
Abstract
Introduction:
Despite improvements in instrumentation and technology in flexible ureteroscopy, the issue of procedural and off-procedural damage remains a problem. The aim of our study was to highlight our initial experience in flexible ureteroscopy using polyscope, a new advancement in the era of flexible ureterorenoscopy.
Materials and Methods:
In this study, we used an 8F modular flexible, steerable polyscope for diagnostic purposes and Dormia basket removal for small renal stones. Three outer disposable catheters were used with proper sterilization in 22 cases.
Results:
The polyscope was used in six cases of undiagnosed hematuria, and biopsy was taken from pelvic growth in one patient, which turned out to be transitional-cell carcinoma. Polyscope was used for removal of residual stones or small stones (<1 cm) using Dormia basket in 16 cases (from August 2008 to July 2009). The mean stone size was 7.5 mm. The vision achieved was excellent in all the cases.
Conclusions:
Minimally invasive techniques are preferred for treatment of renal stones. The problem of lower caliceal stone access has been solved with the primary and secondary deflection of modern flexible ureteroscopes. The modular design of polyscope makes it a more cost-effective option. Relatively cheap and disposable multilumen catheters preclude the need for sterilization of optic cable, thus decreasing the chances of handling-related damages. The chance of instrument-related infection is minimal. Besides, it can be used as a semirigid ureteroscope should the need arises.
