
Abstract
Robot-assisted minimally invasive surgery has become a routine surgical option for the treatment of prostate cancer. Despite its technical advancements, the da Vinci® Surgical System still lacks haptic feedback to the surgeon, resulting in a maximally applied compressive force by the robotic needle driver during every grasping maneuver. Without this perceptional sense of touch and grip control, repetitive robotic needle driver manipulation may unknowingly lead to irreparable damage to fine sutures used during delicate anastomotic repairs. For robotic prostatectomy, any such loss of integrity can potentially lead to premature breakdown of the urethrovesical anastomosis and urine extravasation, especially important for a less-than-perfectly fashioned anastomotic repair. Although it has already been established that overhandling of sutures using handheld laparoscopic instruments can lead to reduced suture strength, it has not been established to what extent this may occur after robotic surgical procedures.
We present analytical data and analyses concerning the failure strength of fine sutures commonly used for urethrovesical anastomotic repair during robotic prostatectomy, after repetitive robotic needle driver manipulation. When compared with noncompromised monofilament suture controls, the average maximal failure force after repetitive robotic manipulation was significantly reduced by 35% (p < 0.0001). Similarly, the average maximal failure force of braided sutures was significantly reduced after repetitive robotic manipulation by 3% (p = 0.009).
This work demonstrates that significant reductions in monofilament and braided suture strength integrity can occur after customary repetitive manipulation by robotic needle drivers in an ex vivo model, with further research warranted in the in vivo setting.
Introduction
Breakdown of the urethrovesical anastomosis during robotic prostatectomy, secondary to failure in suture integrity, could potentially jeopardize the outcome of the repair. Theoretically, such an occurrence would be most noteworthy in the setting of the novice surgeon having limited experience in fashioning an already-compromised anastomosis, or for the experienced surgeon during a technically challenging anastomosis. Although it is well known that overhandling of suture materials with handheld surgical instruments can lead to weakening of the suture integrity, 11,12 the extent to which this may occur after robotic needle driver handling has yet to be determined.
While the principal scope of this study was not to test the clinical relevance of such an episode, the aim was to determine if repetitive suture handling performed by the da Vinci robotic large needle driver, as is customary during robot-assisted radical prostatectomy, can affect the strength integrity of commonly used synthetic absorbable sutures.
Materials and Methods
Sutures commonly used for urethrovesical anastomotic repair were procured through an in-kind donation (Syneture; U.S. Surgical, Inc., Norwalk, CT) and consisted of nonexpired monofilament (3-0 Biosyn™) and braided (3-0 Polysorb™) synthetic absorbable sutures. However, because of its inherently smooth external surface feature and its associated capacity to mitigate bacterial infection, the nonbraided monofilament variety is the most commonly preferred suture for robotic urethrovesical anastomotic repair.
To more effectively declare true statistical insignificance if, indeed, no differences were observed between the suture groups, the authors chose a more stringent power analysis with a beta of 0.05 (95% power) instead of a more customary beta of 0.20 (80% power). On the basis of the above power analysis, four suture groups containing 28 suture specimens each were created (see Fig. 1).
