
Abstract
Purpose:
The aim of this study was to evaluate the safety and efficacy of subcostal upper pole (UP) access in complete supine percutaneous nephrolithotomy (csPCNL).
Materials and Methods:
From July 2008 to February 2009, we performed 20 PCNLs in complete supine position. We present our experience of percutaneous approach in complete supine position to the renal superior calix, while insisting on renal displacement technique to facilitate the puncture of the superior calices and to decrease intrathoracic morbidity. The renal displacement technique was carried out with lung inflation.
Results:
The percutaneous subcostal access of the renal UP was performed in 20 cases and no failure occurred. The overall stone-free rate was 85%, and the stone-free rate for upper calix was 95%. The mean operative time in our study was 102.25 ± 41.56 minutes. The mean hospital stay was 92.4 ± 30.43 hours. The transfusion rate as a complication was 1 (5%), and no intrathoracic complication was noted.
Conclusions:
The renal UP percutaneous access can be performed using several techniques. The superior calix was accessible in csPCNL with the renal displacement technique (lung inflation) subcostally while intrathoracic complications may be avoided. UP puncture in csPCNL with this technique was associated with minimal morbidity and avoids the need for a supracostal puncture, and the stone-free rate appeared to be more.
Introduction
PCNL is considered the treatment of choice for large kidney calculi based on superior outcomes and acceptable low morbidity. 4 Recent advances in instrumentation and technique have improved the factors, including stone-free rates, increased treatment efficiency, and decreased morbidity, therefore favoring PCNL. 4,5
Upper pole (UP) access can be achieved via both supracostal and infracostal approaches. 6 UP access is achieved via a supracostal puncture, and it is used in about a fourth of patients undergoing PCNL. 7 –9
The indications for UP access for PCNL are staghorn calculi, large upper caliceal calculi, calculi in anomalous kidneys (such as horseshoe kidney), calculi in special anatomy such as that seen in morbidly obese patients, and large upper ureteral calculi. 6,7,10 –12 Also UP access is preferable when access to the ureteropelvic junction is necessary, as in patients with proximal ureteral stones, or if an antegrade approach is planned to treat ureteropelvic junction obstruction with or without associated calculi. 7,13,14
Percutaneous access to the UP of the kidney is being performed with increased frequency but it carries the risk of potential pleural or parenchymal lung injury. 15 Patients with a supracostal nephrostomy tube (NT) typically have more discomfort and pain postoperatively than patients with an infracostal NT. 8,9,16 Because of the normal anatomy of the kidney, pulmonary complications are more common with the supracostal approach. 6,11,17
Complete supine PCNL (csPCNL) is a valuable treatment option for kidney stones with complications and stone-free rate approaching that of prone PCNL. PCNL in the complete supine position is safe, effective, and suitable for patients. 4 After this study, we performed all PCNLs in complete supine position.
We performed csPCNL with subcostal UP puncture and found that the kidney is situated lower than prone position, and in this position the access to the UP can be feasible and with less complications.
Materials and Methods
An analysis was performed in 20 patients who underwent PCNL between July 2008 and February 2009. We retrospectively audited all the patients requiring UP puncture during csPCNL over a 9-month period.
Out of the 20 patients in our study, 5 patients had staghorn stones, 5 had upper caliceal stones, 4 had middle and upper caliceal stones, and 6 patients had upper caliceal and pelvic stones.
Exclusion criteria were all of the criteria excluded in supine procedure such as uncontrolled coagulopathy, age < 12, pregnancy, and immunosuppression.
Preparation evaluation included laboratory tests, intravenous urogram, ultrasound, and computed tomography scanning if it was needed. Before PCNL, the urine culture was obtained, and if positive appropriate antibiotics were administered. We used general anesthesia for all the patients. We placed the ureteral catheter for opacification or saline injection.
All the patients were placed in complete supine position without flank elevation.