Introduction
Materials and Methods
Twenty-two patients were enrolled in the study carried out for over 1 year, of which 6 cases required diagnostic ureteroscopy and 16 cases required use of Dormia basket for stone removal. Three multilumen catheters were used in these 22 cases.
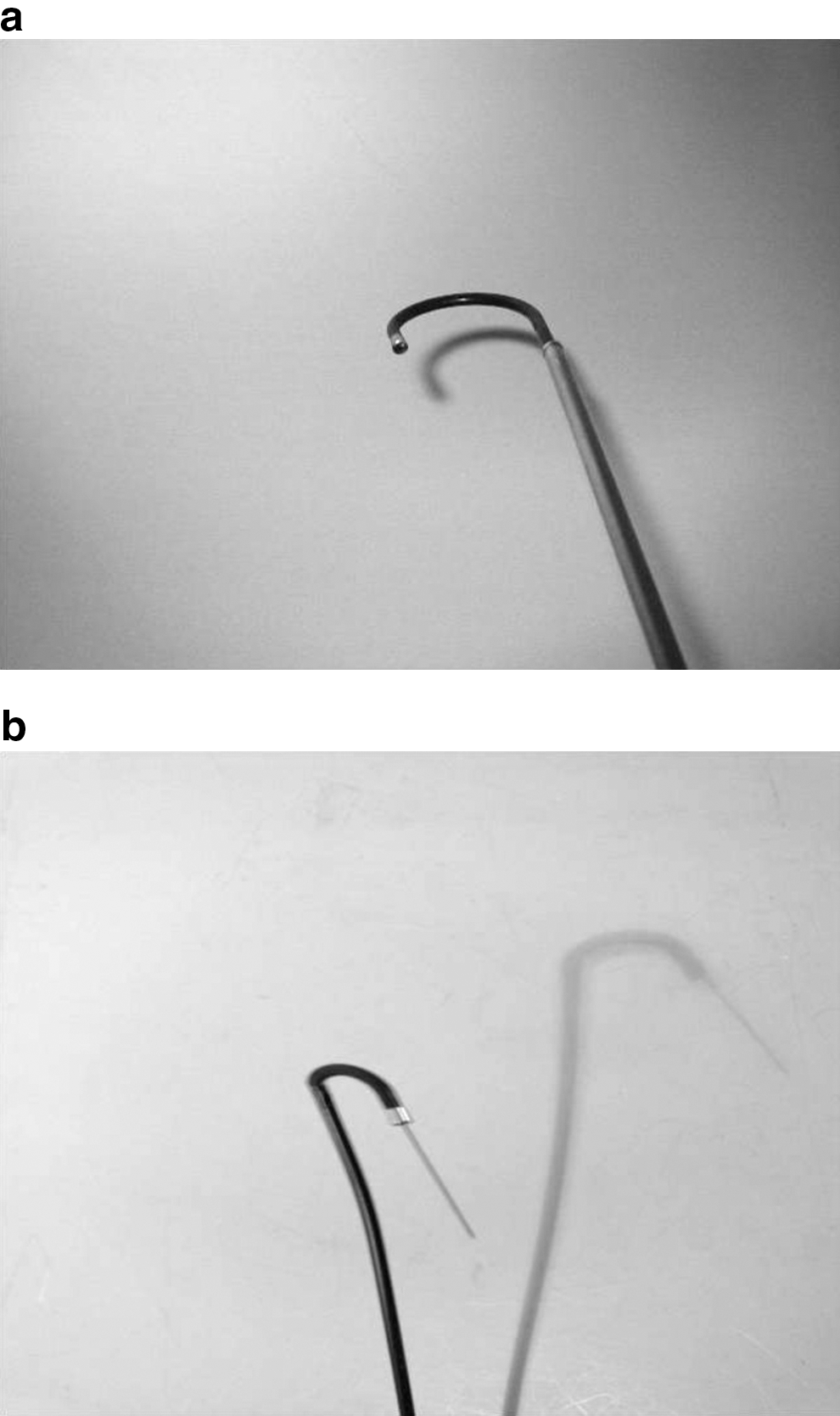
A polyscope is basically a modular flexible ureteroscope having an outer diameter of 8F (2.65 mm), a working channel of 3.5F (1.2 mm), and a length of 85 cm. A polyscope has the following parts (Fig. 1): (1) Steerable, rotatable, multilumen endoscopic catheter with four channels, having active deflection up to 180° with instrument in situ (Fig. 2a, b). (A) Optical channel (B) Channel for attachment of light cord (C) Working channel (D) Channel for steering mechanism (2) Protection tube for the optics (3) Optics with resolution of 10,000 pixels with length of 1500 mm inserted in the optic dispenser, providing 0° direct view with 70° field of vision (4) Combishifter (combined opticshifter and length compensator) (5) Modular eyepiece (6) Disposable steering handle
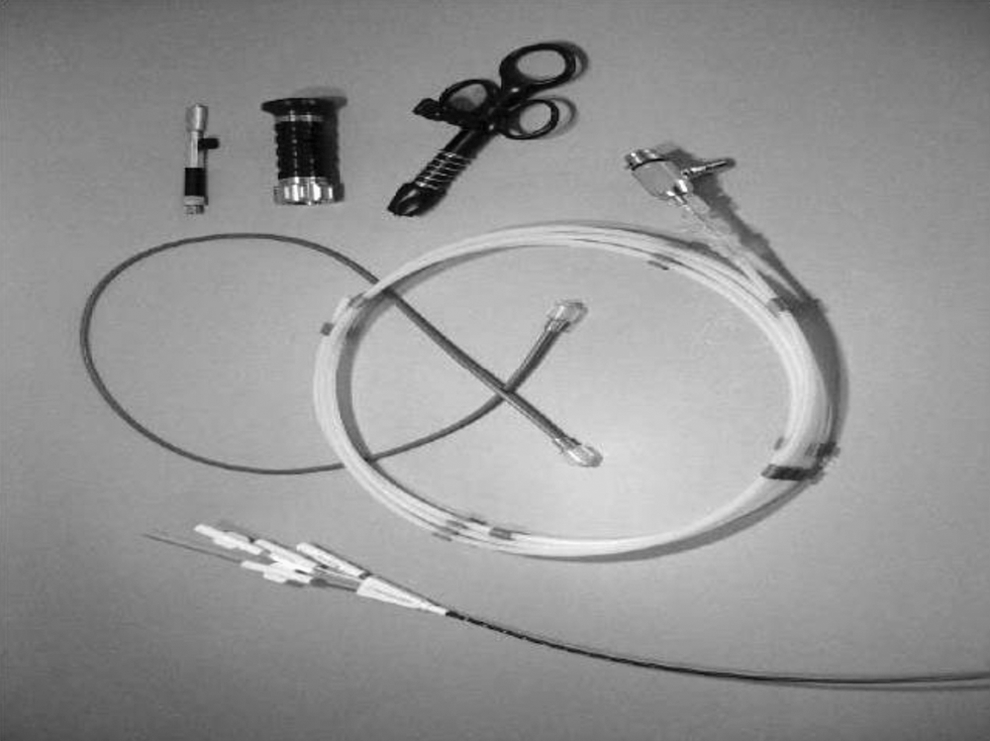
Parts of polyscope from below (anticlockwise): multilumen catheter, optics in its carrier, steering handle, modular eyepiece, optical body with optical combishifter, and optical protection tubing.
