
Abstract
Throughout history, medicine has witnessed paradigm shifts that significantly change patient treatment. In surgical oncology, the introduction of lumpectomy revolutionized breast cancer treatment while partial nephrectomy has altered the management of kidney cancer. In both cases, organ preservation is combined with efficacious management of the cancer via a less invasive approach. Within urology, prostate cancer (PCa) may be the next to benefit from such a treatment paradigm. Current management of PCa involves either whole organ treatment, with the inherent side effects, while selected patients are eligible for active surveillance. Focal therapy offers a middle ground for low-risk patients with PCa, again using the principles of a minimally invasive treatment of the cancer, in this case using an energy source with few side effects, combined with maximal organ preservation. Because focal therapy for PCa is still in evolution, there is no consensus on the ideal energy source that should be used to ablate the PCa, imaging to monitor the tissue destruction in real time, how many treatments may be offered, and the ideal follow-up regimen. Long-term follow-up of patients is needed before it is recommended as a first-line treatment. Nevertheless, evidence is accumulating that radically treating PCa holds survival benefit for patients; however, the number of men needed to treat is considerable, with significant side effects; thus, more centers are investigating focal therapy as an option. This review focuses on the use of the laser as the energy source for focal ablation, while bringing historically relevant information regarding laser energy and highlighting the perceived advantageous of focal laser ablation.
Focal Therapy as a Treatment Strategy in Prostate Cancer
With current trends of prostate-specific antigen (PSA) screening and the lowered PSA threshold for biopsy, 45% to 85% of patients fall under the category of low-risk prostate cancer (PSA < 10 ng/mL, Gleason 3 + 3, clinical T1c–T2a). 3 –5 It is estimated that 25% to 84% of patients with PCa who are currently being treated will not succumb to their disease should they be left untreated; thus, this is known as insignificant disease. 6 –11
Although we risk overtreating a large subset of patients, proponents for active treatment have evidence from the Scandinavian trial. This demonstrated a decrease in cancer-specific mortality for patients who underwent radical prostatectomy (RP) rather than watchful waiting (12.5% vs 17.9%) and an increase in survival without metastasis (76.9% vs 54.4%) 7,12 The European Randomized Study of Screening for Prostate Cancer has also demonstrated a 20% reduction in PCa disease-specific mortality for patients who were screened and treated with whole-gland radical therapies. 13 All available whole-gland treatments, however, exert a significant negative impact on patient health-related quality of life (QoL). 14,15
To combat potential overtreatment of clinically insignificant cancer, active surveillance (AS) has emerged as an alternative management strategy. 16 Patients who are suspected of having insignificant PCa based on physical examination, PSA levels, and transrectal ultrasonographic-guided biopsy (TRUS-BX) results are actively monitored, with radical treatment offered when suspicion of progressive or life-threatening clinically significant disease emerges. Such information is based on repeated physical examinations, PSA (rise or kinetics), and TRUS-BX. Thus AS offers curative treatment to patients who we suspect ultimately need it while it avoids inflicting unwanted side affects in patients who do not need treatment because of insignificant disease. 16
Although AS is theoretically appealing, data are emerging that suggest a considerable proportion of patients offered AS may indeed be harboring significant PCa. In a series of men who were offered AS with selective delayed therapy, a large number of those patients who ultimately underwent RP were found to have advanced disease. Extraprostatic extension occurred in 58% while 8% had nodal disease. 17
Individual risk of disease progression is difficult to assign, so of concern is a small but real possibility of progression to death in the AS population because of the loss of opportunity for cure during the surveillance period. Further, although AS may appear to have no morbidity, several studies have shown deterioration of QoL 18 –20 and even deterioration in sexual function. 21,22 Finally, although AS has gained popularity, it is still infrequently used. In the United States, approximately 10% of eligible men are put on AS protocols, 23 and even in countries where AS is largely accepted, only 30% of eligible men are on AS. 24 Patients and/or their physicians appear to want to treat the PCa once diagnosed.
Currently, the accepted options for treating patients with low-risk PCa lie between radical whole-gland treatment (surgery, external-beam radiation, or brachytherapy) and AS. Each has merits and disadvantages. Focal therapy is different and may be likened to a lumpectomy in breast cancer where only the diseased part of the organ is targeted with minimal impact on the surrounding normal organ. Hence, Onik 25 coined the term “male lumpectomy” for focal ablation of PCa.
