
Abstract
Background and Purpose:
Ureteral stents often cause significant patient morbidity that can be difficult to treat. Drug-eluting stent technology allows the local delivery of a drug. Our previous work demonstrated that ketorolac instilled intravesically at the time of ureteral stent insertion significantly decreased flank pain compared with controls. We sought to determine the safety of a novel ketorolac-eluting ureteral stent.
Materials and Methods:
A total of 92 Yorkshire pigs were randomized to 1 of 5 groups. The oral control group consisted of 12 animals with transurethrally inserted control ureteral stents and 5 days of oral ketorolac. Twenty animals in each of the remaining groups received a control stent, or 15%, 13%, or 7% ketorolac-loaded stents. Ketorolac levels were measured in plasma, urine, and tissue sampled from ureters, bladder, kidneys, and liver using high performance liquid chromatography. Necropsies were performed to evaluate tissue pathology.
Results:
The majority of ketorolac was released within the first 30 days. The highest levels of ketorolac in plasma, kidney, and liver occurred in the oral control group. The highest levels of ketorolac found in ureteral and bladder tissues occurred in the ketorolac-stent groups in a dose-dependent fashion. No adverse events were noted in any of the ketorolac-stent groups. Gastric ulcerations were identified only in the oral control group. No abnormalities were identified in any other internal organs in any group.
Conclusions:
The use of ketorolac-eluting ureteral stents has proven to be safe in a porcine model. The ketorolac-stent group had less than 12% of the ketorolac concentration in plasma, kidney, and liver tissues compared with the oral ketorolac group. Ureteral tissues displayed the highest levels of ketorolac. Clinical studies are needed to determine if ketorolac-elution reduces stent symptoms.
Introduction
To screen potential drugs that may alleviate ureteral stent-related symptoms, patients needing a ureteral stent before shockwave lithotripsy were randomized to receive a single intravesical instillation of saline, oxybutynin, lidocaine, or ketorolac after stent insertion. 3 Stent symptoms, in particular flank pain, were significantly reduced by the administration of ketorolac compared with the other substances. Ketorolac was mechanically blended with the base polymer of the stent and this blended mixture then extruded into the stent. In this manner, the drug was uniformly distributed throughout the entire base polymer of the stent and designed to elute 1 to 4 μg/d, with the majority of the ketorolac eluted in the first 30 days after implantation. The objective of this study was to evaluate the safety profile and the drug release profiles of this drug-eluting stent in a porcine model as evaluated by tissue levels of the drug and histopathologic examination of the genitourinary system.
We sought to determine the safety profile of three different concentrations of a ketorolac-eluting ureteral stent by measuring tissue levels of ketorolac and comparing them with orally administered ketorolac in a porcine model.
Materials and Methods
Ketorolac was loaded into Percuflex Plus (Boston Scientific Corporation, Natick, MA) ureteral stents in three different concentrations (7%, 13%, and 15% weight based, Lexington Stent, Boston Scientific Corporation, Natick, MA). The control group consisted of a non–drug-eluting Percuflex Plus ureteral stent that was administered oral ketorolac (10 mg qid) for 5 days. Farm pigs weighing between 27 and 43 kg were separated into five groups (n = 92). All stent sizes were 6F diameter and 22 cm long. Table 1 outlines the treatment groups, sample size, and duration of stenting. All animal work was performed at Charles River Laboratories, Worcester, MA.
Stents were cystoscopically placed transurethrally under general inhalational anesthetic. Benzathine-procaine penicillin G (40,000 U/kg intramuscularly) was administered at the time of surgery. Twelve (N = 12) control animals in group 1 had placement with a control stent bilaterally and administered oral ketorolac 10 mg qid for 5 days after stent insertion to provide tissue comparison levels of orally administered ketorolac. The ketorolac-loaded stents were loaded in doses of 7%, 13%, and 15% of the dry weight of the stent. Before the onset of the study, the 13% loaded ketorolac stent was identified as being the ideal dose without compromising the structural integrity of the stent. Necropsies were performed at scheduled times outlined in Table 1. Percutaneous aspiration of urine and venipuncture were obtained immediately before necropsy.