Supplementary devices: (1) Monitor (2) Xenon light source (3) Video camera (4) Three-joint arm (5) Chiriflex—the special rigid accessory, by which the flexible polyscope can work as a rigid or semirigid ureteroscope
Accessories: Y adapter for irrigation Biopsy forceps Cytology brushes Grasping forceps Stone-grasping baskets (3F, 120 cm)
Assembling of polyscope
The three-joint arm was installed, which has the following three parts: (A) Vario-arm (B) Table clamp (C) Camera mount
These are assembled and mounted on the table. The camera system is mounted and it is connected to modular eyepiece, which in turn is connected to optic combishifter with the optics dispensed in optic dispenser.
Preparation of optics and scope
Optics is taken out of its dispenser and adjustment of optic dispenser is done. Optics is carried out through the outer protection tubing and then through the disposable polyscopic catheter (Fig. 3). Light source is connected through its cable to the channel for the light source in the multilumen catheter.
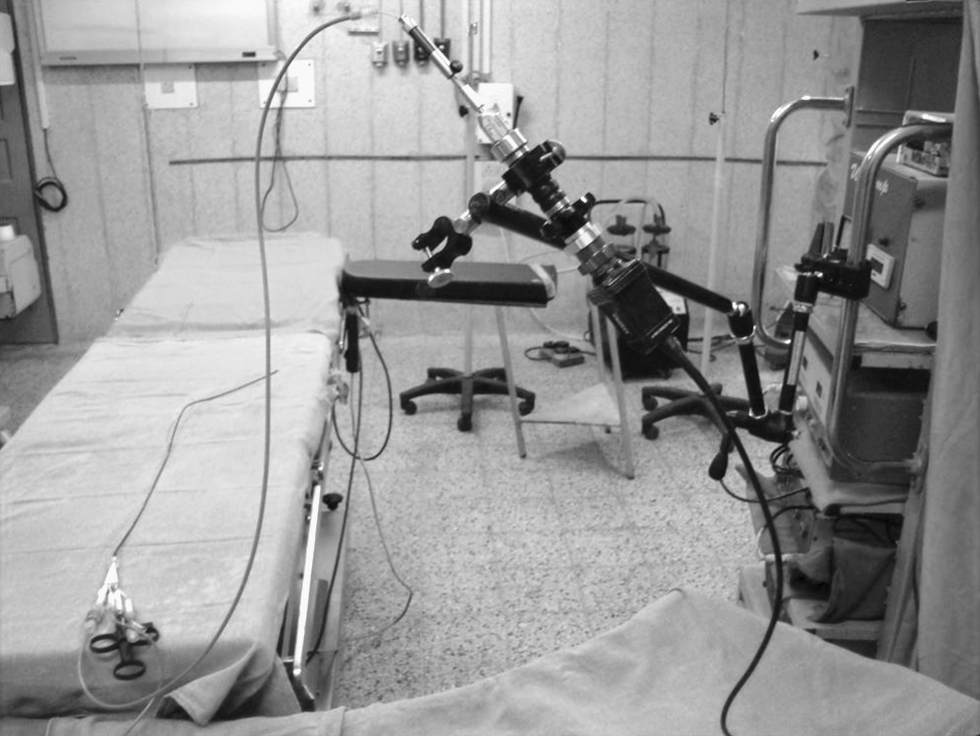
Assembled polyscope with its optics passed through the multilumen catheter connected to protection tubing, which is attached to optical body and eyepiece with camera.