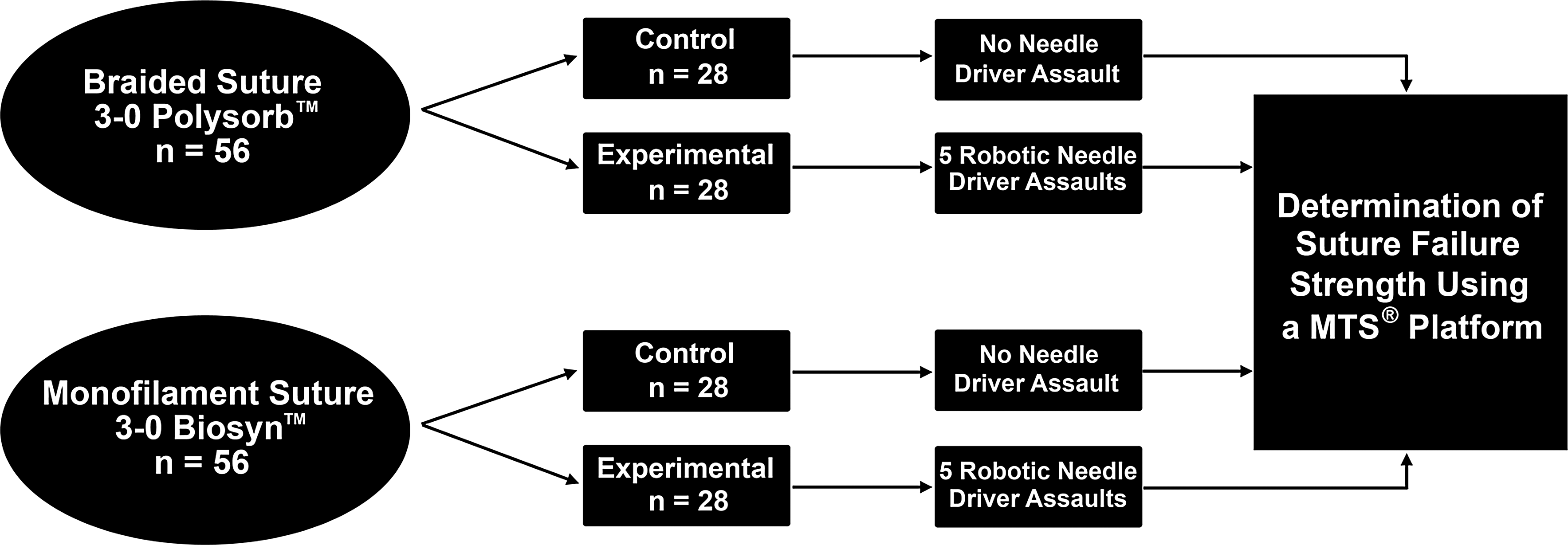
Diagram illustrating the experimental design using 3-0 Polysorb™ and 3-0 Biosyn™ suture material.
With all testing performed under dry air (nonsoaked) conditions, two of the groups consisted of experimental braided and monofilament sutures to which each suture incurred five repetitive da Vinci large needle driver grasping assaults. In preparation for the robotic grasping assaults, each suture specimen was cut to a length of 17 cm, individually threaded within two separate 3-cm sheaths of 1/16-inch thin-walled heat-shrink tubing (previously heat shrunken), of which were threaded within two 1.7-cm-long rubber sterilizer support bushings (Steris Corporation, Mentor, OH). The suture material was secured by crimping no. 5 and no. 7 split shot weights (Eagle Claw Fishing Tackle, Denver, CO) at each terminal end of the suture/heat-shrink tubing complex (see Fig. 2). To effectively allow for a 5-cm length of exposed suture for robotic grasping, each rubber support bushing was secured within customized jig holders engineered to seize each end of the suture construct without causing any intrinsic damage to the suture (see Fig. 3A, B).

Representative image showing the final preparation of the suture materials used for both the da Vinci® large needle driver assaults and suture strength analysis.
