
Abstract
Introduction:
The prone position has been considered the only position for percutaneous access to the kidney for the past 25 years, whereas the supine Valdivia position has recently started to gain acceptance, although it was originally described in the late 1980s. Even more recently, the Galdakao-modified supine Valdivia position was described. However, there is no consensus on which is the best position for percutaneous nephrolithotomy, and the choice is currently based on the surgeon's preference.
Materials and Methods:
The prone, supine, and modified supine positions are described, pointing out the advantages, disadvantages, and results of each technique.
Results:
A number of potential advantages have been described for the supine over the prone position: less cardiovascular change; no need for patient repositioning (with less associated risk of central and peripheral nervous system injury); less X-ray exposure to the surgeon; and less risk of colonic injury. The recently described Galdakao-modified supine Valdivia position allows for a simultaneous anterograde and retrograde approach to the renal cavities for the one-stage treatment of complex renal stones or concurrent renal and ureteral calculi. Moreover, the use of a flexible ureteroscope allows for Endovision puncture to achieve perfect access to the kidney.
Conclusions:
The prone position still represents the standard for percutaneous access to the kidney, and other positions should be compared with this position. However, the supine and the modified supine positions have potentially important advantages for both patients and surgeons that need to be investigated in a large randomised trial to define their superiority over the traditional prone position.
Introduction
In 1987, Josè Gabriel Valdivia-Uria introduced the supine approach for percutaneous nephrolithotomy (PCNL), describing the advantages of his technique that he defined as “a simplified technique.” 3 For the next 15 years, most urologists were reluctant to change from the traditional prone position to the supine one. Recently, however, interest in the supine approach has risen significantly, primarily in high-risk and morbidly obese patients. 4,5 Moreover, the development of better technology and vision with flexible scopes for the upper urinary tract contributed to the development and adoption of a combined technique, both in prone and supine positions. This technique allows surgeons to perform a simultaneous anterograde and retrograde endourological approach to the upper urinary tract for the treatment of some complex stone cases. 6 –10
Medical literature is confirming a renewed interest in percutaneous access to the kidney with a numbers of reports during the past 5 years. 11 –14
In this article, we set out to determine whether there is any evidence supporting a best position for approaching the kidney percutaneously.
Materials, Methods, and Results
Prone position
Since 1976, when Fernstrom and Johansson first reported their technique for removing kidney stones through a percutaneous nephrostomy under radiological control, PCNL has become the standard treatment for endoscopic removal of large renal calculi and is usually performed in the prone position, traditionally considered the safest position for percutaneous access to the kidney. 15
The prone position allows posterior access to the collecting system through the Brodel's avascular plane without significant kidney bleeding and peritoneal or visceral injuries. A wide surgical field for the selection of the puncture site (in particular, for the upper pole calyceal puncture), an adequate nephroscopic manipulation, and a good distention of the collecting system are the other advantages of the prone position for PCNL. This technique is associated with a success rate of 84% to 91%, with minimal complications such as acute bleeding (requiring blood transfusion in 3% to 10% of cases) and bowel perforation in 0.5% of the cases. 16
The first step of PCNL is to create correct access to the renal collecting system, which can be achieved by fluoroscopic or ultrasound-guided puncture or by a mixed procedure. Ultrasound is useful to determine the direction of the needle along the most appropriate angle toward the target entry point, identifying the third dimension. Additionally, ultrasound allows the evaluation of the possible interposition of the splanchnic organs between the skin and the kidney.