Sterilization
Multilumen catheters come in presterilized packs, usually by ethylene oxide. If reused, these can be sterilized by conventional means such as using formaldehyde or ethylene oxide. Optic combishifter is autoclaved. There is no need to sterilize the optics; simple rinsing of the optic dispenser containing optical cable with plain water is sufficient. Before inserting the optical fiber into the polyscope catheter, it is gently cleaned with soft tissue.
Procedure
Patients were enrolled after acquiring their informed consent. Preoperative sterile urine culture was ensured. Prior ureteral stenting was done in necessary cases such as those with multiple fragments. The polyscope was assembled as described earlier. The procedure was carried out in lithotomy position. Prior guidewire was introduced into the desired renal unit with the help of a rigid cystoscope. The polyscope was inserted either over the guidewire or using a ureteral access sheath or chiriflex. Position was confirmed with the help of an image intensifier. Irrigation was done with help of a Y adapter when the working channel was occupied with the instrument. Small stone fragments were removed by nitinol Dormia basket. Postprocedural stenting was done if there was procedural trauma, where access sheath was used, or in cases with multiple fragments. If the multilumen catheter was reused, it was properly sterilized and the same was confirmed by doing swab culture from the catheter tip.
Our use of the polyscope so far has been mainly for diagnostic applications and Dormia basket removal of residual stones after extracorporeal shockwave lithotripsy or percutaneous nephrolithotomy.
Results
We used the polyscope in six cases of undiagnosed hematuria. Biopsy was taken from one of these patients, which turned out to be transitional-cell carcinoma of renal pelvis. Washings from renal pelvis were taken from another patient suspected to be having transitional-cell carcinoma, which later turned out to be hilar renal-cell carcinoma. We removed residual stones or small stones <1 cm using Dormia basket in 16 cases since August 2008. The mean stone size was 7.5 mm. Prior Double-J stenting was used in six patients while postprocedural stenting was required in three patients. Polyscope afforded excellent vision in all the cases. One multilumen catheter was used with proper sterilization for a mean number of 7.3 cases (3 in 22 cases) without any compromise of vision or added complications.
Advantages of the polyscope
As the optic channel is covered by a protective glass pane, the optical fiber does not come in direct contact with the patient, and hence, there is no need for sterilization of the optical fiber. This also results in lesser chances of infection as the polyscope has never been in contact with other patients if the multilumen catheter is not reused. Also, more number of cases can be done rapidly simply by changing the disposable polyscopic catheter.
Because of the modular nature, if some part of the polyscope needs repair, that part can be repaired on the site without the need of sending the whole instrument for repair. As the optical fiber is handled by the surgeon himself and other relatively cheaper parts such as multilumen catheter are handled by staff members, the lifespan of the instrument is increased because of lesser chances of procedural and off-procedural damages.
The optical resolution is around 10,000 pixels with resultant excellent picture quality.
The tip of the polyscope is steerable with active deflection up to 180° (Fig. 2a, b), even with an instrument in situ in the working channel. As the catheter is rotatable, it results in easy access into the inferior calix.
With proper sterilization, the disposable multilumen catheter can be reused without compromising vision, thus increasing the cost effectiveness. Polyscope costs approximately rupees 7.5 lakh Indian rupees (INR), whereas the multilumen catheter costs Rs. 35,000 (INR) per piece. We could do 22 cases using three catheters, with good vision (Fig. 4).
