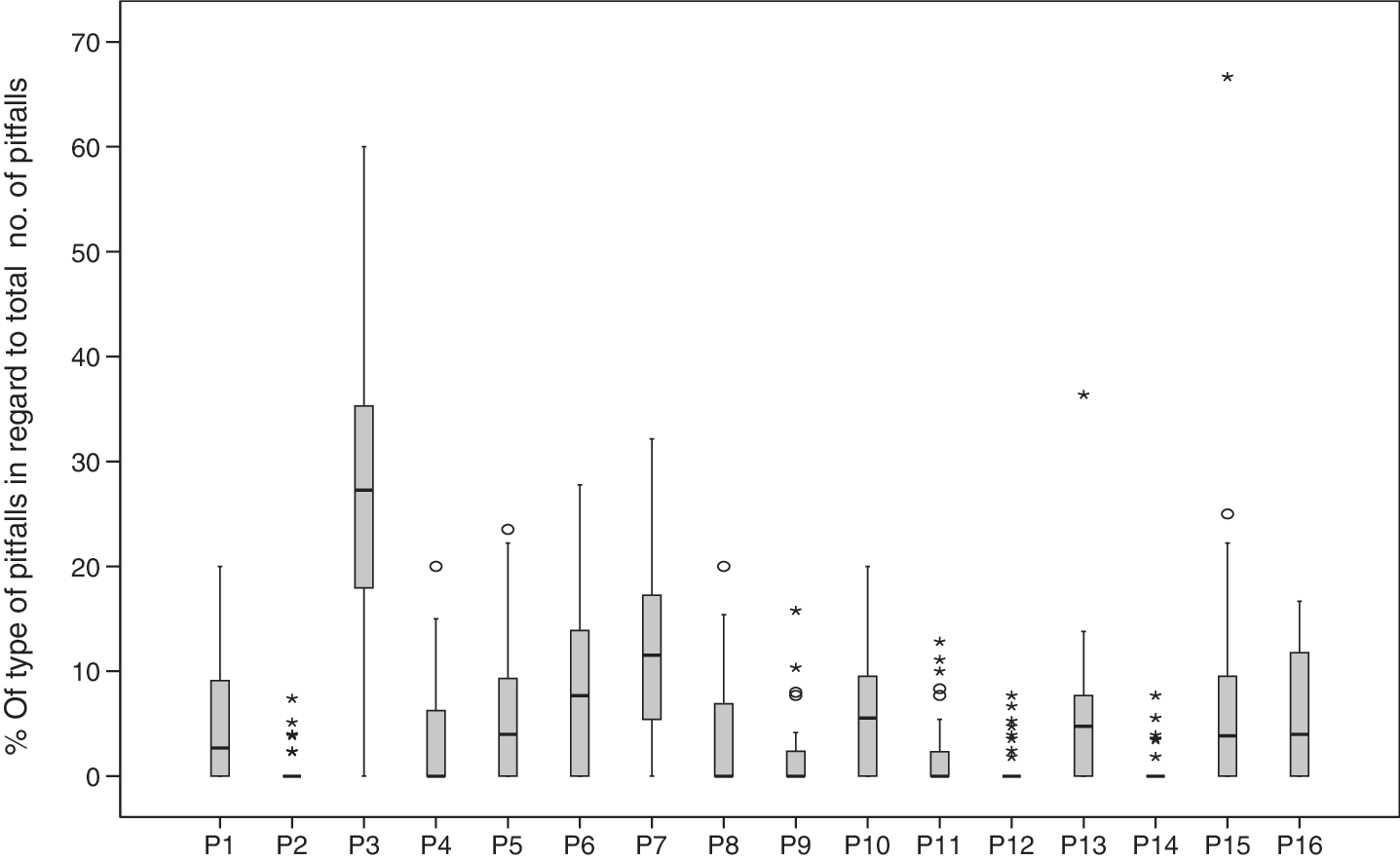
Frequency of occurrence of different types of pitfalls—transurethral resection of the bladder tumor. For description of pitfalls P1 to P16 see Table 1.