Patients are initially placed in a supine position to allow the insertion of a ureteral catheter before performing the kidney puncture, to obtain a retrograde pyelography, or to fill the kidney with saline. The need for an additional intraoperative change of the decubitus to obtain the prone position is potentially dangerous for the patient and prolongs the operative time. Thus far, some authors have proposed alternative modified prone positions as an oblique prone or a prone split-leg position (Fig. 1) to allow for concomitant access to the upper urinary tract 10 and endoscopically guided percutaneous renal access 8,9 or to manage potential migration of stone fragments into the ureter during the PCNL. 17 Moreover, the use of flexible instruments has also allowed easier access to the bladder in the standard flat prone position, except in those patients who are morbidly obese or with known urethral strictures. 18
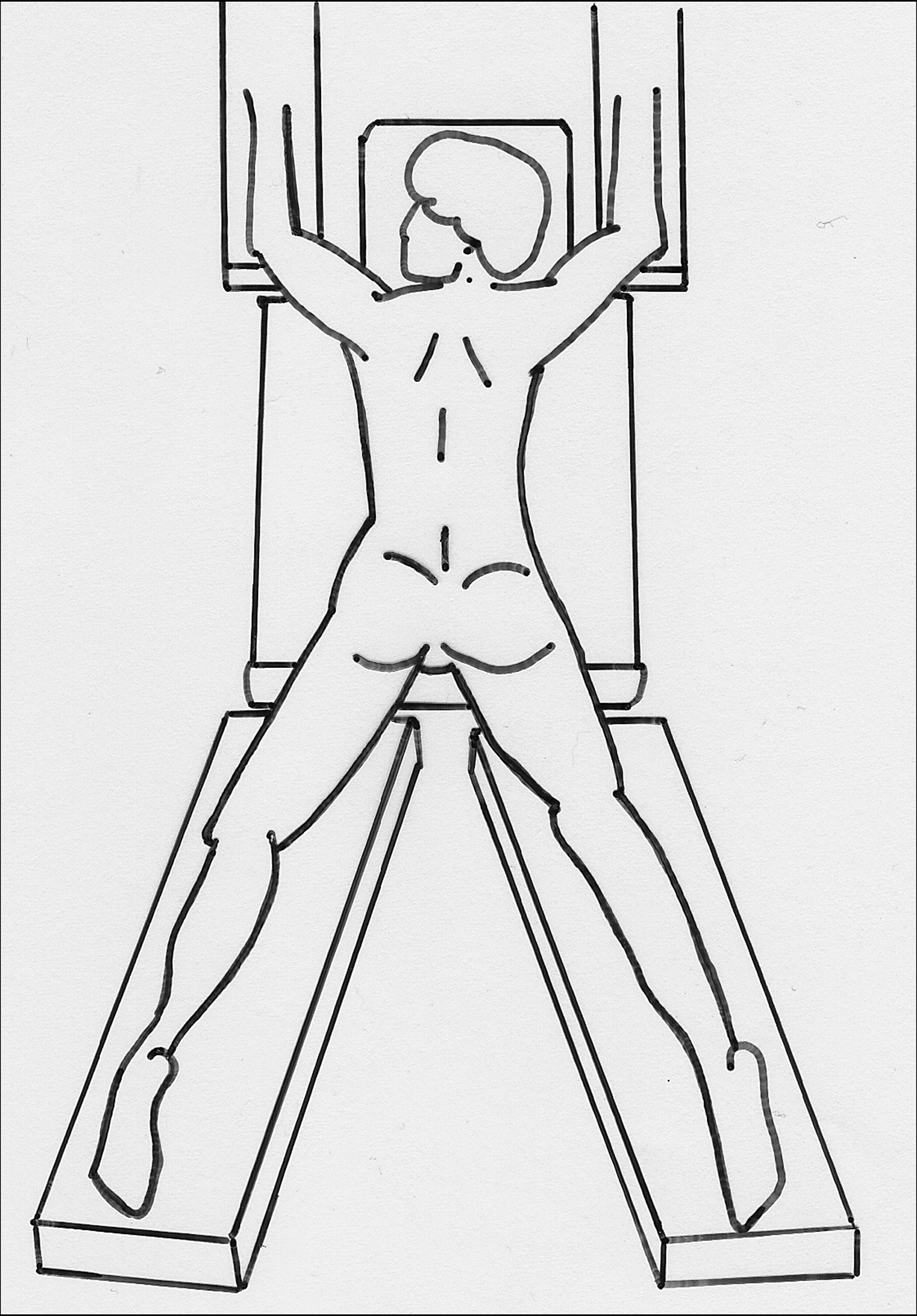
The prone split-leg position.
