
Abstract

Introduction
Materials and Methods
From April 2005 to April 2006, 17 consecutive LPNs were performed. All LPNs were performed with extensive retroperitoneal dissection to completely mobilize the entire kidney. Hilar control was achieved using separate clamps on the renal vein and artery. After clamping, cold excision was performed using laparoscopic scissors. The defect was cauterized with an Argon beam coagulator. The renal tumor bed was closed, and the parenchyma was reapproximated using 2–0 Vicryl sutures with Lapra-Ty clips. A Surgicel bolster was secured to the renal defect. Next, BioGlue was applied onto the repair site with a laparoscopic applicator.
At 3 months postoperatively, a surveillance CT was obtained.
Results
About 13/17 patients received a CT at 3 months postoperatively. All 13 CTs were performed on asymptomatic patients who presented for routine surveillance. Two patients were lost to follow-up. One patient developed an arteriovenous fistula that was embolized, obscuring the CT. One patient had an oncocytoma that did not require surveillance.
All 13 CTs detected renal lesions with areas of attenuation consistent with air. A representative image is shown (Fig. 1). These lesions radiographically mimicked emphysematous pyelonephritis. We attribute the emphysematous appearance to air pockets trapped in the BioGlue seal, as seen in a sample of BioGlue placed on cardboard (Fig. 2). To confirm this radiographic phenomenon in vitro, we performed a CT of the sample, which revealed similar air pockets (Fig. 3). Review of surveillance CTs performed on patients who underwent LPN without BioGlue revealed no air pockets. A representative image is shown (Fig. 4). Of note, since May 2006, we have not used BioGlue and thus have not observed this phenomenon. Instead, we use Evicel, a human fibrin sealant, which has dual functions as a hemostatic agent and mechanical seal. Although some fluid and perinephric stranding is seen on postoperative CT as a result of inflammation, there are no bubbles with Evicel.
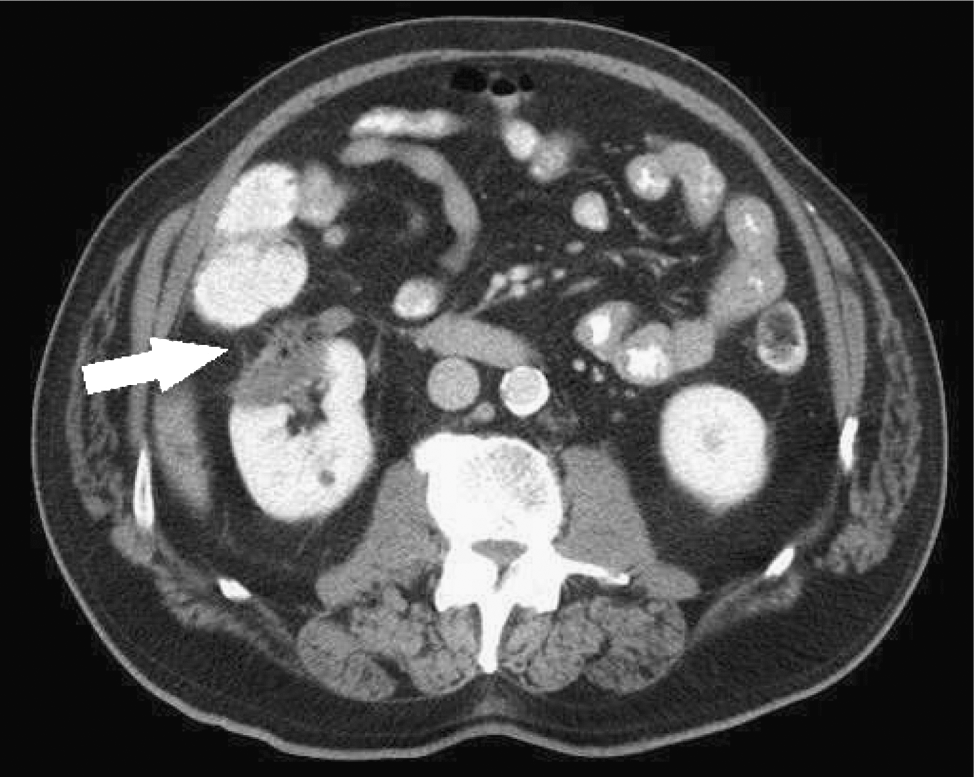
A representative CT image of a patient who underwent laparoscopic partial nephrectomy with BioGlue®. The arrow indicates the surgical defect with areas of attenuation consistent with air. CT = computed tomography.

A sample of BioGlue placed on cardboard, revealing trapped air pockets.