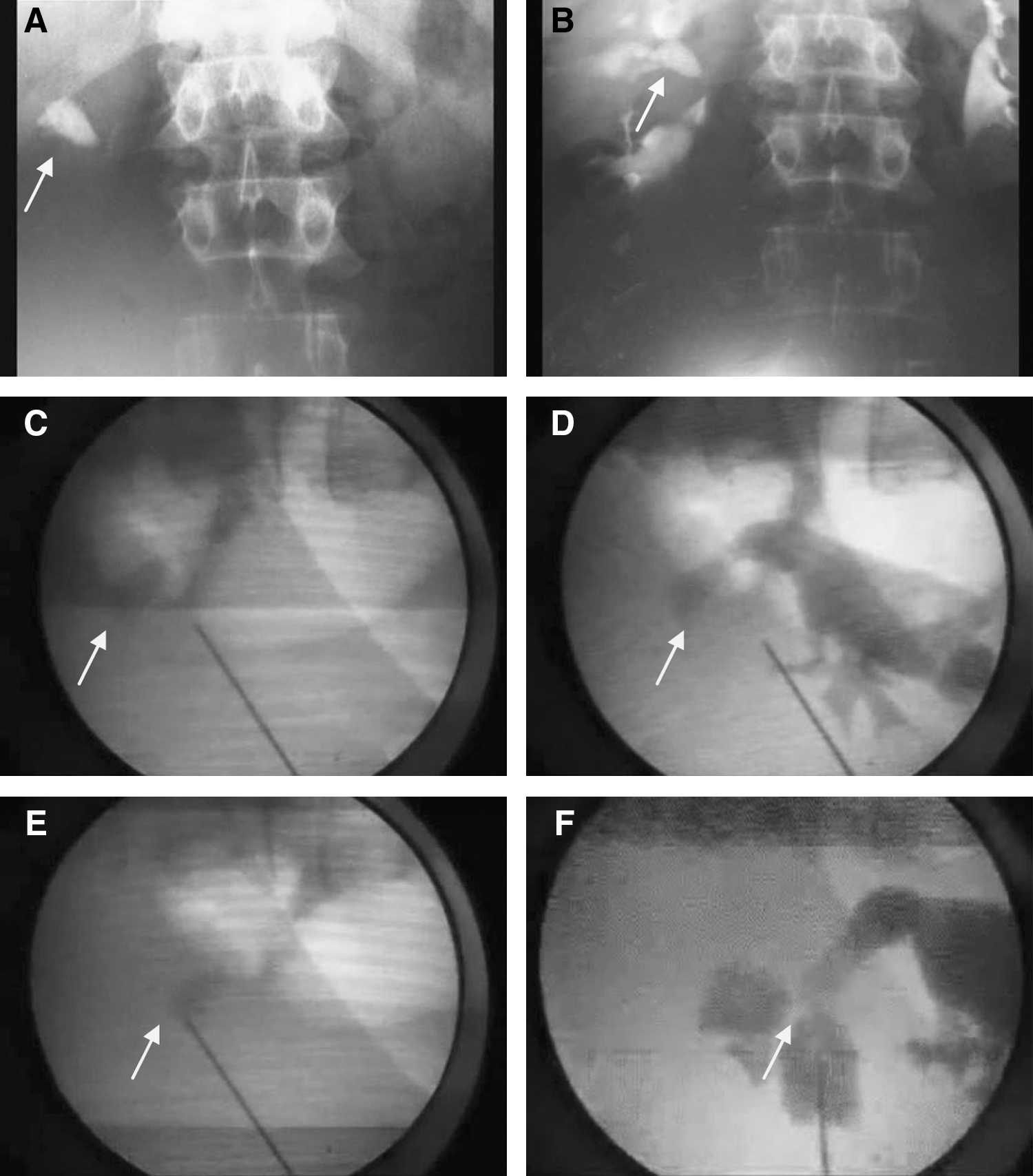
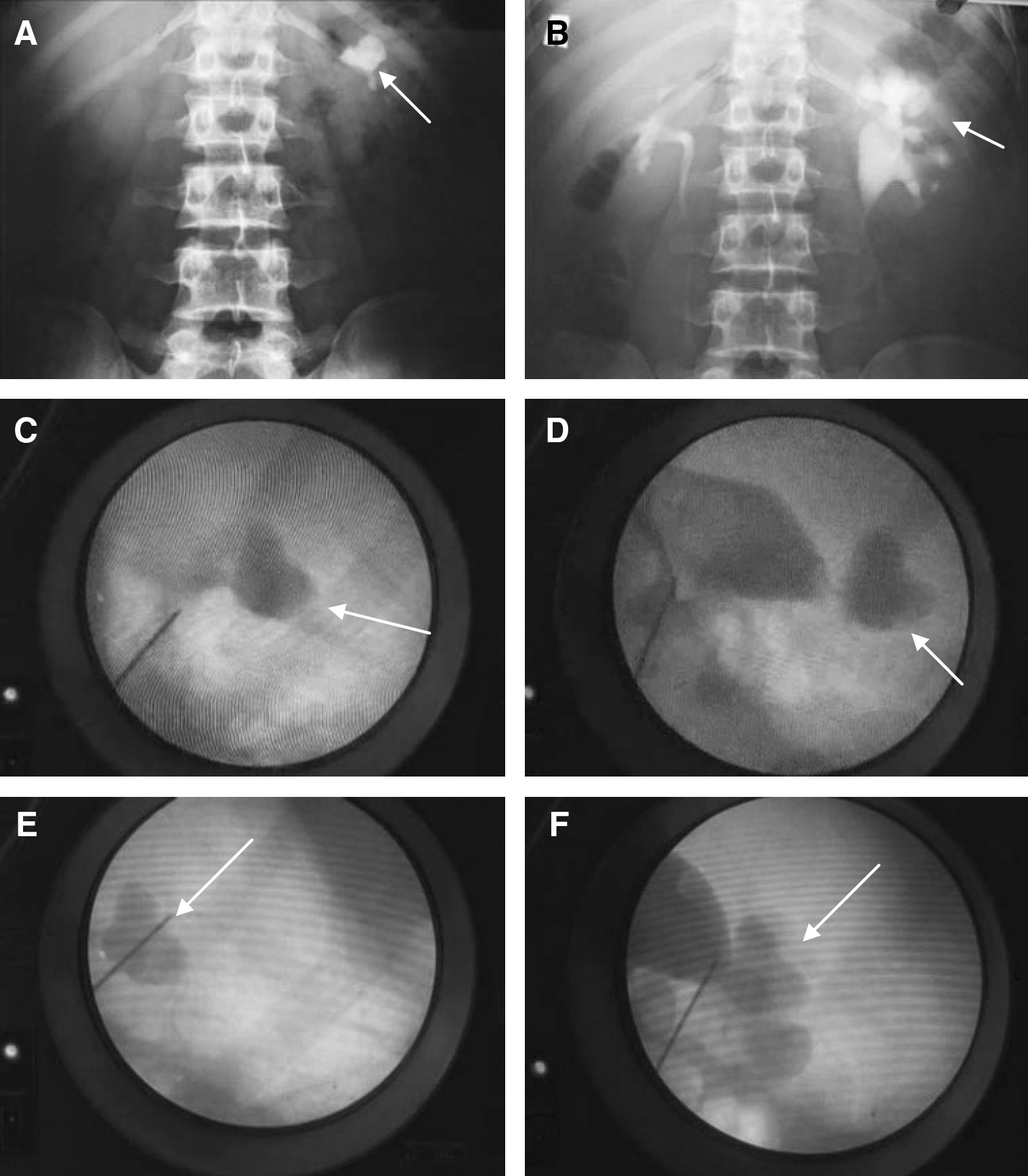
The patients in supine position were placed at bed edge. The bed edge in our hospital (Razi hospital) did not have any defect. We achieved collecting system puncture by an 18-gauge needle under fluoroscopic guide from posterior axillary line. The target was the stone. Our access was subcostal. For accessing the upper calix, while anesthesiologist inflated the lungs, the kidney was punctured under fluoroscopic guidance. In this maneuver the kidney was moved caudally, and the access to the upper calix was feasible, so pleural injury will be avoided, and then dilatation was performed in one shot (Figs. 1 and 2).