The correct position of the patient during a PCNL has always been a debated issue, as the precise access to the kidney is facilitated by a careful positioning of the patient and can reduce intraoperative complications. In the flat prone position, the deflection of the patient placed on a special cushion may increase the distance between the 12th rib and the iliac crest, thus enlarging the area for the correct puncture of the kidney as a consequence. However, elevating the patient from the fluoroscopic table can interfere with a correct handling of the nephroscopes and probes. 17
The major limitations of the prone position are the potentially significant cardiovascular changes, in particular if the patient is affected by severe obesity or associated pulmonary disorders. When moving a patient into the prone position, an almost universal finding is a decrease in the cardiac index that has been variously attributed to reduced venous return, direct effects on arterial filling, and reduced left ventricular compliance secondary to increased thoracic pressure. 19 Obstruction of the inferior vena cava is a well-recognized complication of prone positioning that leads to decreased cardiac output, venous stasis, and potential thrombotic complication. 19 An increased sympathetic activity (increased heart rate, total peripheral vascular resistance, and plasma noradrenaline) has also been described. 20 Turning a patient from the supine to the prone position should be performed carefully, avoiding excessive neck movement and allowing normal blood flow in the carotid and vertebral arteries. Failure to observe these precautions can lead to serious complications of the central nervous system. 19 Moreover, cervical spine injury can be the consequence of excessive neck flexion or extension during surgery in the prone position. 21 Therefore, the head is usually supported on a pillow to obtain a neutral neck alignment. Another important issue is the necessity of a continuous control of the endotracheal tube to ensure that no kinking of the tube occurs. Finally, if the procedure is carried out under spinal or epidural anesthesia, conversion to general anesthesia with endotracheal intubation, if required, will present a great challenge to the anesthesiologist. Musculoskeletal complications (e.g., a stiff neck, hoarseness caused by vocal cord compression, brachial plexopathies, and myelic lesions) have been reported after prone PCNL, particularly in patients with severe cervical spondylosis. 22,23 Additional instruments, such as helmets or mattresses, have been proposed to reduce the potential anesthetic and skeletal complications for patients during a prone PCNL. The Montreal mattress is a rectangular mattress with a central hollow that helps prevent compression of the abdomen during respiration and therefore improves ventilation and cardiac output during surgery; it can be fixed to the operating table to avoid movement. 22 The Proneview protective helmet system has also been used during prone PCNL to support the head, keep the neck neutrally aligned, and still allow a concomitant direct vision of the patients' face and of the endotracheal tube. 23 The simultaneous use of these two tools can reduce the potential complications related to the patient's positioning during a prone PCNL, in particular in patients otherwise considered unsuitable. 23
Supine position
It is difficult to change a standardised technique when good results and a low complication rate have been achieved. In chapter 6 of The Tragedy of Pudd'nhead Wilson, Mark Twain wrote, “Habit is habit, and not to be flung out of the window by any man, but coaxed downstairs a step at a time.” This may explain why most urologists prefer not to consider switching from the traditional prone to the supine position when approaching the kidney during PCNL despite the fact that initial evidence of the efficacy of such techniques were already published in the late 1980s by Gabriel Josè Valdivia-Urìa. 3 Ten years later, in 1998, the same author described the first series of PCNLs in the supine position, once again without obtaining a unanimous consensus among the endourological community. 24 What has happened over the last 10 years? A number of publications and editorial comments from several centers all over the world have appeared in the literature, which support the conclusions that Valdivia-Uria pointed out two decades before. 5,11,13,14,16,25,26 At the same time, the supine technique has been repeatedly shown during live surgery sessions and has been widely debated at main urological meetings worldwide. Thus, the supine approach has started to become more accepted and is being practiced. 27
The supine position for approaching the kidney percutaneously, as described by Valdivia-Uria, 3,24 consists of placing the patient supine, with the side harboring the stone close to the lateral extremity of the operation table. The posterior axillary line is marked with the patient in a standing position before the operation, whereas the XIIth rib margin and the iliac crest are marked just after the ipsilateral flank is elevated with a 1 to 3 liter water bag (depending on the patient's body size) to outline the area for the percutaneous access to the kidney (Fig. 2). The ipsilateral arm is laid on the thorax while fluid replacement is assured on the contralateral arm. Pressure injuries (such as ligament lesions and neurological deficits including brachial plexus palsy) should be prevented by adequately applying soft pads under all the pressure points at risk. Before draping the patient, it is important to verify that the radio-opaque bar of the operating table does not lie in correspondence with the operating field, thereby hampering fluoroscopy.