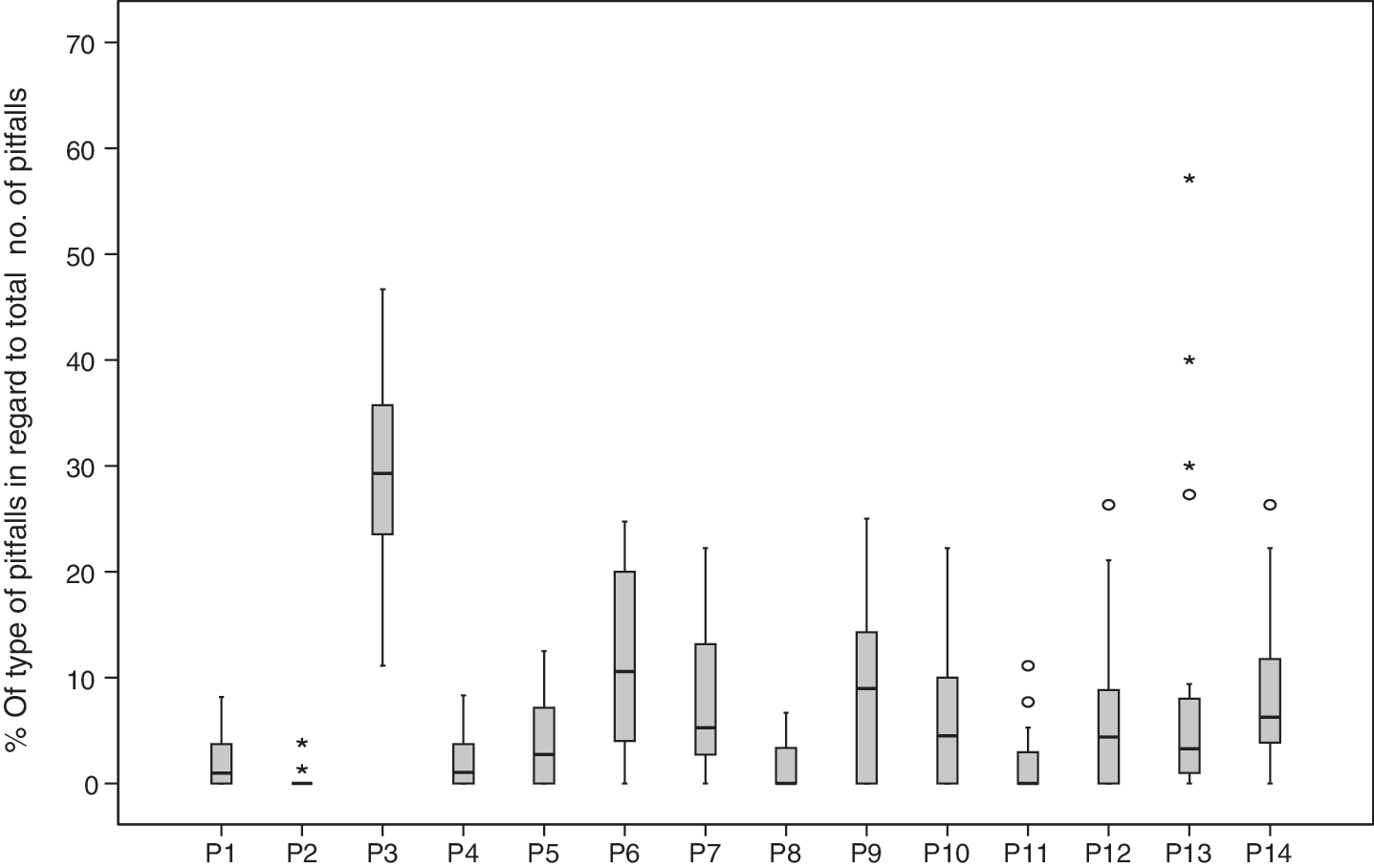
Frequency of type of pitfalls—transurethral resection of the prostate. For description of pitfalls P1 to P16 see Table 1.