Ketorolac drug concentrations were determined to characterize the drug uptake in local urinary tract tissues and systemic blood levels from the Lexington stents compared with the control stent and oral ketorolac dose group. Ketorolac levels were measured in plasma, urine, and tissue sampled from ureters, bladder, kidneys, and liver using high performance liquid chromatography (HPLC, Waters Alliance Separations Module, Model 2695, Waters Corporation, Milford, MA). All stents (ketorolac-loaded or Percuflex) were removed to determine the remaining ketorolac concentration. After tissue homogenization, HPLC was used to determine drug concentration in the corresponding tissues using an established protocol validated in our laboratory after the Guidance for Industry, Bioanalytical Method Validation fromthe Food and Drug Administration (
The remainder of the genitourinary organs and liver were fixed and processed for histopathologic analysis and analyzed for any abnormality by a veterinarian pathologist blinded to the treatment group (Charles River Laboratories). Drug-loaded ketorolac stents and control stents were recovered from all animals in all groups and assessed for remaining drug concentration on days 2, 5, 15, 30, and 60 using HPLC. All HPLC was performed at Boston Scientific laboratories (under the supervision of HD and JL only). All other work was performed at Charles River Laboratories by their staff or BHC under the supervision of JDD.
Results
All animals had successful stent placement cystoscopically and survived to their designated time point.
Drug release
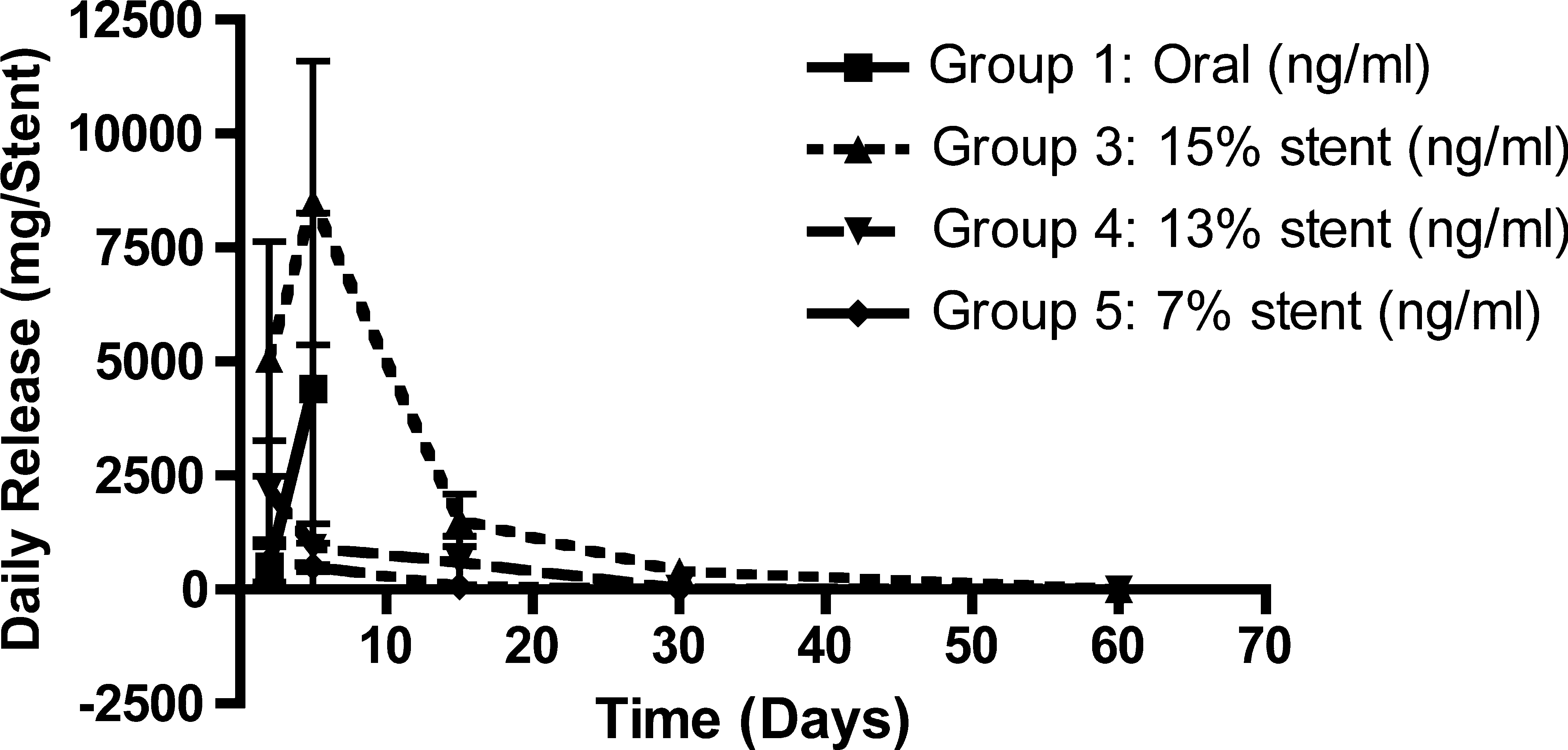
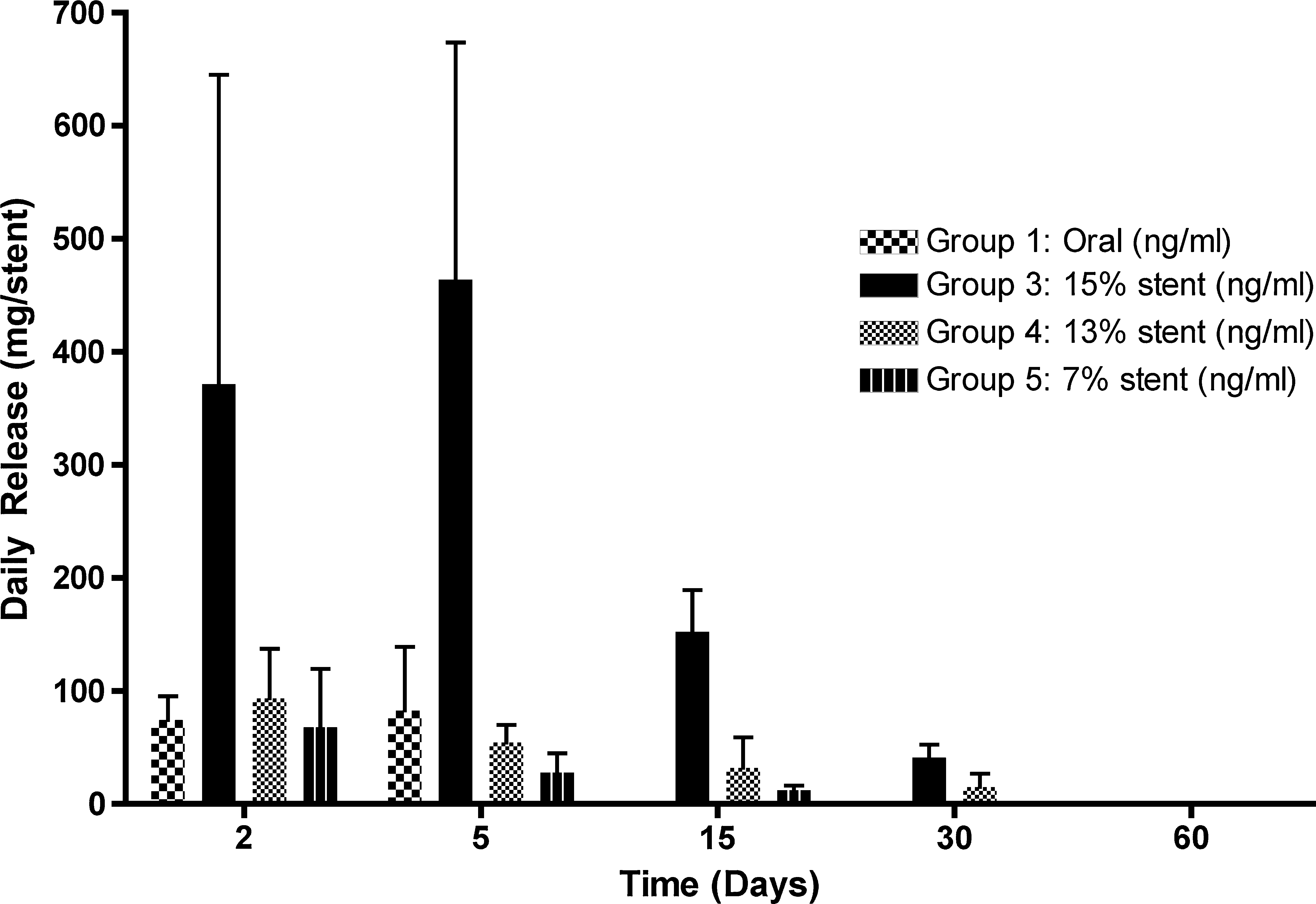
Regardless of the amount of initial drug loaded, the ketorolac-loaded stents (7%, 13%, 15%) share similar release profiles, with a burst in release on day 2 (Fig. 1). The cumulative amount of ketorolac released was related to the initial amount loaded into the stent. After day 15, stents released below 10% of the recommended daily oral dose (4 mg/stent/d) for both the 13% and 15% ketorolac-loaded stents. The total amount of ketorolac released per stent by day 30 was 111 mg and 65 mg for the 15% and 13% ketorolac-loaded stents, respectively (Fig. 2). By day 60, the 15% ketorolac-loaded