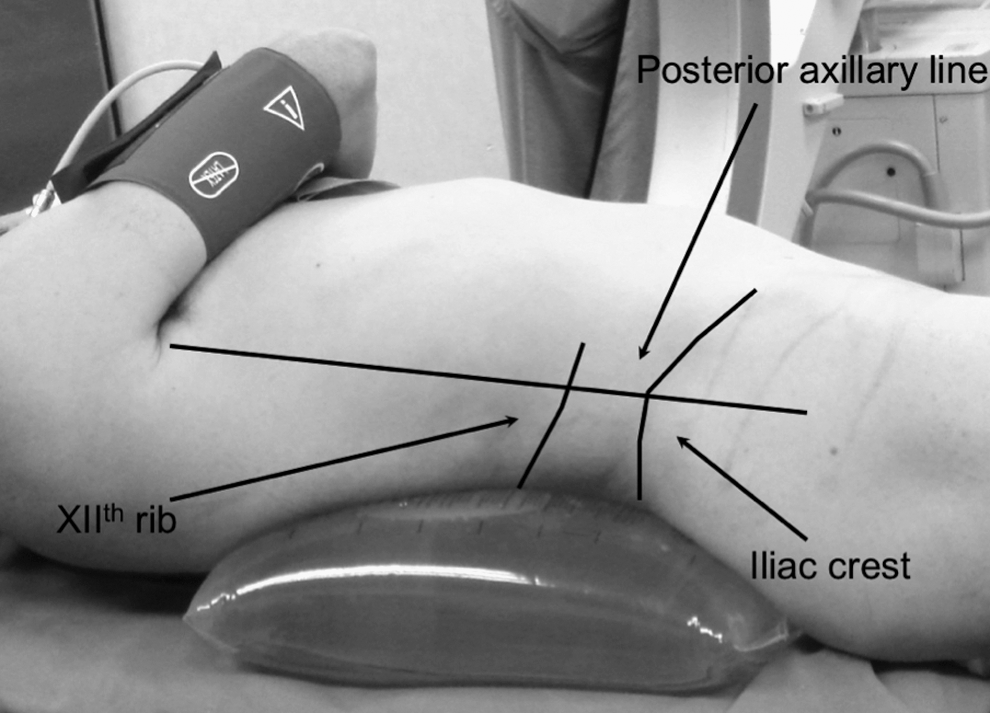
Skin markers (posterior axillary line, iliac crest, and the XIIth rib margin) to outline the area for the percutaneous renal access.
Flexible cystoscopy, through an easily accessible urethral orifice, is used to place a retrograde ureteral catheter to obtain a pyelography, just before puncturing the chosen calix. Similar to the prone position, the puncture can be performed under fluoroscopic, ultrasound, or a mixture of guidance procedures. Correct access to the tip of the renal papilla is gained under biplanar fluoroscopic guidance. The needle follows a plane which is perpendicular to that of fluoroscopy, allowing easy control of its entrance into the collecting system and eliminating the need to rotate the radiologic C-arm, as is usually performed during the prone approach.
