
Abstract
The laparoscopic management of difficult adhesions can be quite challenging for even the most experienced of laparoscopic surgeons. We describe a case of managing a suspected enterotomy with a laparotomy during a robot-assisted radical prostatectomy and the surgical options after repair. The case was complicated by a Meckel's diverticulum fused and continuous with a urachal cyst, itself a rare occurrence. After the excision of the Meckel's diverticulum–urachal complex, the laparotomy incision was closed, and the prostatectomy was performed robotically. We discuss the controversies regarding continuation of a planned robotic procedure after a midline laparotomy.
Introduction
We believed it necessary to make a laparotomy incision to deal with a suspected enterotomy before beginning a robot-assisted radical prostatectomy (RARP). After the general surgical portion of the procedure, three options existed. First, the laparotomy incision could be closed, the surgery terminated, and the RARP rescheduled for a future date. Second, the operation could be converted to an open radical retropubic prostatectomy. Finally, the laparotomy could be closed, the abdomen re-insufflated, and the prostatectomy performed robotically. We decided to perform the last option. We will discuss our reasoning behind this decision as well as the embryology of Meckel's diverticula (MD) and urachal remnants.
Case Report
A 59-year-old man with a history of a remote appendectomy and no medical history was taken to the operating room for a planned RARP after the diagnosis of clinically localized prostate cancer. During initial laparoscopy after trocar placement (but before docking the robot), a broad adhesion to the midline abdominal wall was noted from the periumbilical region and continuing inferiorly. It appeared that bowel was in this adhesion, and a laparoscopic adhesiolysis was begun. The adhesions were extremely dense and seemed to be continuous with the abdominal wall. During adhesiolysis around a cystic structure, there was concern for an enterotomy as it appeared that bowel mucosa was exposed.
A general surgeon (B.P.J.) was consulted, who felt that the laparoscopic exposure was inadequate. The decision was made to evaluate the adhesions and cystic structure from an open approach. The trocars were removed, and the abdominal cavity was opened with a 15-cm periumbilical midline laparotomy incision. Lysis of adhesions continued, and it was discovered that a MD was densely adherent to the infraumbilical midline region. The MD measured ∼12 cm in length and was located ∼50 cm from the ileocecal valve. The distal portion of the MD was found to be fused to and continuous with what appeared to be a urachal remnant (Fig. 1). The urachus was freed from the anterior abdominal wall and traced to the dome of the bladder, where it was transected. The MD was transected transversely at its origin at the ileum. The entire small bowel was run, and no additional pathology or enterotomies were discovered.

Meckel's diverticulum with fused urachal remnant.
At this point in the operation we decided that it was safe to proceed with the prostatectomy. Rather than extend the patient's laparotomy incision to the pubic symphysis and continue with an open radical retropubic prostatectomy, we believed that an RARP could be performed safely. The trocars were replaced through their incisions under direct vision, and the laparotomy incision was closed with interrupted #1 polyethylene terephthalate sutures in a figure-of-eight fashion. The supraumbilical trocar was replaced and the abdomen was re-insufflated. The RARP proceeded with no further complications. At the conclusion of the procedure, the fascia remained intact, but two sutures had loosened. Concern for fascial integrity led us to remove all interrupted sutures, deliver the specimen, and close the fascia with a running O-looped polydioxanone suture.
The patient's postoperative recovery was complicated by a wound infection, which was subsequently opened. He was discharged on postoperative day 4 after improvement in the infection and the recovery of bowel function. One month postoperatively, the patient's wound infection had resolved, he did not develop any additional complications, did not require readmission, and had an undetectable prostate-specific antigen.