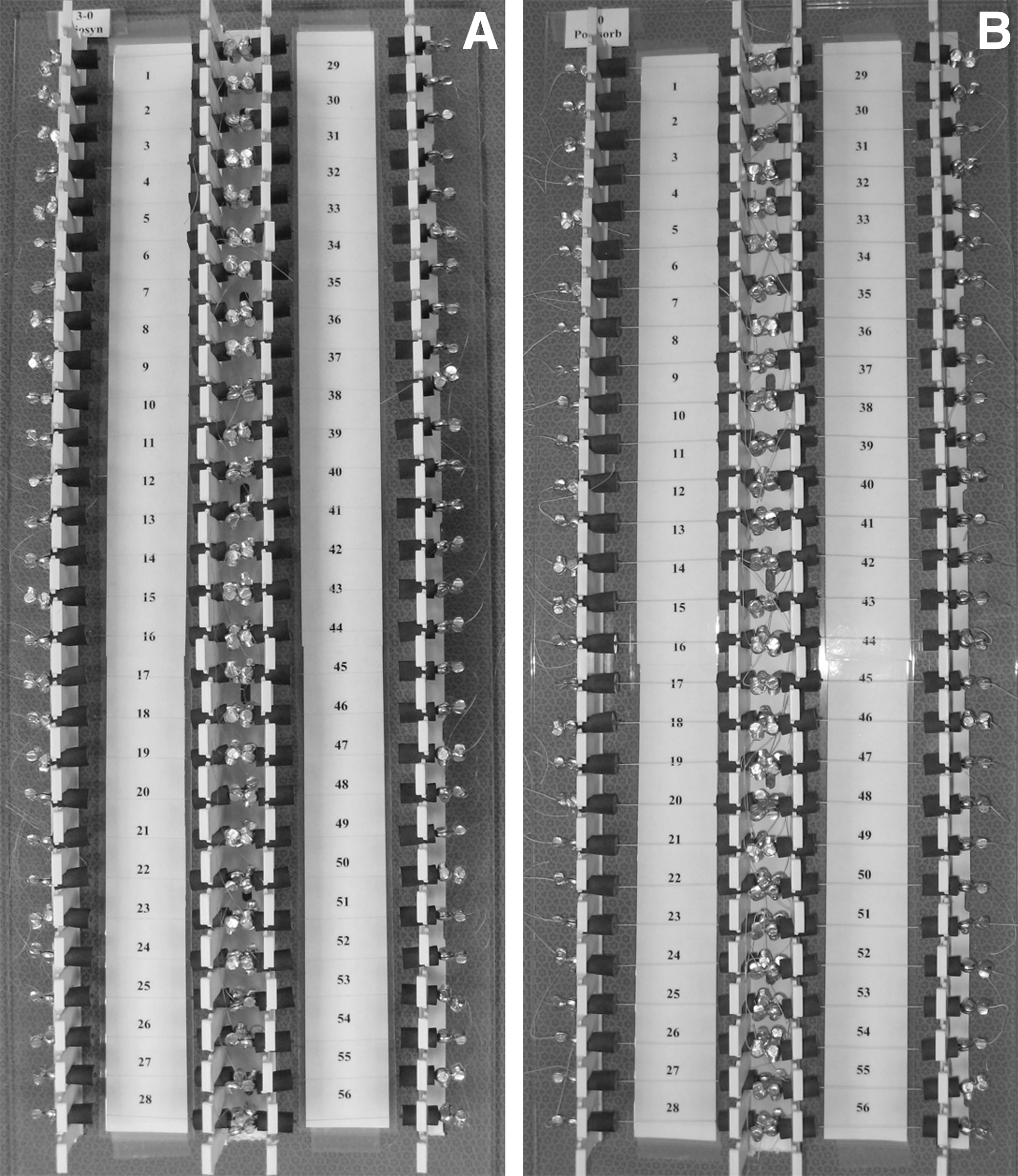
Representative images of the customized jig holder used to stabilize the monofilament suture material (
The two remaining suture groups consisted of control specimens containing identically matched suture material to that of their experimental counterpart (28 monofilament and 28 braided), prepared in an identical fashion, and to which incurred no needle driver grasping assaults.
For the 56 specimens identified for robotic grasping manipulation (28 monofilament and 28 braided), the da Vinci large needle driver was positioned to perform five separate grasping maneuvers along the 5-cm length of exposed suture (see Fig. 4). After the needle driver grasping assaults, all specimens (experimental and matched control) were transported to the laboratory for tensile testing.

Representative image showing repetitive da Vinci large needle driver assaults.
Blinded to the specimens incurring robotic grasping assaults, the authors performing the tensile strength analysis randomly loaded the matched set of suture specimens onto a MTS® (Eden Prairie, MN) platform that consisted of a hydraulically controlled ram and a previously calibrated dynamic load cell (see Fig. 5). Under displacement control and with a pull speed of 2 cm/second, the sutures were pulled apart to failure, and the maximum failure force and displacement of each was recorded.