Differing from the prone position, the surgeon is seated while puncturing the kidney, with the needle almost horizontal or slightly inclined upward toward the operating table. This orientation of the needle, and consequently of the Amplatz sheath, explains why the supine position favors the drainage of the stone fragments during PCNL and allows the surgeon to carry out a low-pressure procedure. This is different from the prone position, wherein the needle is almost vertical (Fig. 3). The renal puncture should be made behind the posterior axillary line, without overpassing it ventrally, to avoid splanchnic injury.

Direction of the needle during supine (
A number of potential advantages for the supine Valdivia position could be outlined:
First, it is more comfortable for the surgeon, who may work while sitting down during prolonged procedures.
The X-ray exposure to the surgeon during the entire procedure is decreased, because he no longer works with his hands in the fluoroscopic field.
It implies important anesthesiological advantages, including a low incidence of cardiovascular, respiratory, neuroendocrine, and pharmacokinetic problems, which are more frequent with the prone position, particularly in patients with compromised cardiopulmonary function, kyphosis, debilitation, and morbid obesity. Moreover, it allows for more rapid access to the airways during the entire procedure, making it potentially less hazardous for any patient.
Further, patient positioning is less demanding and time-consuming, because an intraoperative change of the position is not required. This means less risk of central and peripheral nervous system injuries related to an inaccurate repositioning and a single definitive draping of the patient.
Colonic injuries are also potentially less frequent due to the more anterior displacement of the colon with the patient in the supine position, as described by Hopper et al. 28
Moreover, since the percutaneous tract is horizontal or slightly inclined downward, spontaneous evacuation of stone fragments during the procedure is easier.
As with all things, there are disadvantages as well. The superior calyceal puncture is more challenging, because the upper pole of the kidney is more medial and posterior and is deeply located within the rib cage. A decreased filling of the collecting system may result in more difficult nephroscopy, because the renal cavities are constantly collapsed. However, it should be observed that maintaining low pressures within the renal cavities may be important to prevent fluid absorption and urosepsis. Finally, an anteromedial movement of the kidney during dilation was noticed with the supine position, sometimes making the procedure more difficult.
The learning curve has been discussed, but no study has yet been conducted on this topic to evaluate the difference between the prone and supine positions.
Comparison of outcomes of supine and prone PCNL
The overall outcomes of PCNL performed in the supine position (Table 1) are similar to those with the prone approach (Table 2), in terms of stone-free rate, secondary procedures, major complications, and transfusion rate. 16 In a randomised study recently conducted by De Sio et al, 13 no significant differences in the stone-free rate (supine 88.7% vs. prone 91.6%), mean postoperative Haemoglobin decrease (supine −2.3 g/dL vs. prone −2.2 g/dL), or splanchnic injury (no lesion occurred) were reported. However, the small number of patients enrolled (39 patients, supine position; 36 patients, prone position) and the carefully selected population (body mass index >30 kg/m2, stones in more than one calyx and staghorn stones were exclusion criteria) do not allow any definitive conclusions. Moreover, on comparing the two largest contemporary series of percutaneous approach with the kidney, performed with the patient prone 29 or supine, 24 visceral injury and transfusion rate were reported in 0% and 0.06% and in 1.4% and 0.8% of the cases, respectively. In a recent review conducted by de la Rosette et al, 16 the authors concluded that the outcomes in nonobese patients with small-sized stones seem to favor the supine approach, whereas the prone position provides better stone-free rates in the group of patients with complex renal calculi. However, no definitive conclusions can be drawn due to the well-known limitations of the studies published.