Certainly, one may consider focal therapy as a logical extension of the AS concept; it has a low risk for lifestyle-altering complications associated with whole-gland treatment but also aims to achieve cancer control at the outset. This is possible because PCa, although multifocal in a majority of cases, is considered to have an index cancer, 26 which is the one most likely to cause extraprostatic extension and ultimately disease spread. Focal therapy relies on imaging to identify such a clinically threatening index cancer and treat it, and in doing so minimize the risk of progression associated with expectant management in AS patients.
At present, three major energy sources have been used in focal therapy: Cryoablation, 25,27,28 high-intensity focused ultrasound (HIFU), 29 and laser ablation. 30 We will now outline the physiology behind laser ablation and emphasize the advantages and disadvantages in using laser energy to perform focal therapy for PCa.
History of the Laser
Laser is an acronym for Light Amplification by Stimulated Emission of Radiation and was under legal dispute as to its origins, but Gordon Gould in 1957 is now credited. The basic process involves exciting a particular material by an external source (light, electricity, chemical reaction). The material is placed between two mirrors that act as an optical resonator, which intensifies the interaction between the electromagnetic field and the excited material (amplification). Making one of the mirrors partly transparent allows the resulting laser beam to exit the resonator. Depending on the material used, a different wavelength will be generated.
Laser radiation has three important characteristics: It is coherent (the wave trains are exactly in phase), it is collimated (the beam is parallel), and it is monochromatic (all the photons have the same wavelength, frequency, and energy). Albert Einstein theorized about a laser in a 1917 publication on quantum theory that postulated the phenomenon of extremely focused light beams. The first principle of quantum theory postulates that light travels in packets of energy known as photons. The second principle postulates that most atoms or molecules exist in a low-energy-state. It is possible to add energy to atoms in the ground state to convert the majority of low energy atoms to higher energy levels. The energy then is released spontaneously in the form of photons or electromagnetic waves to return to the ground state. Einstein also postulated that when a photon of light energy of the same wavelength strikes an excited atom, that photon and the photon of light that is released are discharged simultaneously and therefore will be identical in frequency and phase. This is the concept of stimulated emission used in the creation of a laser.
The physical aspects of a laser system are dictated by its wavelength, and the wavelength of the laser is dictated by the source that is being excited. The first commercial laser built in 1960 by Maiman 31 used a synthetic ruby as a source of excitation. The first generations of lasers used various forms of gas as excitation mediums such as N2–CO2 and helium-neon. The second generation of lasers used liquid materials as forms of excitation and are called dye lasers because they use an organic dye as the excitation medium, usually as a liquid solution. Compared with gases and most solid state lasing media, a dye can usually be used for a much wider range of wavelengths. The wide bandwidth makes them particularly suitable for tunable lasers and pulsed lasers. Moreover, the dye can be replaced by another type to generate different wavelengths with the same laser, making dye lasers very versatile. In addition to their recognized wavelength agility these lasers can offer large pulsed energies or very high average powers. 32
In 1970, the first continuous-wave dye laser, being argon pumped, was developed. The output of a laser may be a continuous constant-amplitude output (continuous wave) or pulsed, In the pulsed mode of operation, the output of a laser varies with respect to time, typically taking the form of alternating “on” and “off” periods. This application facilitates the depositing of as much energy as possible at a given place in as short a time as possible.
The medical field was quick to realize the possibilities in laser energy; only 3 years after the first commercial laser was built, McGuff and associates 33 reported on the effect of a ruby laser on melanoma cells transplanted in hamsters. Many more studies that examined the use of laser energy for treating patients with cancer soon followed. 34 –38 Laser energy was quickly adapted for tissue welding, coagulation, and importantly, tissue ablation. 39 –41
Focal Laser Ablation
The term laser ablation refers to the thermal destruction of tissue by laser. There are differing names for laser ablation, including photothermal therapy, laser interstitial tumor therapy, and laser interstitial photocoagulation. 42 The term interstitial laser ablation reflects the fact that the laser fiber is inserted into the tissue as opposed to ablating tissue with a laser while maintaining a buffer medium between the fiber emitting the energy and the tissue being ablated (eg, air for cutaneous application, saline when applying laser energy in the bladder/ureter). We prefer the term focal laser ablation (FLA) when referring to the treatment of PCa as it describes the intention and the treatment.