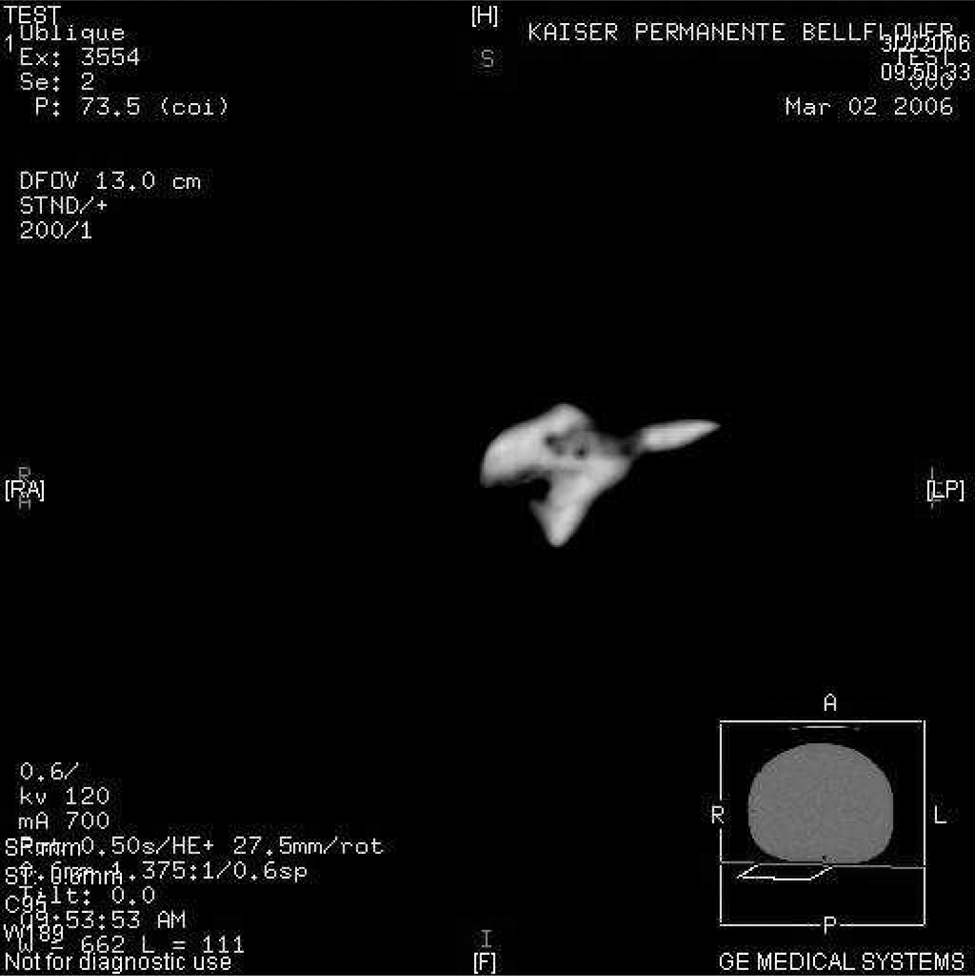
A CT image of the same sample of BioGlue seen in Figure 2 demonstrates trapped airpockets.
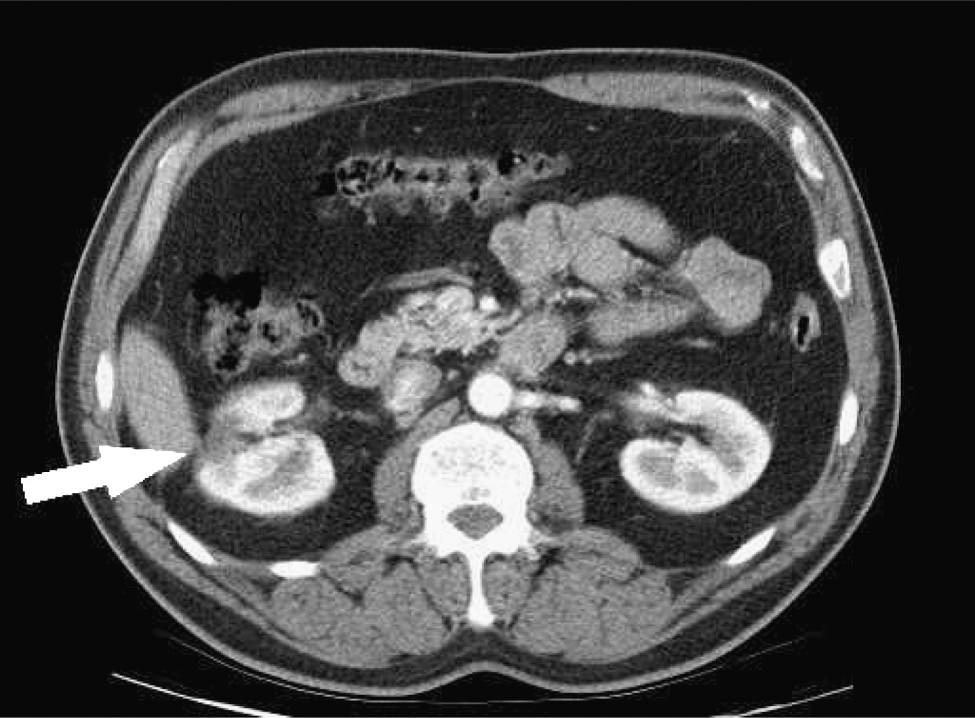
A representative CT image of a patient who underwent laparoscopic partial nephrectomy without BioGlue. The arrow indicates the surgical defect.
Conclusion
Because of its viscous consistency and its ability to harden quickly, BioGlue forms a seal around the defect created during LPN. During injection, air is invariably incorporated into the seal, and an emphysematous capsule is seen on CT. Awareness of this phenomenon can help avoid confusion during clinical interpretation of surveillance CTs.
Footnotes
Disclosure Statement
No competing financial interests exist.