Combined approaches: the modified supine position
The modified supine position, as described by Ibarluzea et al, 6 is a supine decubitus with a lithotomic arrangement of the legs. The posterior axillary line should be drawn on the skin with the patient standing. The patient is then anesthetised and arranged in the Valdivia supine position, with the flank to be operated raised and slightly rotated by a single underlying 3-liter water bag (Fig. 4A) or by two separate jelly pillows placed under the thorax and the ankle (Fig. 4B). The ipsilateral arm is bent on the thorax. Care should be taken to obtain a wide operating space and to avoid any steric hindrance while performing the kidney puncture, with the flank leaning out of the border of the operating table and out of the water bag.
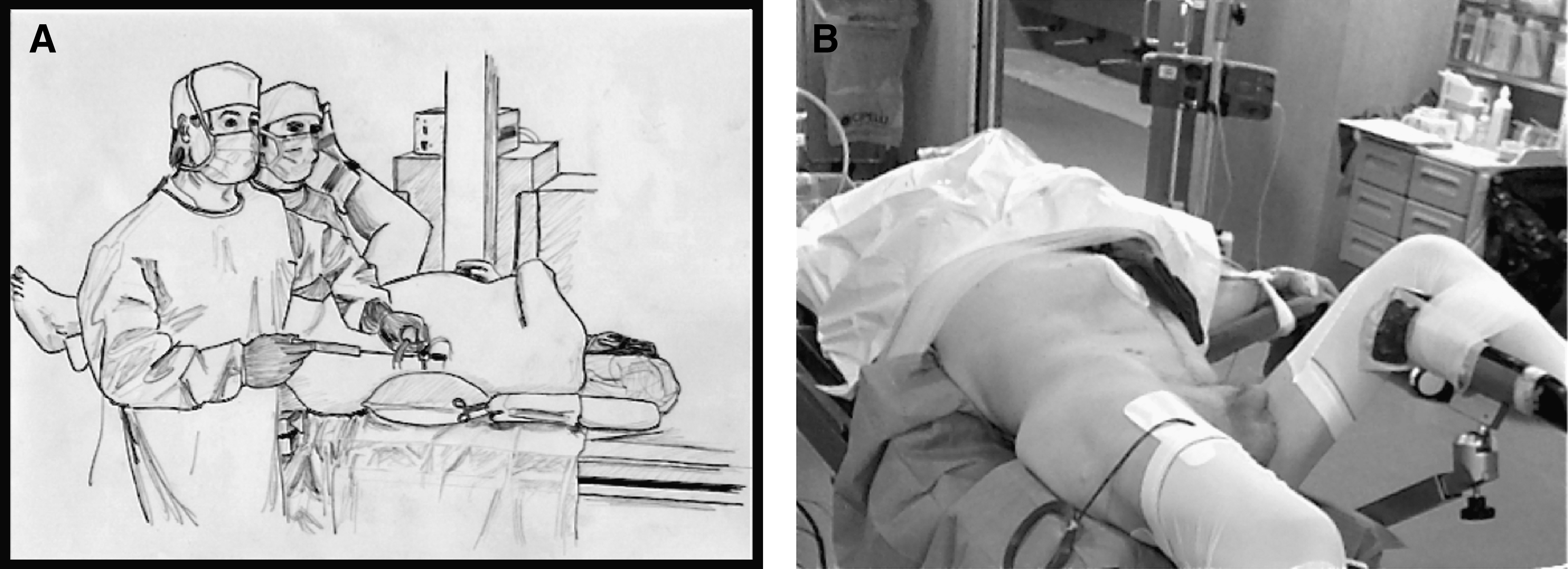
A single 3-liter bag (
Subsequently, the lower limbs are arranged according to the Galdakao-modified lithotomic position, with the leg of the operated side extended and the contralateral one well abducted (Fig. 5A, B). As in the other positions, pressure injuries should be prevented.

The Galdakao-modified supine Valdivia position: front (
Once the positioning of the patient is completed, the area for the percutaneous access to the kidney is delimited, and the renal puncture is made behind the posterior axillary line, as in the supine Valdivia position.