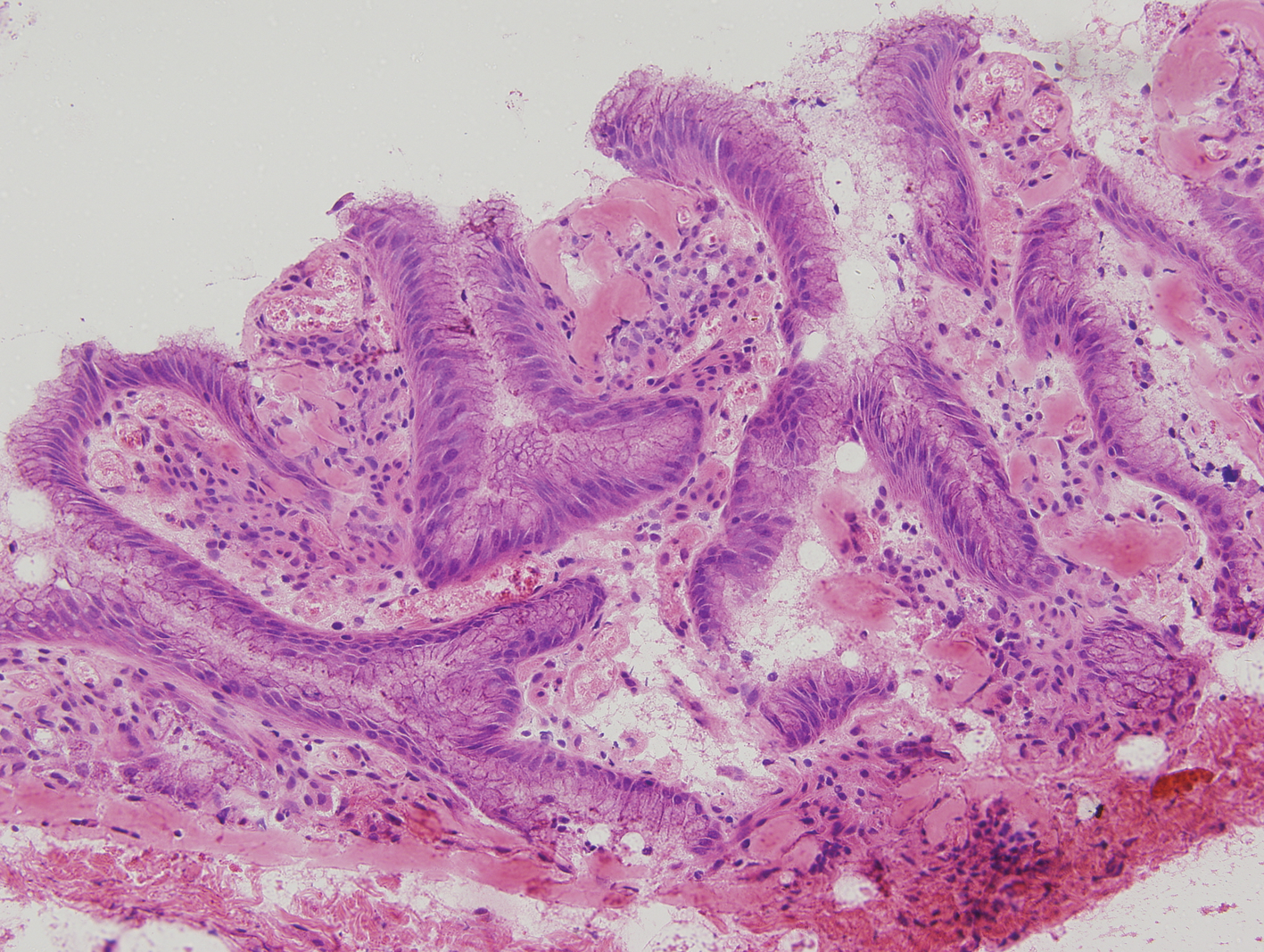
Final histopathology revealed a portion of small intestine with adjacent gastric type mucosa, consistent with an MD (Fig. 2). Additionally, the urachal cyst specimen was consistent with urachus, including muscularis propria (Fig. 3).

Meckel's diverticulum with ectopic gastric mucosa (40 ×).
Urachal cyst with columnar epithelium (200 ×).
Discussion
Two aspects of this case warrant reporting and further discussion. The rare finding of two fused yolk sac remnants is interesting and explains the presence of dense periumbilical adhesions. More importantly, however, is a discussion regarding the management of difficult adhesions, laparoscopic enterotomy, and the ability to convert back to a laparoscopic or robotic procedure.
In this case, given the abnormal anatomy and questionable enterotomy early in the case, we did not feel comfortable proceeding further laparoscopically. Converting to an open laparotomy improved the exposure to safely finish adhesiolysis and repair the enterotomy; it also permitted us to run the bowel. As we discovered, converting to an open procedure did not compromise the ability to continue with the planned RARP. This decision was validated over time, as the patient did well postoperatively, with the notable exception of a wound infection.
