
Abstract
Any focal therapy requires correct localization of the lesion; consequently, much effort is now devoted to accurate characterization of the spatial distribution of the tumor within the prostate. One of the greatest difficulties in the localization of prostate cancer is its frequent multifocality, but prostate cancer is unifocal in 13% to 43.7% of cases and unilateral in 19.2%. In cases of multifocality, it seems that the index tumor is the biologic driving force behind the malignant potential of prostate cancer. Not only is the Gleason score of the secondary nodes lower than that of the index node, but 80% of the secondary nodes are smaller than 0.5 cc and almost all extraprostatic extensions are associated with the largest cancers. While current evaluation with 12 to 18 core biopsies may be adequate to determine the index lesion, transperineal three-dimensional mapping biopsy of the prostate should be undertaken if greater accuracy is needed.
Introduction
Widespread use of the prostate-specific antigen (PSA) serum test has boosted the number of diagnosed prostate cancers and also reduced the mortality of prostate cancer. It has also, however, been the cause of overtreatment through the use of radical therapies, 1 because early diagnosis has entailed a progressive reduction in the mean tumor volume in radical prostatectomy specimens and has also raised the incidence of unilateral tumors. 2 These observations, together with a progressive improvement in conservative approaches to cancer treatment, have prompted a significant number of patients to request nonradical therapies (focal therapy) to achieve reasonable control of localized carcinomas. 3
Any focal therapy necessitates correct lesion localization. Despite the important advances in imaging techniques, they are still insufficiently precise for this purpose, 4 and consequently criteria for the selection of patients who may benefit from focal therapy remain to be defined. 5 Prostate cancer heterogeneity should also be added to the equation when selecting treatment: Quite a high percentage of cases show an indolent natural history, 6 and for this reason, a number of authors still believe that the best focal management of prostate cancer is active surveillance. 7
A lot of effort is currently being devoted to accurate characterization of the spatial distribution of the tumor within the prostate, despite the remaining limitations of and doubts about focal therapy for prostate cancer. The objective of such effort is to circumscribe the group of patients considered eligible for this therapy.
One of the greatest difficulties in prostate cancer localization is its frequent multifocality, which gives rise not only to problems in determining its topography but also to doubts over the characterization of its biology.
The purpose of this article is to review what is already known about prostate cancer multifocality to assist in determining those patients who may benefit from focal therapy.
Multifocality and Laterality
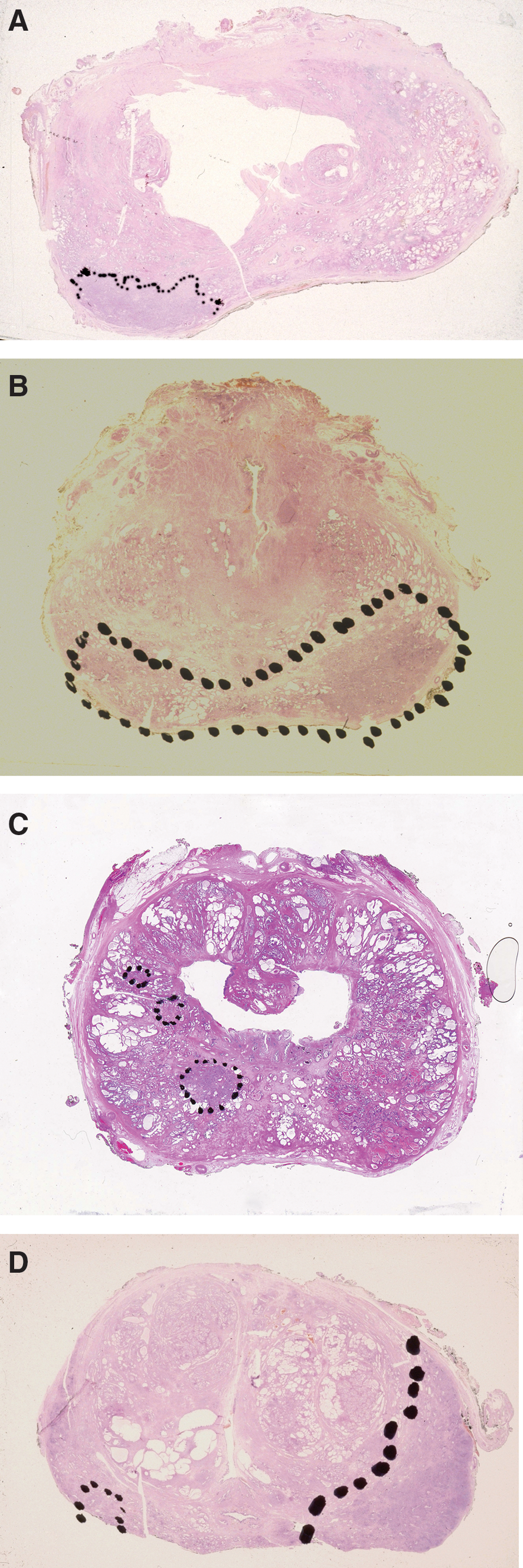
Neoplastic multifocality refers to the presence of different tumors that are separated from each other by normal tissue. The phenomenon of multifocality is not exceptional in nonfamilial neoplasias, either in extraurologic locations 8 –11 or within the urogenital tract, 12,13 but it is particularly frequent in prostate cancer. 14 To identify multifocality, however, prostatic tumor nodes should be studied in consecutive parallel sections because of their nonspherical growth pattern (Fig. 1). One issue that does not arise in the prostate is whether multiple lesions are synchronous or asynchronous, because, given the limitations of imaging diagnosis and current radical treatments, virtually all relevant studies are performed on radical prostatectomy specimens.