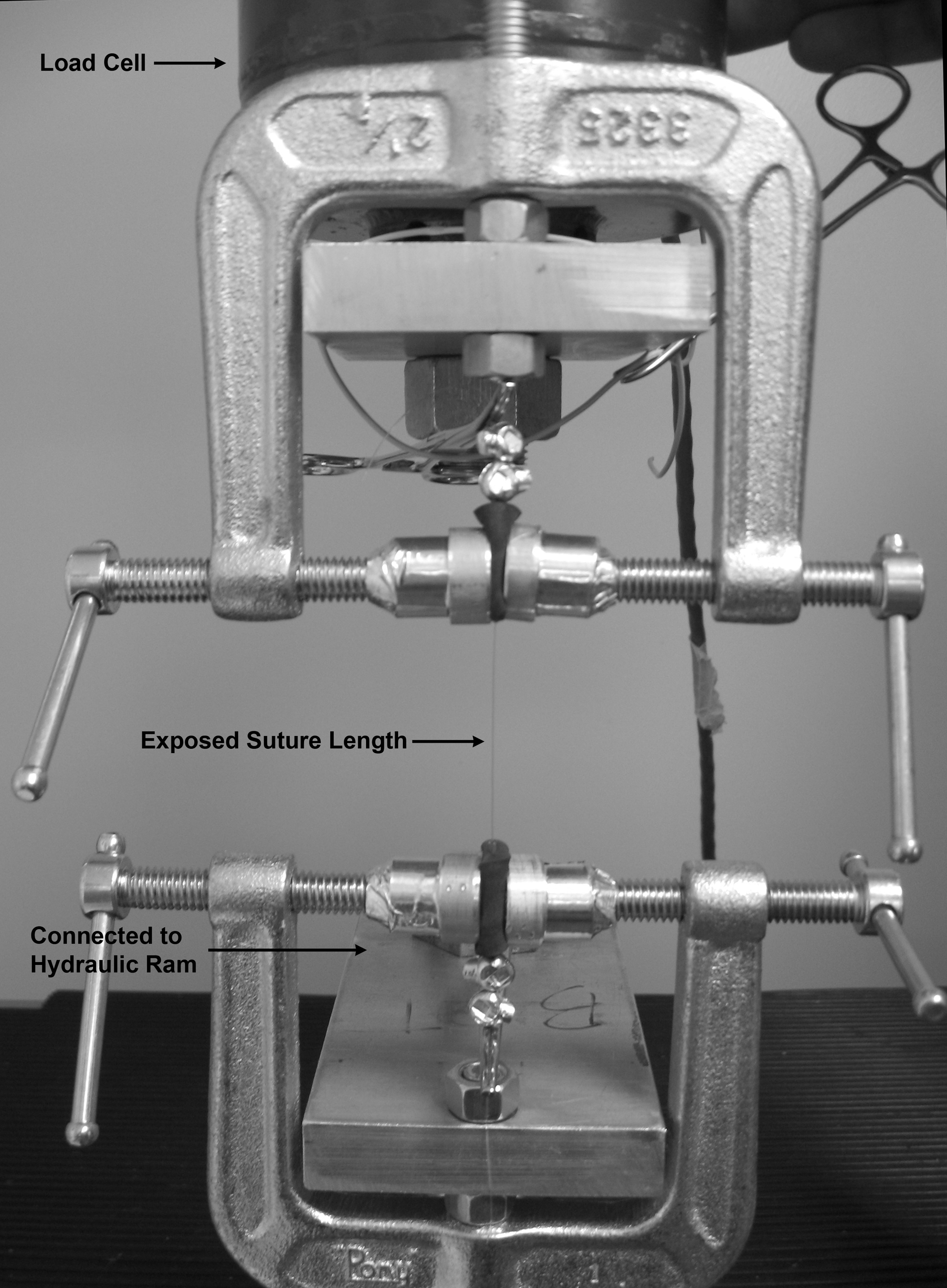
A representative illustration of a suture test specimen loaded onto the MTS® testing platform before failure strength evaluation.
An analysis of variance, blocking on the suture, was performed, and a post hoc Tukey standardized range test was used to evaluate the main effect of the suture failure. Significance was accepted at p < 0.05.