It is necessary to follow a precise protocol, determining exactly the spatial organisation of the operating room, which is very crowded by the operators and by numerous, cumbersome instruments. First, the two urologists (one for the percutaneous procedure, the other for the retrograde rigid or flexible ureteroscopy) should be able to look at all the monitors during the entire procedure (ultrasound, fluoroscopy, and endoscopic monitors) without continuously moving from their working positions. The instrumenting nurse should be able to reach and help both urologists, and the anesthesiologist and nurses should not be hindered in their activities by the working material (lithotripsy energy source and other accessories), without interfering with the procedure themselves.
Figure 6A and B show two different schemes according to the side being operated on.

Spatial organization of the operating room in the Galdakao-modified supine Valdivia position according to the kidney to be approached: right (
The Galdakao-modified supine Valdivia position has some potential advantages, including those already mentioned for the supine position.
As in the other positions, the renal puncture may be performed under ultrasound and/or fluoroscopic guidance. An alternative possibility is to perform a percutaneous renal puncture under direct visual guidance (Endovision puncture) by using flexible ureteroscopy that allows the needle to reach exactly the tip of the chosen renal papilla along the Brodel's avascular line and thus prevents hemorrhagic complications. Direct retrograde vision of the collecting system may also be useful during the dilation of the percutaneous tract and the application of the Amplatz sheath, avoiding an excessive use of fluoroscopy. Finally, during this step, it may be useful to apply a security guide wire through the percutaneous tract, traveling down the ureter and coming out from the urethra, obtaining a so-called “kebab-patient.”
This position allows a preliminary retrograde ureteroscopic evaluation, which is not strictly necessary but is sometimes useful (i.e., for evaluation and/or treatment of concomitant ureteral calculi or strictures, evaluation of the possibility of a simple retrograde treatment, Endovision percutaneous renal puncture, and subsequent retrograde retrieval of calculi from calyces not otherwise reachable through the percutaneous tract).
It allows a great versatility in the treatment of the urolithiasis along the entire urinary tract, allowing the use of combined percutaneous anterograde and ureteroscopic retrograde maneuvres (endoscopic combined intrarenal surgery, Fig. 7), using both rigid and flexible endoscopes, and minimising the need for multiple percutaneous accesses with related risks. In particular, using the anterograde and retrograde routes, simultaneously with both rigid and flexible instruments, makes the superior calyceal puncture an unnecessary approach, eliminating potential and important complications linked to a supracostal access.

Endoscopic combined intrarenal surgery using both rigid (
Additionally, the combined use of retrograde and anterograde instruments might increase renal cavity dilation when needed, allowing a pressure-controlled procedure.
Only one clinical study on this technique has been published 7 ; it reports a single surgeon's experience with 127 consecutive patients. About 40% of the patients were obese (body mass index >30), and 29.1% were classified as American Society of Anaesthesiologists score 3. No organ injuries or anesthesiological complications occurred. The reported transfusion rate was 3.1% with three artero-venous fistulas in the puncture site requiring urgent embolisation. The stone-free rate was 81.9% after the first treatment and 87.4% after the second percutaneous treatment through the same access during the same hospital stay.
Discussion
PCNL has undergone a significant evolution during the last 30 years due to improvements in the access technique, instrumentation, and lithotripsy technology.
For many years, the prone position was considered the only position for PCNL. It provides safe access to the kidney with a very low risk of splanchnic injury, a wide surgical field, adequate instrument manipulation, and a good distention of the collecting system. Nevertheless, some potential anesthesiological complications (directly correlated with the position, including circulatory and ventilatory difficulties) and the intraoperative change of the position represent the most important disadvantages of the prone position. Some modifications of the standard flat prone positions, such as the reverse lithotomy and the prone split-leg position, together with the development of flexible scopes to access the urinary tract allowed a simultaneous anterograde and retrograde approach to the upper urinary tract, avoiding the need to turn the patient during the procedure. 8 –10
The increasingly widespread use of the supine position and, even more recently, of the Galdakao-modified supine Valdivia position have opened a debate on which is the best position for approaching the kidney for PCNL.