Interstitial laser ablation was first described by Bown in 1983. 43 He inserted a 400 μm glass fiber into a metastatic skin lesion and, using an neodymium:yttrium-aluminum-garnet (Nd:YAG) laser system and deploying a bare fiber, caused local necrosis in the treated area The basic principles behind laser ablation are the conversion of laser light into heat by tissue. The optical and thermal properties of the tissue as well as the parameters of the laser beam influence the extent of the thermal ablation. The optical and thermal properties of the tissue are determined by the structure, water content, and blood circulation. The key concepts are absorption, scattering, reflection, thermal conductivity, and heat capacity.
The prostate as a tissue is suited for FLA because of its optical absorption rate without excess vascularity, which causes heat conduction and limits the ablation size when performing FLA in highly vascularized tissues such as liver.
The laser beam properties are governed by the wavelength, power, and density. The main absorption of biologic molecules occurs within the range of a wavelength shorter than about 280 nm (ultraviolet). The penetration of light is optimal at wavelengths longer than 1 μm (the near-infrared range of the spectrum). The high water content (60%–80%) of most tissue leads to an extensive absorption of infrared radiation and thus to a very efficient energy transfer and heating of the tissue when irradiated with lasers of these wavelengths (eg, CO2 laser).
Evidence is accumulating that laser energy penetrates tumor cells better than normal tissue 44 and thus enables larger coagulation zones in tumors. The laser most commonly used for FLA is the Nd-YAG laser, with a wavelength of 1064 nm, but it is being replaced by more compact and less expensive infrared (800–980 nm) diode lasers. The delivered photons induce an increase in temperature. Local tissue temperatures above 60°C cause rapid coagulative necrosis and instant cell death, but irreversible cell death can also be achieved at lower hyperthermic temperatures (>42°C), although longer durations are necessary. 45,46 Temperatures above 100°C will cause vaporization of cellular protoplasm, followed by desiccation and shrinkage of the tissue; afterward, any additional laser energy causes a quick temperature rise, and temperatures above 300°C cause the tissue to burn and carbonization occurs.
Since the first deployment of interstitial FLA in 1983 by Bown, 43 many modifications have been made. The application of the laser beam via flexible quartz fibers of diameters from 250 to 1000 μm allows FLA through flexible fiberoptic devices and through thin needles.
The use of specially designed interstitial fiberrs, which are quartz fibers that have flat or cylindrical diffusing tips and are 10 to 40 mm long, provide a much larger ablative area of up to 50 mm.
Increasing laser power output in newer lasers allows for better light transmission and larger ablative zones. It also causes increased local temperature rise close to the laser fiber, however, risking overheating and carbonization of the adjacent tissue. Carbonization of tissue decreases optical penetration and heat conduction and limits the size of the lesion produced.
To limit such events and to prevent overheating close to the fiber tip, water-cooled laser application sheaths are being used. They allow for higher laser power output (up to 50 W compared with 5 W) while preventing carbonization. 47,48 Thus, the use of multiple water-cooled higher power fibers allows ablative zones of up 80 mm in diameter.