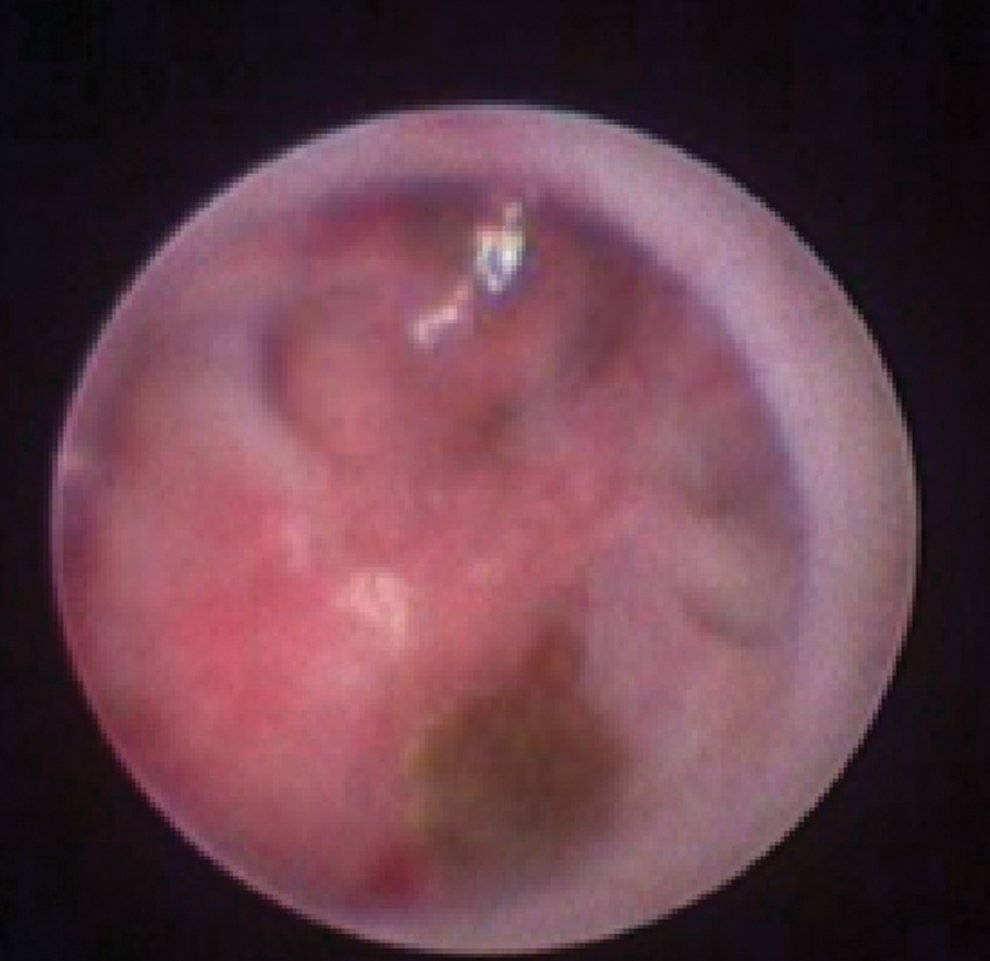
Polyscopic view using the reused catheter.
With chiriflex (Fig. 5), the instrument can be used as a rigid or semirigid ureteroscope, which adds to the versatility of the instrument (can also be used as a flexible nephroscope/cystoscope by changing the outer sheath).

The polyscope with chiriflex.
Discussion
The desired properties of an optimal flexible ureteroscope includes a good image quality, better irrigation rates, adequate maximal deflection, and long durability. A major problem with the currently available flexible ureteroscopes is the high cost of maintainance 1 and the time lost when the scope needs repair or replacement.
Since the first description of ureteroscopy by Young and McKay, 2 there have been remarkable changes with the advent of rigid, semirigid, and flexible ureteroscopes with miniaturization. The application of flexible ureteroscopy was first reported by Marshall in 1964 3 ; this ureteroscope was not capable of being directed and was not having a working channel. Bagley et al 4 developed a flexible ureteroscope with a working channel and an active tip deflection along with altered stiffness of the endoscope leading to secondary deflection.
The main problem during flexible ureteroscopy is the access to lower-pole calix, which is limited by active deflection. The problem is further compounded by the presence of instruments in the working channel. Lower-pole stone access was first reported by Grasso and Bagley. 5 Later, Grasso and Ficazzola 6 in 1999 reported a fairly high success rate for lower caliceal stones smaller than 1 cm.