(
(

(
Dilatation was performed by 9F dilator. A single 28F Amplatz dilator was pulled in the Alkan guide. This single passage allowed insertion of the 30F Amplatz working sheath. We used rigid nephroscope.
Small stones were directly extracted by grasper, and large stones were treated by pneumatic devices. We defined stone ≤ 4 mm as stone-free status. Kidney, ureter, bladder radiograph was performed to detect stone-free rate on the first postoperative day. Ultrasound was performed to detect radiolucent stones and other complications such as hematoma and extravasation.
Foley catheter and ureteral stent were exited 2 days after operation.
We performed tubeless PCNL routinely, except while the surgeon was suspicious of severe bleeding, extravasations, and large residue of stone.
Results
The mean age of the patients was 45.9 ± 13.25 years. In our study, 11 (55%) patients were males and 9 (45%) were females (Table 1). The mean body mass index of the patients was 27.4 kg/m2.
SWL = extracorporeal shockwave lithotripsy.
Six (30%) patients had a history of hypertension, 2 (10%) had diabetis mellitus, 2 (10%) had ischemic heart disease, and 10 (50%) patients had no past medical history. Fourteen (70%) of the stones were on the left and six (30%) were on the right. In the 20 kidneys requiring UP puncture, there were five patients with staghorn stones, five patients had upper caliceal stones, four patients with upper and middle caliceal stones, and six patients had upper and pelvic stones. Seventeen (85%) patients had radioopaque stones and three (15%) had radiolucent ones. The mean stone size was 4.83 ± 1.93 cm. NT was placed for five (25%) patients, and 15 (75%) of them were tubeless. The mean serum creatinine level was 0.95 ± 0.23 mg/dL. Four (20%) patients had a past history of open stone surgery, 2 (10%) with a history of PCNL, and 14 of them had no history of previous stone surgery. Access to the patients with the history of previous stone surgery was not difficult. Nine (45%) patients had previous history of SWL and 11 (55%) of patients had no history of SWL. The overall stone-free rate was 85% (17 of 20), and the stone-free rate for upper calix was 95% (19 of 20). Overall stone residue was three (15%), and the stone residue of upper calix was one (5%). These patients were managed by SWL.
Transfusion rate as a complication was one (5%), and there were no thoracic complications. Fever was seen in one (5%) patient who was relieved after 24 hours. Mean operative time in our study was 102.25 ± 41.56 minutes. The mean hospital stay was 92.4 ± 30.43 hours. The mean hemoglobin level after surgery was 13.08 ± 1.68 mg/dL. The mean analgesic doses given postoperatively were 100 mg of meperidine in the patients.
We did not routinely use a chest kidney, ureter, and bladder radiograph after an UP puncture unless clinically indicated, that is, clinical suspicion of pleural or lung injury. We had no case of conversion to open surgery, deep vein thrombosis, plural effusion, pneumothorax, hemothorax, and colon injury.
The C-arm position in relation to the caliceal anatomy for UP caliceal puncture was 0 and 30 degrees. Respiratory inflation in all the patients was sufficient, and we had done PCNL in all patients using this technique.