Perhaps the most exciting innovation is the ability to monitor in real time the lesion created by the laser using imaging techniques, such as magnetic resonance (MR) thermometry and contrast-enhanced ultrasonogrphy (CEUS). Because FLA is highly compatible with MR and does not cause any electromechanical disturbances, the use of MR thermometry allows for real-time monitoring of lesion size and allows for individually adjusted heat dosing application ensuring adequate tumor ablation while avoiding damage to nearby vital structures. CEUS is well suited for FLA as well; because the thermal effects created by the ablation reduce blood perfusion significantly, there is no uptake of microbubbles in the ablated area. Thus, the treatment effect in tissue is evident by the absence of CEUS signal, with obvious delineation between viable and nonviable tissue (Fig. 1). 49
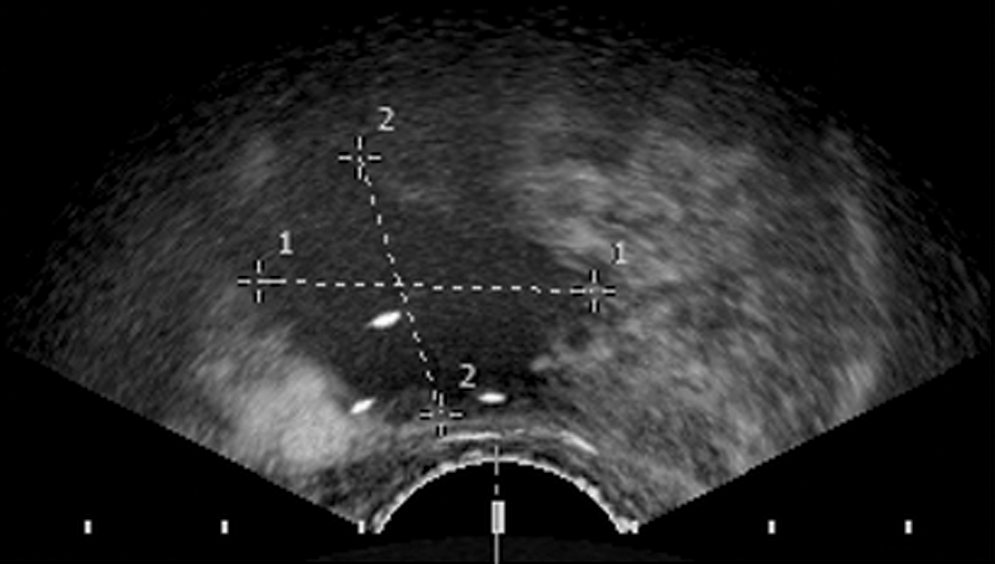
Contrast enhanced ultrasonographic image shows an ablation real time.
Focal Laser Ablation for Tumors Other than the Prostate
Ever since the advent of FLA in 1983 by Bown, 43 there have been numerous studies regarding the effectiveness of FLA for tumors (eg, unresectable liver metastasis and inoperable hepatocellular carcinoma [HCC] treatment). In a large nonrandomized study, Vogl and colleagues 50 treated 1801 colorectal cancer liver metastasis in 603 patients with MR image-guided FLA. Local tumor control rates of above 96% at 6 months based on MR imaging were achieved, with an overall complication rate of 1.5% and a 30-day mortality of 0.1%. No tumor seeding was noted, and a median survival of 4.4 years after diagnosis of metastases was achieved, being superior to the 17.4 months median survival after receiving chemotherapy alone.
Several contemporary studies of outcomes of FLA for inoperable HCC have achieved acceptable complete ablation rates of 82% to 97.5% with tumors smaller than 3 cm, and from 60% to 82% in tumors 3 to 4 cm. 51,52 Mortality is very low considering the patient population at 0.1% to 0.2% and major complications around 1.5%. 51,52 When compared with radiofrequency ablation and HIFU, FLA was shown to be equivalent and less morbid. 53
In summary, FLA has been performed on a variety of different tumors with encouraging results (Table 1) and is gaining popularity as an image-guided, MR-controlled localized tumor ablation modality.
HCC = hepatocellular carcinoma; US = ultrasonography; Met. = metastases; CT = computed tomography; MRI = magnetic resonance imaging; N/A = not available; RCC = renal-cell carcinoma.
Focal Laser Ablation for Low-Risk Prostate Cancer
Currently, all the studies being published in focal therapy for low-risk PCa are nonrandomized, small cohorts, and phase I clinical trials. Focal therapy for PCa, however, appears to be gaining acceptance and holds promise for a better balance between cancer control and morbidity.
In a recent phase I clinical trial by our group, 30 we performed image-guided FLA for patients with low-risk PCa. The enabling technology for targeted FLA as opposed to hemiablation or subtotal gland ablation is accurate imaging. The ability to visualize the target, navigate an ablation tool to that target, and monitor the ablation process all in real time is crucial to perform truly focal therapy and minimize the morbidity.