Consecutive parallel sections show that the apparent different nodules are a single tumor (pT2c/GS 3 + 4).
The reported incidence of multifocality in whole mount analysis ranges between 87% 14 and 56.3% 15 ; in other words, prostate cancer is unifocal in 13% 14 to 43.7% 15 of cases. These figures are quite similar to those reported for latent prostate carcinomas (62% multifocal). 16
Multifocal prostatic carcinomas show two foci in 17.3% to 31.1% of cases, three in about 28.6%, and more than three in the remainder. 14,15
One aspect that has proved to be very significant, thanks to the novel focal therapy options, 17 is laterality (Fig. 2), because focal therapy may be considered even when the neoplasia is multifocal; if it is localized laterally, the focal therapy can be considered as a radical treatment. Furthermore, completely unilateral cancer is observed in as many as 19.2% of patients. 18
(
Earlier carcinoma detection because of PSA determination has brought about a decrease in tumor volume (in 1988–1995, only 10% of patients who underwent prostatectomy showed tumor volumes ≤5%, whereas in 2001–2003, the corresponding percentage had risen to 37%). 2 The early diagnosis of prostate cancer represents an early treatment and, for this reason, a decrease in tumor volume that has been accompanied by a reduction in the number of separate tumor foci per radical prostatectomy from 7.3 to 2.9, 19 –21 and also by considerably increased unilaterality (63%). 22 All of these findings represent further arguments in favor of focal therapy.
Multifocality and Tumor Volume
Tumor volume is a long-established biologic indicator and has always referred to the volume of the main cancer focus or index tumor. 23 One also needs to address the issue of the tumor volume of the smaller nodes, however, and how it impacts on the index tumor volume. The sum of volumes of additional tumors is seldom as large as the volume of the index tumor, because 80% of secondary nodes have a volume smaller than 0.5 cc, 24 the average being 0.63 cc 25 (Fig. 3). Probably the low tumor volume of the secondary nodules can explain why the PSA failure rates (hazard ratios) were similar for the patients with only one nodule and patients with an index tumor plus secondary nodules, confirming that predictive estimates only need to measure the index tumor. 25

Multifocal, bilateral prostate cancer with a principal (index) nodule and small secondary nodules (pT2c/GS [global] 3 + 4).
Multifocality and Gleason Score
Heterogeneity of Gleason patterns in a tumor nodule lies at the basis of the guidelines regarding interobserver reproducibility, 26 –28 and a number of studies have addressed its impact on the biologic evaluation of patients. 29 –32 It is to be expected that multifocality will further increase heterogeneity of the Gleason score (GS).