Given the outcome, one cannot be overly critical of the procedural plan, but a natural question arises: In retrospect, would we have been able to perform this procedure completely laparoscopically or robotically? Currently, we are not experienced enough with intracorporeal bowel surgery (we perform our urinary diversions extracorporeally during robotic cystectomy) to comfortably repair an enterotomy, excise an MD, or confidently run the bowel laparoscopically. The location of the MD–urachal cyst complex on the midline anterior abdominal wall would have been difficult to approach robotically. In a patient positioned for robotic prostatectomy, the robot must approach from between the patient's legs. Given the triangulation requirements of the robot, this essentially mandates that the camera port must be in the midline. Thus, the midline structure would be viewed from a midline approach, making it difficult to observe both sides of the adhesion. This is obviously suboptimal and likely unsafe.
After repair of the enterotomy, closing the laparotomy and abandoning the RARP would have been a reasonable management option. However, this would have required another hospitalization, procedure, and additional operative risks. We believed that there were no contraindications for performing the RARP once the MD had been addressed and the bowel run to our satisfaction. One area of concern was whether the fascial closure would be sufficiently air-tight to accommodate pneumoperitoneum. We found that this was not an issue with an interrupted fascial closure. A running fascial closure would likely have also been sufficiently air-tight.
In many laparoscopic operations, the intended procedure can be performed through a laparotomy incision, minimizing the morbidity of open conversion. In this case, however, the relatively small periumbilical incision would have needed to be extended inferiorly to the pubic symphysis, resulting in a very large incision. With such a large incision and an open peritoneum, the exposure of the prostate would have been suboptimal and the bowel would have needed to be retracted. Effectively this would have been the same incision as an open radical cystectomy (if not larger), and similar lengthy convalescence would thus be expected. In addition, we personally believe that we can perform a better prostatectomy from a robotic approach than an open one. As such, the best option for our patient was an RARP.
This brings us to our decision: closing the laparotomy and continuing with the prostatectomy robotically. The concept of reinsufflation after laparotomy closure is not novel. In fact, it is commonly performed during robotic cystectomy to perform the urethral-neovesical anastomosis of an extracorporeally created neobladder. However, the translation of this practice into the setting of possible enterotomy before robotic prostatectomy has not, to the best of our knowledge, been reported in the urologic literature. (A single case report of an open repair of a small bowel injury before a laparoscopic ventral hernia has been reported in the general surgery literature. 3 ) We offer a surgical management option for a suspected enterotomy during an RARP that permits a thorough examination of the bowel, without compromising the ability to continue with the prostatectomy robotically.
Embryologic Review
The urachus and the omphalomesenteric duct both develop from the yolk sac early in embryological life. An MD is a true diverticulum that forms secondary to the failure of the vitelline duct to obliterate during the fifth week of fetal development. It is the most common congenital abnormality of the gastrointestinal tract, occurring in 2% of the population. In some circumstances, the MD contains ectopic mucosa, most commonly gastric. These MDs are more likely to be symptomatic with a variety of presenting complaints ranging from abdominal pain to gastrointestinal bleeding and acute bowel obstruction. 4 In the majority of cases, however, the MD is asymptomatic and is often diagnosed during an elective surgery.
Formed from endodermal tissue, the urachus is the embryological remnant of the allantois. By the fifth month of gestation, the urachus usually narrows down to a narrow epithelial tube that connects from the apex of the bladder to the umbilicus. The fibromuscular band usually becomes obliterated shortly after birth to form the median umbilical ligament and is flanked by the remnants of the umbilical arteries, the medial umbilical ligaments. It is believed that the urachus persists in half of fetal specimens but only 2% of adults 5 ; a urachal cyst is thought to occur in 1 in 5000 births. 6 The urachus can remain completely open or obliterate partially, leading to the formation of cystic structures at any site along the tract. Similar to an MD, these cysts are often asymptomatic, but can present after they become infected or as an incidental discovery during an abdominal operation.
The presence of both urachus and omphalomesenteric duct remnants in the same patient is a rare pathology. In 1977, Pinté et al 7 reported that out of 66 cases with an MD, 1 patient had an associated urachal duct remnant. In 1983, Rich et al 8 described that out of 35 patients with anomalies of the urachus, 2 had omphalomesenteric duct remnants.
Conclusion
Our experience suggests that should the need arise to enter the abdominal cavity during a laparoscopic operation, it is possible to close a large laparotomy incision and still complete the desired laparoscopic procedure. The potential operative advantage of completing the procedure robotically over an open technique suggests that closing the laparotomy and proceeding robotically may benefit the patient. As we continue to push the boundaries of laparoscopy, occasionally a step backward in the name of safety is the better part of valor.
Footnotes
Disclosure Statement
No competing financial interests exist.