PCa lesions were targeted based on multiparametric MR scans. The MR imaging served to target the tumor once diagnosis was established with standard TRUS-BX. When the location is depicted by biopsy and the tumor is visualized by MR scanning, it accurately denotes the specific location 83% of the time in the peripheral zone for tumors larger than 4 mm in diameter. 54 The tumor coordinates and contours thus obtained were then used to guide laser fiber placement by using 3-dimensional ultrasonographic guidance. CEUS with real-time monitoring of lesion size development increases the likelihood of tumor destruction (Fig. 1). Using this technique, 0.25 cm3 of PCa was targeted, creating a 2.2 cm3 well-defined region of decreased enhancement or ablated zone.
The postprocedure and morbidity were negligible. Self-limited perineal discomfort was the most common (25%) side effect and mild hematuria that did not warrant medical attention the most severe (16%). No significant drop in International Index of Erectile Function-5 scores was noted up to 6 months postprocedure. There was no worsening of urinary symptoms as assessed by the International Prostate Symptom Score and no incontinence using the strict criteria of no pads worn.
The short-term oncologic results seem promising, with no evidence of disease seen on results of postprocedure biopsy in 50% of patients and 67% free of tumor at the ablated zone. So, RP attempts to achieve the “trinity” of cancer control, continence, and maintenance of erectile function, but even in expert hands, side effects remain significant. These data on FLA suggest that there were no cases of erectile function or continence compromise and that only longer-term data in larger series for follow-up of cancer control are needed before the trinity is achieved for FLA.
Laser physics is a well-studied science. It is accurate, predictable, and reproducible and induces minimal damage outside the targeted ablation zone. It has been demonstrated to be a simple and effective means of prostate tissue destruction when used as a therapy for benign prostatic hyperplasia 55 and effective means of tumor ablation for a variety of different tumors (Table 1). One of the main advantages in using FLA in general and for PCa treatment is that lasers are highly MR compatible. MR imaging with its superb soft-tissue contrast and its multiplanar capabilities has the best visualization of the prostate and its surrounding anatomy. MR is capable of monitoring temperature change, which makes it an ideal imaging modality for real-time assessment of thermal ablation.
MR, however, is extremely sensitive to ferrous materials and electromagnetic disturbances. Although HIFU, radiofrequency ablation, and cryoablation have been used with MR, FLA is uniquely suited for MR because the off-the-shelf fibers used are made of quartz and do not cause any disturbance in the bore of the magnet. Furthermore, the energy being used is nonelectromagnetic whereas the other modalities have to undergo specific modifications to be MR compatible. Finally, the source of energy being used by devices other than laser causes electromagnetic disturbance, forcing MR scanning to be stopped or specifically modified while ablating the prostate.
Focal ablation of the prostate using energy modalities other than laser under MR guidance with real-time monitoring is being investigated but needs the development of new equipment and techniques, 56 –58 which adds further unnecessary complexity and cost to a highly technical field.
Another important or even crucial aspect of focal therapy is the ability to cause a confluent cellular ablation in the target area. In an ongoing study, Trachtenberg and coworkers performed FLA followed by RP 1 week after the FLA procedure; using a two-fiber configuration and creating three different ablation sites, they managed to create a uniform ablated zone that was verified by rigorous pathologic whole-mount sectioning every 3 mm and using both hematoxylin and eosin staining and vital staining (Fig. 2). The absence of any viable living cells in the ablated area lends to the scientific validity of FLA, which will again need to be confirmed with longer follow-up.

Pathologic confirmation of ablation. (
Conclusion
Focal therapy as a paradigm for treating patients with PCa is still in evolution, but initial evidence suggests an advantage over whole-gland radical treatments in two elements of the trinity—potency and continence. Oncologic efficacy needs considerable follow-up for PCa patients and in a large number of patients for focal therapy to be accepted as a first-line option in patients with low-risk PCa. So, there is much scientific work ahead of us to further evaluate focal therapy, including evaluating what is the preferred imaging modality to be deployed and what source of ablation energy to use.
FLA appears a promising energy modality, because lasers are readily available, relatively inexpensive, create confluent ablation zones, and can be easily monitored by both real-time MR imaging and CEUS. We believe that all these attributes will make FLA into a popular utility for focally ablating PCa.
Footnotes
Disclosure Statement
No competing financial interests exist.