Global GS in latent prostate cancer is similar in patients with unifocal and patients with multifocal tumors (GS 7–10 in 15.6% and 14.6%, respectively). 16 Observations in patients who have undergone prostatectomy, however, show some variation among observers, with some authors reporting no differences between the groups 33 while others have observed some relation of GS heterogeneity to multifocality. 14,15
Of course, there are differences between unifocal and multifocal tumor GS, but these differences do not necessarily mean that the secondary nodes add aggressiveness, because in some series, the median GS of the secondary nodes is lower than that of the index node (eg, 5.5 vs 6.4). 19 In another series, the GS of the index tumor correlated with the overall GS in 68% of cases; the primary Gleason pattern of the index tumor was the same as the overall primary pattern in 97% of specimens, whereas the secondary pattern of the index tumor was the same as the overall secondary pattern in 68% of specimens. In a further series, the percent Gleason grade 4 or 5 did not differ according to whether the tumor was unifocal or multifocal. 33
The role of the tertiary Gleason pattern is strongly debated and not recommended in the clinical evaluation, but according the 2005 Consensus Conference on Gleason Grading of Prostatic Carcinoma, the possible biologic impact (including multifocality) of the tertiary pattern is included in the evaluation in the primary and secondary system. 26
Multifocality and Stage
Extracapsular invasion is not restricted to the largest tumor in each case, but also occurs in tumors of relatively small volume. 34 When the tumor volume is quite small (<5 cc), however, the tumor is most frequently an intraprostatic one, even if it is multifocal. 22 In 92% to 100% of carcinomas, extraprostatic extension is associated with the largest cancer. 33,35
Core Needle Biopsy and Assessment of Multifocality
To what extent does core needle biopsy represent the topographic distribution of cancer in the prostate? This question is of crucial relevance when deciding uon focal therapy, yet uncertainty remains. While biopsy is the best method on which to base the selection of focal therapy,
36
it is important to recognize its limitations: A single positive biopsy has been reported to predict only laterality in 71% of cases.
37
The negative predictive value is a mere 43.6%.
38
Even though extended biopsies and even transrectal saturation biopsies have contributed to increasing the number of cancer diagnoses, they do not seem to have improved the topographic determination.
39
It is not yet known how many cores are necessary in transrectal biopsies to identify and characterize a clinically significant prostate cancer reliably, because biopsy templates have been optimized for cancer detection and not for tumor characterization. 39 Increasing the number of cores does not, in itself, seem to make any contribution to determination of carcinoma location, but a mapping stereotactic biopsy via transperineal access that is performed with the equipment and setup used in the interstitial brachytherapy procedure provides higher reliability concerning both laterality and GS. 40