Discussion
PCNL for the treatment of renal stones and other related renal diseases has proved its efficacy. 4,18 PCNL has replaced open surgery as the treatment of choice for large, multiple, and staghorn renal calculi. 1,19
PCNL in the complete supine position is safe, effective, and suitable for patients, and also access to upper calices in this method with subcostal approach is easy. 4
The indications for UP approach are staghorn calculi, large or multiple upper caliceal or ureteral stones, calculi associated with ureteropelvic junction or upperureteral pathology, and calculi in anomalous kidneys. 6,10,11
Renal displacement technique in UP access makes the superior calix accessible while avoiding intrathoracic complications, but is effective only when the kidney is mobile. 20 We used tubeless PCNL routinely as a safe and effective procedure, but it should be avoided in those with significant hemorrhage, perforation of the collecting system, a large residual stone burden, or ureteral obstruction. 21
Subcostal approach to upper calix in the prone PCNL in another our study was more difficult. 21
The reported complication rate during PCNL varies from 3% to 18%. 1,22,23 In our study, transfusion as a complication was one (5%), and fever was seen in one (5%) patient who relieved after 24 hours, but there were no other major complications such as failed access, thoracic complications such as pneumothorax or pleural effusion, and injury to other organs. No pulmonary injury because of the subcostal access was seen. In the study by El-Assmy et al, 1 the overall complication rate was 6.6%, in the reported range that was similar to our study. Shoma and colleagues 24 reported a bleeding rate of 9% in patients in the supine position. The blood transfusion rate in the current series (4.8%) was similar to the rate of between 1% and 10% reported in PCNL cases overall. 7,13,25
The risk of blood transfusion after PCNL was influenced by many factors including operative technique, patient status, and stone complexity. The number of punctures has also been incriminated in the occurrence of vascular injuries in some series. 1,26
In previously published reports, an increased incidence of colon injury during PCNL was observed in the presence of colonic distention because of the previous intestinal bypass surgery, female sex, elderly, thin patients, the presence of a horseshoe kidney, and previous renal surgery. The incidence of colonic injury was also greater on the left side, with a lower caliceal puncture, and with an extreme lateral origin of the percutaneous puncture. 1,22,27 In our study no patient had a colonic injury. The colon floats away from the kidney when the patient was in the supine position; this makes the colon less likely to be injured by a puncture made in the posterior axillary line. 28
In the study by El-Assmy et al, 1 pleural effusion occurred in two patients and all had supracostal access, which gives a thoracic complication rate of 1.4% in patients undergoing supracostal access. Young et al 29 reported a 4.2% rate of significant thoracic complications in a series of 24 intercostal nephrostomies. Also in a larger series of 167 supracostal punctures performed by one urologist, Lashley and Fuchs reported 9.5% significant thoracic complications. 30 But in our study with subcostal access, we had no thoracic complications; this result was dependent on the subcostal access. In our technique, while the anesthesiologist had inflated the lungs, the kidney was displaced caudally, subcostal puncture under fluoroscopic guidance was performed by the surgeon, and UP access was achieved, so that pleural injury could be less.
Reported stone-free rates in the study by Rana et al for larger (staghorn) and complex calculi are good, with up to 87% stone clearance. 18 The overall stone-free rate in the study by El-Assmy et al 1 was 85.1%, which is in the range reported by Stening and Bourne, 10 and they are similar to our study where it was 85% (17 of 20). The stone-free rate for upper calix was 95% (19 of 20). In the study by Wong et al, 3 after the first PCNL, the mean hospital stay was 2 days (range 1–10 days). In the event a second PCNL was required, only 1 or 2 additional days (including the day of surgery) of hospitalization were required. In the study by Raza et al, 11 the median hospital stay was 5 days but in our study the mean hospital stay was 92.4 ± 30.43 hours. The mean operative time in our study was 102.25 ± 41.56 minutes which was less than the results obtained by Neto (mean time 162.1 minutes). 5
To the best of our knowledge there is only one study about csPCNL. 4
We performed PCNLs in complete supine position without any towel under the patient's flank and with no change in leg position. Access to upper calices in this method was easier than the prone position. The irrigation fluid fall on patients was low, so the rate of hypothermia was lower. Anterior kidney displacement in complete supine position was less than modified supine position. 4 In our study, subcostal access with renal displacement makes the superior calix accessible while avoiding intrathoracic complications.
Upper access was achieved intercostal routinely, which was accompanied with more pulmonary complications. In csPCNL, subcostal access to the upper calix was feasible, so that pleural injury can be less. UP PCNL with subcostal approach seemed to be a new valuable treatment option for complex stone disease and had less thoracic complications.
Although supine PCNL has numerous advantages and is routine in some surgical centers throughout the world, its popularity in the field of urology, as a whole, is still minimal. This lack of general acceptance most likely stems from the fear of colonic injury during this procedure and also a deficiency in the training of supine PCNL in educational centers.
This study is the preliminary one and need further studies with more cases for evaluation.
Footnotes
Disclosure Statement
No competing financial interests exist.