stent approached complete release of drug (135.4 ± 1.2 mg/stent) while the 13% stent released approximately 80% of the loaded ketorolac (93.4 ± 3.5 mg/stent). The 7% ketorolac loaded stent released 51% of the original loaded amount (32.3 ± 0.9 mg).

Comparison of daily ketorolac release (mg/stent).
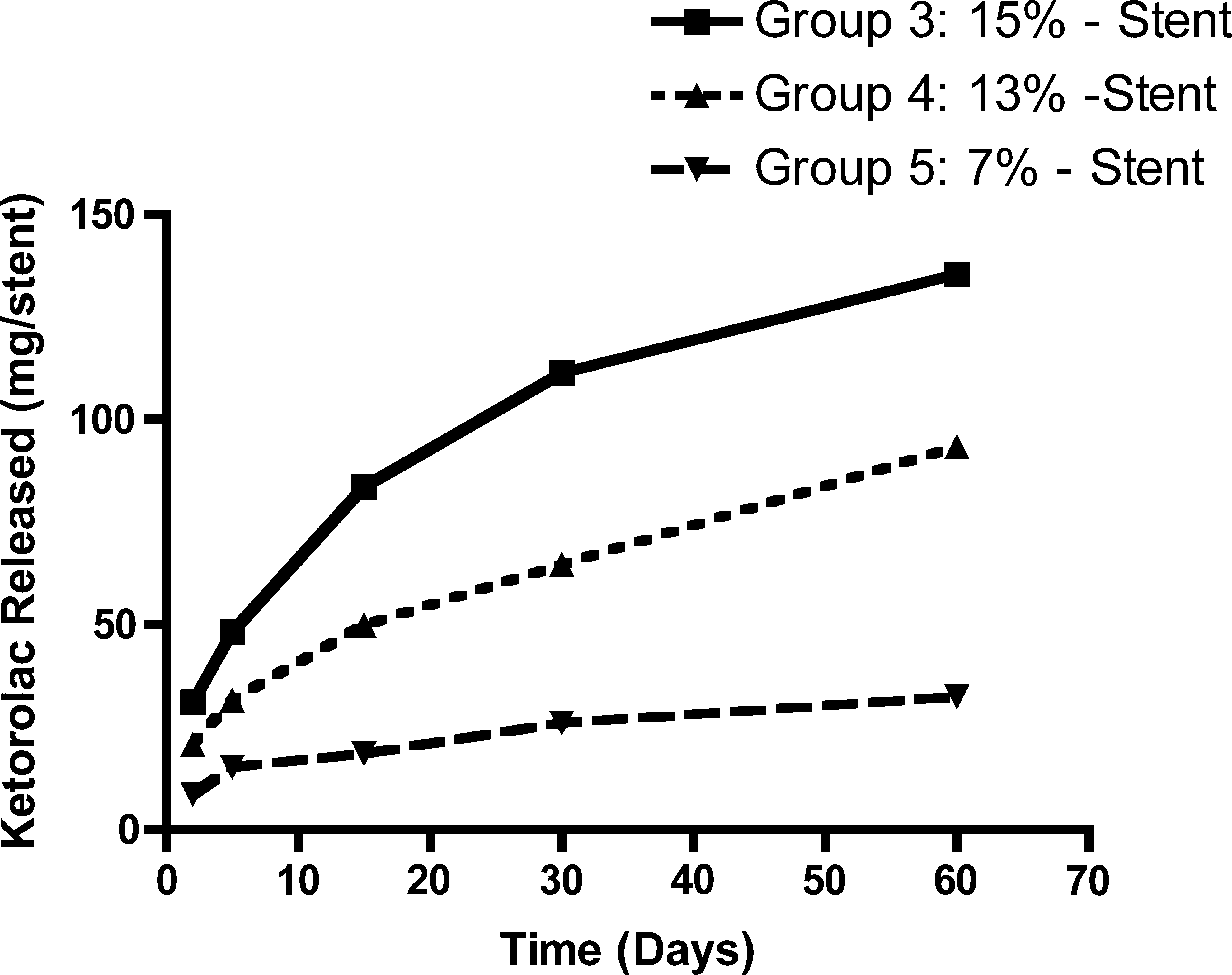
Comparison of cumulative ketorolac release profiles.
Throughout the study duration of 60 days, the maximum concentrations in the blood, liver, and kidney of the 15% loaded group (stented bilaterally) were 10%, 11%, and 12%, respectively, of the tissue levels found in the orally dosed group. By day 60, ketorolac concentrations in the blood, liver, and kidneys of the 15% and 13% groups were undetectable. With respect to the kidney, tissue concentrations of ketorolac were more than six times greater after oral dosing compared with stenting, regardless of the amount of ketorolac in the ureteral stent (Fig. 3). Furthermore, the levels of ketorolac in the nonstented contralateral kidney were similar to the kidney with the eluting stent, thus suggesting that ketorolac found in the nonstented kidney of a ketorolac-eluting stented animal was the result of ketorolac absorption and redistribution by the circulatory system.

Kidney tissue levels of ketorolac.
The highest levels found in plasma also occurred in the orally dosed group and were undetectable at many of the time points in the ketorolac-eluting stent groups (Table 2). The highest plasma and liver levels from the ketorolac-eluting stent occurred in the 15% loaded group but was still only one-tenth of the highest level found in the oral ketorolac group. Similar findings were found in the liver levels of ketorolac (Table 3).
[C]oral ratio is calculated based on day 2 oral and day 15 stent concentrations: 347.82/30.01 ≅ 11.6. For 13% stent group, plasma concentration at day 2 is 12.91/347.82 = 3.7%. For 15%, 30.01/347.88 = 8.6%.
N/D = below the limit of detection; N/A = not applicable.
[C]oral ratio is calculated based on Day 2 oral and Day 15 stent concentrations: 136.88/14.93 ≅ 9.2.
For liver, limit of detection = 10 ng/g & LLOQ = 30 ng/g. Results under LLOQ are extrapolated from standard curve.
LLOQ = lower limit of quantification.