Among the current models of flexible ureterorenoscopes, DUR-8 Elite by ACMI is capable of double deflection with 270° ventral deflection, whereas Flex-X by Karl Storz has 270° deflection in both the ventral as well as dorsal direction. Storz Flex-X2 ureteroscope has laser-resistant ceramic sheath. Similar scopes are available from Wolf and Olympus. DUR-D by Gyrus-ACMI has utilized the “chip on the tip technology,” resulting in better image quality. 7
Despite the ongoing improvements in technology, there is concern regarding the damages occurring due to handling of the costly endoscopes. Another area of concern is the need of sending the endoscope for repair, especially in countries with limited resources. The stringent sterilization requirements preclude more cases in succession with conventional flexible ureteroscopes. Polyscope is an innovation in these fields, with distinct advantages.
Polyscope is a flexible ureteroscope with modular design. The multilumen catheter has an outer diameter of 8F and a working channel of 3.5F. The steering component is having a luer-lock mechanism for deflection of the steerable tip of the catheter, which can also be rotated. The tip deflection is around 180°. It has an inbuilt mechanism for the attachment of the light cord. There is no separate irrigation channel and the irrigation is done using a Y adapter in the working channel, although there is another model as described by the manufacturer, which has an additional channel for irrigation, but the optical resolution is only 6000 pixels.
The optical resolution of polyscope is about 10,000 pixels. The optics are contained in optics dispenser, along with optics combishifter to adjust the length of the optics. The optic fiber passes through the optical channel of the multilumen catheter and there is an outer protection tubing, one end of which attaches to the multilumen catheter and the other end to the optical combishifter with optical body and camera system.
The whole system is mounted on the operating trolley cart by means of trio arm and tripod stand. The chiriflex allows the instrument to be used as a semirigid ureteroscope (Fig. 4).
The main advantage of polyscope is its modular design, which allows the repair of individual parts, without disturbing the other components. The optics never comes in direct contact with the patient, and the optical channel is covered by a pane of glass. So the optical fiber does not need to be sterilized. After each use, the optics can be removed from the used polyscope catheter and inserted into a new sterile polyscopic catheter. Thus, the next case can be done immediately. Modular polyscope differs from other flexible ureteroscopes in having separate optics, no need of sterilization of optical fibers, and doing cases in quick succession by simply changing the multilumen catheter. Further, there are less handling-related damages. If required, the polyscope can be used as a rigid ureteroscope.
Polyscope is manufactured by POLYDIAGNOST GmbH, a Germany-based company, and marketed by Lumenis India Pvt. Ltd.
In our experience, the multilumen catheter can be reused without compromising the visual quality or sterility parameters. The passive stenting was required in some cases so that the access sheath could be used. This study is limited by the fact that there is no direct comparison of the polyscope with conventional flexible ureteroscope in terms of image quality, irrigation rates, and lower-pole deflection. However, these parameters are comparable with the other commercially available flexible ureteroscopes. As the study included only 22 patients over the period of 1 year, queries about the durability of polyscope cannot be answered, especially without the use of the laser, although it seems to have an edge over other flexible scopes by virtue of compartmentalization with separate optics. The aim of the present study was to share our experience on this new device and have feedbacks from other centers so that its utility and superiority can be assessed and verified.
Conclusions
Minimally invasive surgery is preferred by patients with renal stone because of excellent stone clearance and low morbidity. The problem of lower-pole access has been addressed by the primary and secondary deflection properties of flexible ureteroscopes. Modular design of the polyscope makes it a better and more cost-effective option. As disposable multilumen catheter is a relatively cheap part of the instrument and the expensive optical fiber is handled by the surgeon himself, there is less chance of handling-related damage to the optical fiber. In our limited experience, polyscope has proved its efficacy and utility in terms of durability, economy, and optical quality. However, the instrument needs to be assessed over a longer period of time and in larger number of patients at different centers before its perceived advantages can be reliably validated.
Footnotes
Disclosure Statement
No competing financial interests exist.