In some studies, the total cancer length in needle biopsies has been found to be significantly greater in the case of multifocal tumors than in the unifocal group. 33
Multifocality and Cancer Topography
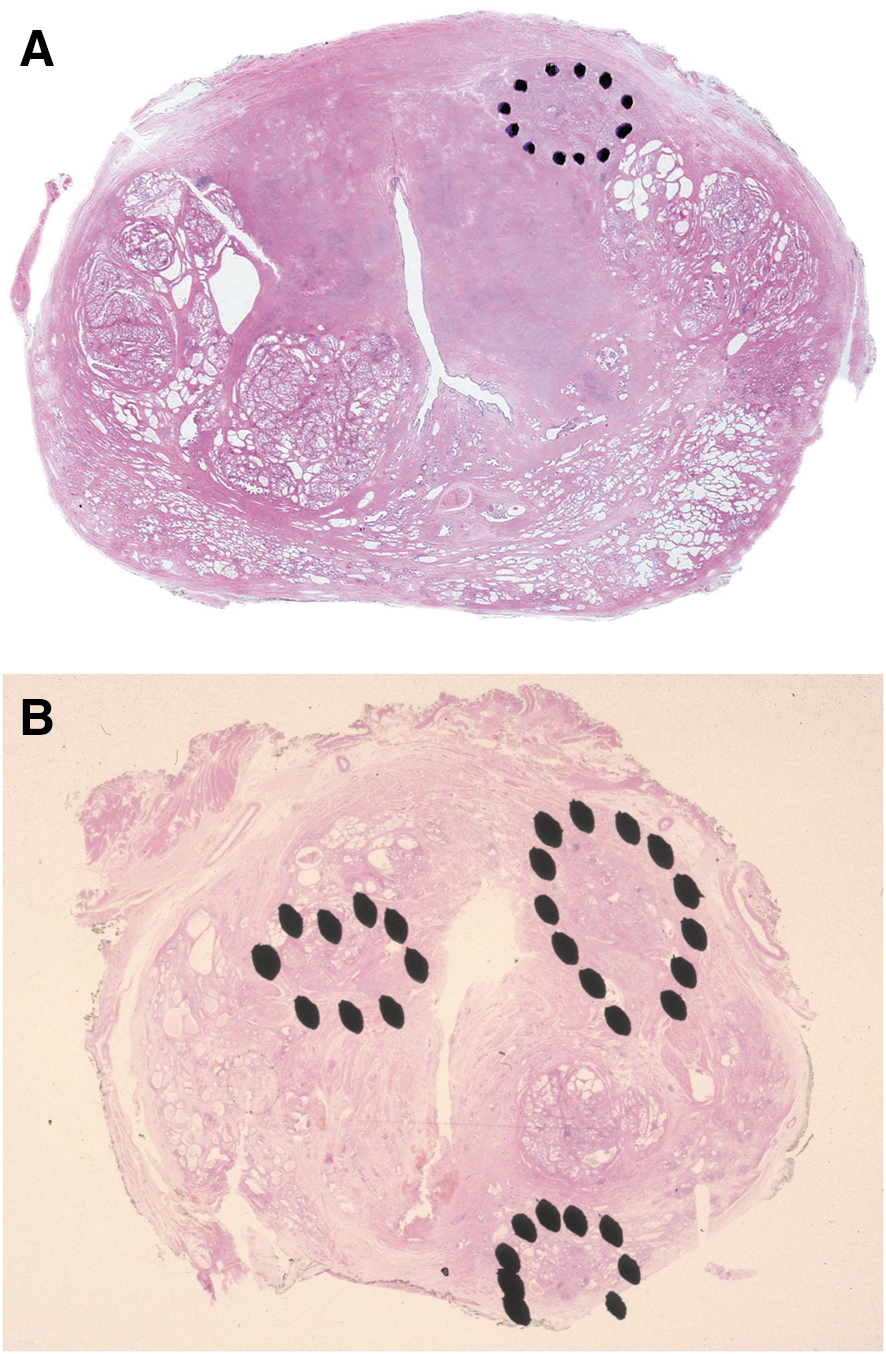
The topographic distribution of the cancer is not usually taken into account when performing radical therapy, but, as indicated above, it is very relevant to focal therapy. Most surgically treated neoplasias are located in the peripheral zone. In low-volume tumors, the most severely affected area is usually the apex, with the middle portion and the base becoming involved as the tumor volume grows. 41 The distribution also tends to be posterior; anterior growth is present in just 14% of cases (Fig. 4A), although the tumor extends to both the anterior and the posterior portion in 28%. 42 While this distribution is based on observations in low-volume tumors, 22 multifocality does not seem to alter it. 43 One study found that only 2% of specimens contained foci solely in the transition zone, and that almost all transition zone foci occurred in conjunction with peripheral zone foci and were ≤5 cc in volume (Fig. 4B). 44 One topography-related piece of information that may be relevant, depending on the focal therapy approach applied, is the distance from the tumor to the prostatic urethral mucosa. In a recent study, this distance was found to be shorter in bilateral tumors (2.4 mm) than in unilateral ones (3.2 mm). 45
(
Pathogenesis of Multifocality
The reason for the high prevalence of multifocality in prostate cancer is unknown. In one study that examined TMPRSS2 gene rearrangements, 70% of multifocal prostate carcinomas were discordant in at least one focus; for this reason, the authors considered multifocal prostate carcinoma to be a heterogeneous group of diseases arising from multiple, independent clonal expansions. 46 It is to be noted that the incidence of unilaterality is even higher in low-volume (supposedly initial) carcinomas than in carcinomas of greater volume 2 ; multifocal high-grade prostatic intraepithelial neoplasia (HGPIN) is a significant risk factor for prostatic adenocarcinoma 47 ; and the absence of HGPIN in radical prostatectomy specimens denotes a significantly lower rate of tumor multifocality. 48 These facts lead us to wonder whether HGPIN transforms into carcinoma at various foci, with these foci subsequently growing and can become larger nodes through clashing.
Conclusions
While the natural history of different prostate cancer foci remains unknown, some evidence exists that the index tumor is the biologic driving force behind the malignant potential of prostate cancer, 37 which confirms that predictive estimates only need to measure the largest carcinoma. 25 Despite their relative heterogeneity, the biologic behavior of multifocal tumors is no different from that of unifocal tumors. 16 With these things in mind, current evaluation with 12 to 18 cores may be enough to determine the index lesion when faced with a patient who is a potential candidate for focal therapy. If greater accuracy is needed, a transperineal three-dimensional mapping biopsy of the prostate 40 should be performed, obtaining a higher number of cores.
Footnotes
Disclosure Statement
No competing financial interests exist.