The highest urinary levels were found in the 15% ketorolac stent group, followed by the oral ketorolac group (Fig. 4). The 13% ketorolac-loaded ureteral stent produced lower urinary levels than found after oral administration. Figure 5 illustrates ketorolac levels in the ureteral tissue. The ureters with stents displayed the highest ketorolac levels in a dose-dependent fashion that was greater than the levels found in the oral ketorolac group. Figure 6 outlines the levels of ketorolac found in bladder tissue where the 15% ketorolac-loaded ureteral stent produced the highest levels. The 13% ketorolac-loaded stent produced equivalent levels to those found in the orally dosed group. Table 4 outlines the amount of ketorolac found in tissues compared with the orally dosed control group. The 13% ketorolac-loaded ureteral stent produced 4% and 8% of the tissue levels in plasma and kidney, respectively, compared with orally dosed animals and produced nondetectable levels in the liver.
Urine levels of ketorolac.

Ureteral tissue levels of ketorolac.
Bladder tissue levels of ketorolac.
N/D = below the limit of detection.
Pathology
A blinded pathologist conducted evaluation of the fixed tissues. For both groups with stents, there was no difference in incidence or degree of ureteral tissue response (edema, inflammation, and hemorrhage), no difference in renal or urinary bladder tissue response, and no liver pathology. Gastric ulcers were detected at necropsy only in animals that received doses of oral ketorolac, and gastric ulcers were not seen in any animal with ketorolac-loaded stents. Use of ketorolac-loaded stents was associated with an increase in the incidence of microscopic superficial ureteral mucosal erosion, but no accompanying adverse events, such as ureteral perforation or systemic inflammatory response, were noted. None of the doses of ketorolac-loaded stents produced any tissue changes in the kidneys, ureters, or bladders of animals with stents. Squamous metaplasia in ureters with stents of both groups was noted occasionally at the latter time points and considered to be an adaptive response to local irritation and inflammation, and was not considered to be a preneoplastic lesion. Many findings in response to the stents in this study were the same as those that have been previously reported in published literature in both porcine and canine models. 4,5
Discussion
Endoscopes and mechanisms of intracorporeal lithotripsy have improved to the point that the biggest morbidity after ureteroscopic lithotripsy is often the ureteral stent that is left indwelling postoperatively. Stent symptoms include dysuria, hematuria, urgency, and flank pain. In the most severe forms, patients are unable to perform normal activities of daily living and are unable to return to work until the stent has been removed. The exact cause of stent symptoms is unknown but has been theorized to be secondary to one or several of the following: Irritation of the bladder trigone, interruption of normal ureteral peristalsis, reflux of urine into the kidney from the stent, irritation of the renal pelvis by the retention curl, and inflammation of the urothelium by the mechanical irritation of the stent. 6 Softer biomaterials presumably would improve symptoms, but in a randomized trial of a “softer” ureteral stent vs a more “rigid” stent, there was no difference in symptoms. 7
Orally administered tamsulosin was found to improve stent symptoms in a group of 38 patients with a 7F ureteral stent compared with 37 control patients with stents given placebo. 8 The mechanism of the tamsulosin action is to block the alpha receptors of smooth muscle that is located in the ureteral wall. This developed from the use of tamsulosin in promoting spontaneous stone passage from the ureter by preventing spasmodic contractions of the ureter around the obstructing stone. 9
Drug-eluting stents were first pioneered in the cardiology field when paclitaxel, an antimitotic drug, was designed to elute from a metal coronary stent to prevent tissue hyperplasia within the lumen and stenosis of the stent. 10 To determine which medication would best be suited to elute from a ureteral stent to reduce symptoms, three medications were screened by instilling each intravesically in patients who underwent ureteral stent placement before shockwave lithotripsy. 3 Lidocaine, oxybutynin, ketorolac, or saline (control) was instilled in a total of 40 patients in a randomized trial. Stent symptom questionnaires were completed at certain intervals, and ketorolac was found to significantly decrease flank pain compared with the other groups. Consequently, this led to the development of a ketorolac-eluting ureteral stent in an attempt to improve patient comfort.