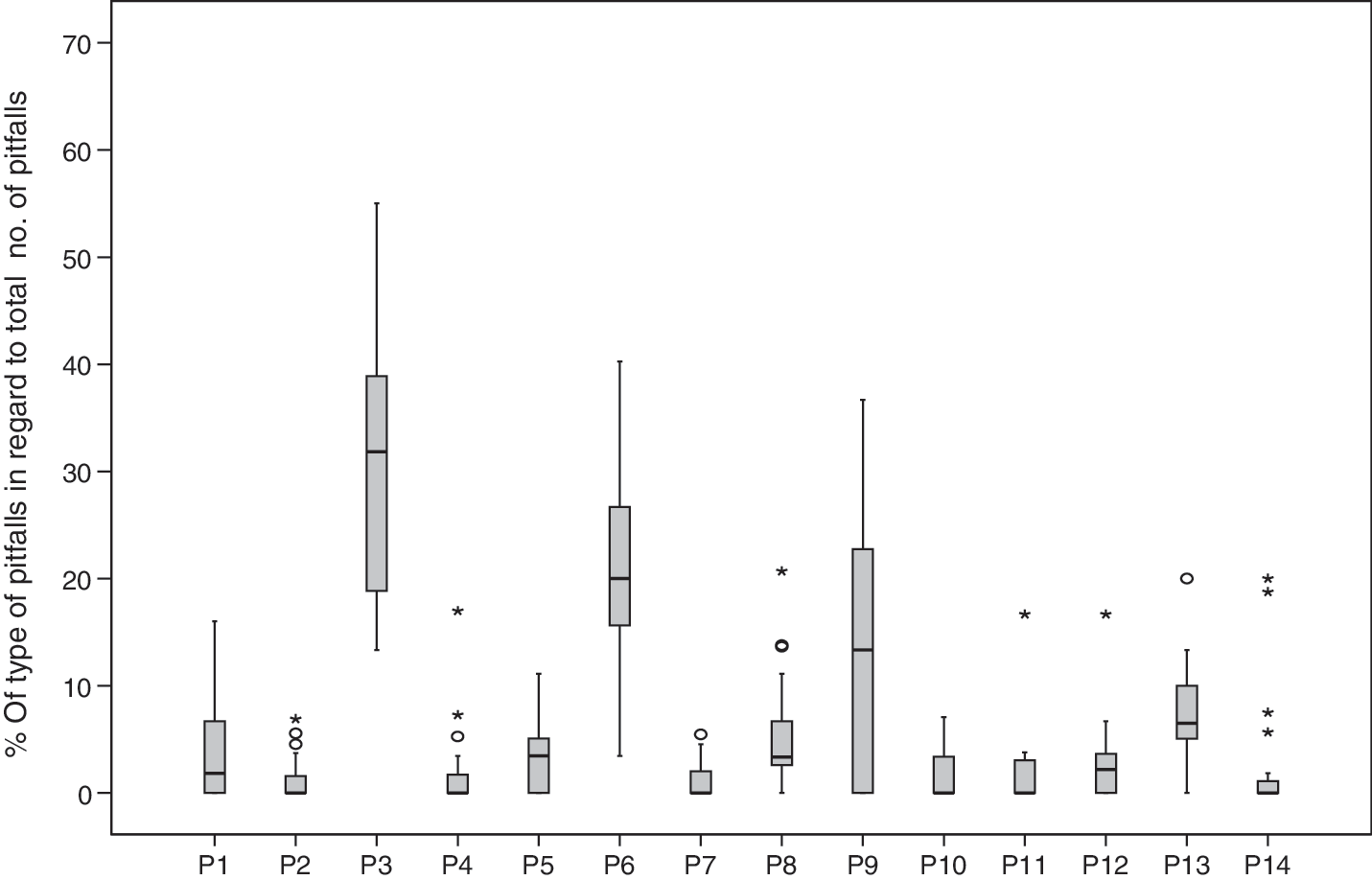
Frequency of type of pitfalls—ureterorenoscopy. For description of pitfalls P1 to P16 see Table 1.
Discussion
The results of this study indicate that planning/anticipation on new situations and handling of instruments are the predominant pitfalls in all three transurethral procedures. This suggests that training model developers should pay particular attention to these factors. Additionally, simulators should be able to train irrigation management for TURBT, depth of resection for TURP, and timing of usage of X-ray for URS.