The history behind the dissemination of the supine position is somewhat interesting, revealing the surgeon's reluctance to shift from an efficient and low morbidity technique to a new and potentially less morbid procedure. Josè Gabriel Valdivia-Uria first described the supine position in the late 1990s. 3 Fifteen years later, other urologists reported their new experience with this technique, supporting the same conclusions pointed out by Valdivia. 5,11,13,14,16,25,26
What is the situation in 2010? Although PCNL is a common urological procedure, a recent survey showed that 11% to 56% of the urologists performing PCNL routinely in the United States and Europe obtained percutaneous access themselves. 30 –32 In this situation, percutaneous access is mostly performed by radiologists the same day or some days before the PCNL and is traditionally performed in the prone position. As a consequence, it is extremely difficult to obtain large-scale randomised trials.
A recent review concluded that “urologists are recommended to perform PCNL in the position that is most familiar to them.” 16 Although this cannot be considered scientifically sound advice, the lack of data from large-scale, randomised, and controlled trials could justify this conclusion.
The pure supine or the Galdakao-modified supine Valdivia positions have several potential advantages over the prone position. They are less demanding and time-consuming procedures, are more comfortable for both patient (less anesthesiological risk, reduced fluid absorption) and surgeon (reduced X-ray exposure, “sitting” procedure), and allow a simultaneous retrograde approach to the ureter and renal pelvis, with both rigid and flexible scopes, for contemporaneous treatment of ureteral and/or complex renal stones. They can reduce the number of access tracts (and related morbidity), as stones located in unreachable locations may be relocated by a flexible scope and fragmented through the single nephrostomy tract. 7,33 In the end, we must keep in mind the goal of the surgeon performing PCNL: “to completely remove the stone with less invasivity.”
The risk of colon injury during access to the renal collecting system, with the patient prone or supine, has been studied by Hopper et al. 28 In a series of 500 abdomen computed tomography scan, the frequency of a retro-renal colon increased from 1.9% to 10% depending on the supine or prone position, respectively. About 50% of the patients had a more posterior colon in the prone position compared with those in the supine position at the same level, with an average movement of the colon of 12 mm posteriorly. Although colon injuries occurred rarely with both techniques, performing PCNL in the prone position may increase the risk. However, one should keep in mind that obtaining a preoperative computed tomography scan, performed in the same position used for PCNL, and the use of ultrasound to access the kidney may minimise the risk of colon injury, irrespective of whatever position is used.
The ability to perform the Endovision technique to access the kidney has advantages not only in terms of potentially less bleeding (due to a perfect puncture of the calyx) but also in terms of direct control of the puncture, dilation and position of the Amplatz sheath, and the creation of a rapid through-and-through (percutaneous-urethra) access to the urinary collecting system. 34 These allow a standardisation of the technique to minimise complications. Moreover, it could be considered a fundamental step for the training of residents, allowing them to better understand the complex anatomy of the renal cavities, to better approach the calyx, and to become more familiar with the retrograde approach to the kidney with a flexible ureteroscope.
Conclusion
The prone position should still be considered an adequate position for PCNL with more than 30 years of successful experience in treating all types of kidney stones. It represents the standard to which other positions should be compared. However, the pure supine or the Galdakao-modified supine Valdivia positions have potentially important advantages for both patients and surgeons that need to be investigated in a large randomised trial to define their superiority over the traditional prone position.
Footnotes
Acknowledgments
The authors gratefully acknowledge Dr. Gaspar Ibarluzea and Dr. Mikel Gamarra for illustrations.
Disclosure Statement
No competing financial interests exist.