Results
Failure strength results are summarized in Figure 6. The analysis of variance indicated that repetitive manipulation by the da Vinci large needle driver significantly decreased the suture strengths of both the monofilament (p < 0.0001) and braided (p = 0.009) materials, with the most commonly preferred nonbraided monofilament suture suffering the greatest strength reduction. For the monofilament suture group, the average maximum force (failure point) for the control group was 58.0 ± 3.5 N, and 37.5 ± 5.3 N for the robotically manipulated group; demonstrating a 35% reduction in suture strength after robotic manipulation. For the braided suture group, the average maximum force (failure point) for the control group was 55.3 ± 1.4 N, and 53.9 ± 2.4 N for the robotically manipulated group, demonstrating a 3% reduction in suture strength after robotic manipulation.
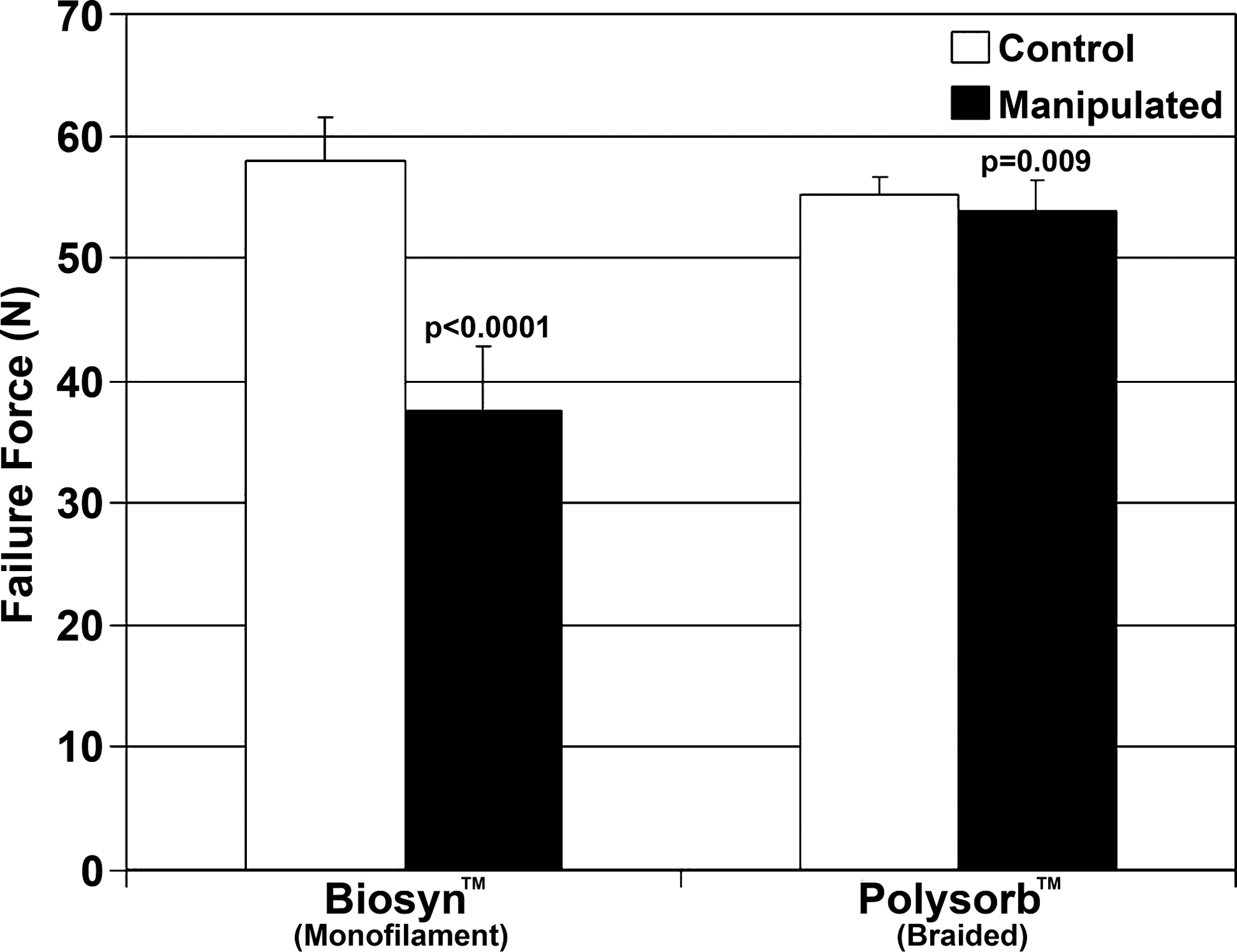
Graphical results of the noncompromised (Control) suture material versus the suture material incurring repetitive da Vinci large needle driver grasping assaults (Manipulated). Note the significant decrease in the suture strength integrity of the suture most commonly used (monofilament suture) for the urethrovesical anastomotic repair during robot-assisted radical prostatectomy.