Ketorolac is a nonsteroidal anti-inflammatory drug that inhibits prostaglandin synthesis and is commonly used to treat patients with renal colic. It has been shown to decrease renal perfusion pressure and ureteral smooth muscle contractility in animal models of ureteral obstruction. 11,12 Although the exact causes of stent-related symptoms are unknown, inflammation of genitourinary tissues is believed to be involved and preventing this inflammation would be beneficial in reducing pain. Ketorolac-eluting ureteral stents were studied in three different concentrations in this study to determine tissue and plasma levels produced by stents that contained low dose (7%), target dose (13%), and safety-margin dose (15%) of ketorolac compared with animals who were administered ketorolac orally. These amounts were chosen to provide a dose-response curve. The upper limit of 15% was chosen, because this is the maximum amount that can be loaded into a ureteral stent before the properties of the biomaterial change.
The majority of ketorolac from the eluting ureteral stents was released within the first 30 days after implantation in a similar fashion in all dosages of stents (Fig. 1). The stability of the stents was not affected by the loading of drug into the material. All stents were implanted by one surgeon (BHC), who could not discern any difference between stents during implantation. Furthermore, all stents maintained integrity as evidenced at necropsy, and all of the retaining curls remained intact and prevented stent migration.
The benefit of a drug-eluting ureteral stent is concentrated delivery of drug to local tissues where it can be most effective and, at the same time, also reducing systemic levels and the potential for side effects. Ketorolac-loaded ureteral stents delivered greater amounts of ketorolac to the ureteral and bladder tissue compared with the orally dosed group, further validating that a drug-eluting ureteral stent would deliver the highest levels of drug to local tissues in the urinary tract and have the potential for the greatest effects.
The ureteral concentrations of ketorolac were between 2 to 5 times the concentration found in the oral control group from days 2 to 31. The systemic levels were substantially lower or nondetectable compared with the oral control group. Plasma levels of ketorolac were highest in the oral control group compared with all ketorolac stent groups at days 2 and 5. This study shows that a drug-eluting ureteral stent can deliver high levels of drug to the immediately surrounding genitourinary tissues, such as ureters, bladder, and urine. If stent symptoms have a pathogenesis similar to that of renal colic, then ureteral spasm may play a role, and reducing ureteral contractility would result in improved comfort.
The maximum concentrations of ketorolac in the blood, liver, and kidney of the 13% ketorolac-loaded stent were much lower compared with the oral control group (4%, undetectable, and 8%, respectively). By day 60, ketorolac concentrations in the blood, kidney, and liver of ketorolac-eluting stent groups were undetectable. The maximum recommended daily dose of oral ketorolac is 60 mg. The ketorolac-eluting ureteral stent delivered systemic levels that would be equivalent to 1 mg daily of oral drug and therefore does not represent any safety concerns.
Histologically, the ketorolac-eluting ureteral stent was biocompatible and produced only mild edema and inflammation equivalent to the non–drug-eluting control stents. The ketorolac-eluting ureteral stents did produce slightly more superficial ureteral mucosal erosion, but did not result in ureteral thinning or perforation. This is likely because of the relatively rougher surface of the ketorolac stent compared with the Percuflex Plus, because the drug is blended with the base polymer in both solid and small particle forms. Importantly, such systemic side effects as gastric erosions and ulcerations were not observed in any of the drug-eluting ureteral stent animals as they were in the orally dosed group. This is a prime example of the benefit of locally delivered drug and how it can avoid systemic side effects.
Conclusions
This study has shown that a novel ketorolac-eluting ureteral stent is safe in the porcine model and delivers high concentrations to local ureteral and bladder tissues with minimal levels in plasma. There was a slightly higher incidence of superficial ureteral mucosal erosion in the drug-eluting stent group, but this was not associated with any negative effects. What remains to be seen is whether this will result in a clinical benefit, which can only be addressed in a randomized, blinded, controlled clinical trial.
Footnotes
Disclosure Statement
Jamie Li and Hamid Davoudi are Boston Scientific Corporation employees. Ben H. Chew and John D. Denstedt are consultants with Boston Scientific Corporation.