Nowadays various urological simulators have been developed to train (parts of ) the TURBT, TURP, and URS procedures. 10,15 Planning/anticipation on new situations can sometimes be trained on these simulators to a certain extent, provided that residents are taught and supervised by an expert. Additionally, most simulators only provide a limited number of training modules. An advantage of (animal) box trainers is that real-time instruments are used to learn how to handle the instruments, whereas the training options of virtual reality simulators are frequently restricted to the use of virtual reality instruments. A model for training TURBT has been described where the trainee can manage the infusion, but this model is limited by the fact that it uses pig cadaver bladders, which have a smaller capacity than human bladders and lack the possibility of bleeding. 27 Most existing TURP simulators are virtual reality simulators, 3,13,28,29 which are generally limited by providing no or unrealistic haptic feedback. 30 This means that the depth of the resection is often difficult to train on these simulators. Further, in reality, the depth of the resection is often evaluated by judging the appearance of fatty tissue instead of prostate tissue. This is an aspect of real-time procedures that is often not integrated in simulator images. One URS virtual reality simulator enables the use of X-rays, 31 and URS box trainers enable the use of normal X-ray equipment, if available.
The results of this study provide insight into the pitfalls that the residents are likely to encounter when performing procedures in the OR and this insight can be used to improve programs to train the performance of procedures outside the OR. Additionally, the information on the pitfalls provided by this study may be helpful to optimize the teaching process inside the OR too. Supervisors' awareness of the most common pitfalls can lift their teaching to a higher level of quality and efficiency. It would be worthwhile for further studies to focus on ways to improve the master-apprentice type of training in the OR, as this will always be an essential component of the process of mastering operative skills. Further, it would be interesting to investigate whether “task deconstruction” 32 (splitting the procedure in parts so that the resident performs in order from easy to difficult) in real-time procedures would influence the amount and type of encountered pitfalls.
In literature, motor skills are sometimes divided into four different types of skills: cognitive (thought processes), perceptual (interpretation of presented information), motor (movement and muscle control), and perceptual motor (integration of thought, interpretation, and movement skills). 33,34 In this observational study the whole procedure was evaluated, also including pitfalls other than motor skill pitfalls, such as positioning the patient. Therefore, the division into four types of skills was not applicable in this study. However, in future experimental studies aiming at teaching and training procedures, usage of this classification of skills would be worthwhile.
One of the limitations of this study is that supervisors may differ in their opinions on the appropriate methods to perform a certain procedure and residents generally learn their operative skills from different urologists in different hospitals. This may have resulted in an interaction and pitfall being recorded during a procedure supervised by one urologist, whereas supervision by another urologist might not have led to an interaction or pitfall at that moment in the procedure.
Interaction and pitfalls cannot be analyzed without interpretation. Although this study aimed at objective classification of pitfalls, it cannot be ruled out that subjective aspects have played a role. To counteract this, the analysis and classification were performed by an observer who had been present in the OR as well as by another observer who had not been present in the OR. Interrater agreement was satisfactory (0.7) and any disagreements between the observers were resolved by discussion.
Specialists (and probably residents as well) are known to overestimate their own performances when asked to indicate the scope of their experience. 35 A limitation of this study may be that residents overestimated the number of procedures performed, when asked to indicate the amount of previous experience.
Conclusion
The results of this study indicate that in urology training, attention should be paid to planning/anticipation on new situations and handling of instruments while performing a procedure. Further, training programs need to focus on irrigation management for the TURBT procedure, depth of resection for TURP, and timing of usage of X-ray for URS. The models and simulators that are currently available offer only limited possibilities for training in these areas.
Footnotes
Acknowledgments
The authors thank the urologists and residents from the Canisius Wilhelmina Hospital, Catharina Hospital Eindhoven, and VU University Medical Centre who were willing to participate in this study. The authors also thank Mereke Gorsira for her editorial assistance.
Disclosure Statement
None declared.
Abbreviations Used
Presented in part at the American Urological Association Annual Meeting, Chicago, Illinois, 2009.