Discussion
The acceptance and use of robotic surgery has greatly increased over the last decade. Advantages include decreased length of hospitalization, decreased postoperative pain, reduced blood loss, faster recovery, and fewer complications. 13 For robot-assisted prostatectomy, one of the most technically difficult and challenging aspects of the procedure is the fashioning of the urethrovesical anastomosis. Factors that can contribute to a poor anastomotic repair include, but are not limited to, the condition of the anastomosis (i.e., already compromised), comorbidity factors (i.e., diabetes or steroidal use), anatomic patient variations (narrow pelvis, large prostate gland, wide bladder neck, etc.), and the robotic experience of the surgeon.
The level of robotic surgical experience can range from limited to vast. The novice robotic surgeon, one who may be prone to mishandling of both the delicate tissues and suture materials, typically struggles to fashion a tension-free anastomosis, relying heavily on the integrity of the suture. Further, in the setting of an already compromised anastomosis, the ability of the suture material to maintain its integrity may play an even greater role in the overall quality of the repair. Even in the hands of an experienced surgeon, comorbidities or anatomic variations can contribute to a less-than-ideal anastomotic repair. Anytime a less-than-desirable anastomotic repair exists, any premature breakdown of the suture may contribute to urine extravasation and delayed healing. This can result in prolonged need for catheterization, patient discomfort, extended hospital stay, increased medical costs, and a possible increased risk of long-term anastomotic stricture formation. Presently, it is difficult to ascertain the amount of irreparable suture damage that may occur after robotic suture manipulation during the urethrovesical anastomotic repair. 14,15 To our knowledge this is the first attempt to analytically determine the amount of damage sustained to fine absorbable sutures after repetitive manipulation by the da Vinci large needle driver, a preferred instrument of choice for robotic radical prostatectomy.
When using the da Vinci large needle driver to handle the suture, results from this study show a statistically significant reduction in suture strength integrity after repetitive grasping assaults, with the most commonly favored suture material (the nonbraided monofilament) exhibiting the greatest strength reduction. After applying five separate needle driver grasping assaults along a 5-cm length of suture, we have attempted to conservatively approximate the in vivo conditions encountered during routine urethrovesical anastomotic repair. However, the authors urge that this approximation may vary greatly among surgeons, or be dependent upon the procedural learning curve and surgical robotic experience, with grasping assaults over a given area of suture easily exceeding this study's estimation, a condition that may result in an even greater loss of suture integrity.
While it is uncertain if these statistically significant strength reductions are clinically relevant, surgeons performing robotic prostatectomy should be mindful, especially when using fine monofilament sutures, that repetitive manipulations using the da Vinci large needle driver, an instrument that exerts a maximum closing force during each grasping maneuver, can significantly diminish the strength of the suture. More importantly, any such loss in suture integrity could potentially jeopardize the integrity of the anastomotic repair. Nonetheless, whether this diminution in suture integrity is transferable to in vivo conditions, that is, after the expected hydrolytic degradation of the absorbable suture materials, is yet to be established and warrants further investigation.
Footnotes
Acknowledgments
This work was supported by the Summa Foundation. The authors would also like to thank Jerry VanStavern of Syneture (a subsidiary of U.S. Surgical, Inc.) for the in-kind donation of the Biosyn and Polysorb suture materials.
Disclosure Statement
No conflict of interest or competing financial interest existed for any of the authors associated with this study.