
Abstract
Introduction:
The endoscopic deployment and extraction of endoluminal stents, such as ureteral stents, is commonplace in contemporary medical management of many diseases. In a hemorrhagic environment, endoscopic identification of a stent can be challenging. To date, no study has evaluated the optimal color for endoscopic stent identification.
Methods:
Eight different colored stents were placed in a simulated bladder model. Each stent color was evaluated in saline and three progressively more concentrated bloody environments. A flexible cystoscope was used to make 15-second video clips of the stents in each environment. Participants viewed the videos in a random sequence. Participants were asked to identify the color of each stent, and rate the identification on a 10-point scale. Logistic regression models were used to model the relationship between identification, stent color, environment, and experience.
Results:
Forty-seven participants reviewed the videos. In clear and mildly bloody environments, blue stents had the highest identification (p < 0.06, p = 0.001, respectively). In moderately bloody environments, yellow stents had the highest identification (p < 0.01), whereas silver stents had the highest identification in severely bloody settings (p = 0.004). Blue and green stents were identified most commonly and received the highest identification scores in all environments. Level of training and experience with endoscopy were not significantly associated with the correct response rate.
Conclusions:
This study demonstrates that the color of a stent plays an important role in endoscopic identification. Our results suggest that blue and green colors offer superior visibility in both clear and hemorrhagic environments.
Introduction
Stent design elements such as type of material, length, anchoring mechanism, and ease of manipulation are being studied extensively as important safety features. 2,3 For example, encrustation of the indwelling stent is a common complication that can lead to increased patient morbidity 4 ; by changing the material that the stent is made from to more biocompatible materials or to include coatings that resist encrustation, the number of associated complications has decreased. 5
Both placement and extraction of the stent requires the surgeon to first identify the stent, usually under direct cystoscopy. Although typically this is a simple task, a bloody environment can complicate identification of the stent. 6 Poor stent identification can lead to increased procedure time or even require secondary cystoscopy. The associated increased cost or increased patient discomfort related to longer procedures makes ready identification of the stent even in bloody environments a priority for the surgeon. 7 An aspect of stent design that can be directly controlled and may lead to better identification is appropriate selection of the color of the stent to be placed. To our knowledge, there has been no prior evaluation of the ease of identification of stents as differentiated by color.
The purpose of this study was to consider the impact of color on ease of identification of the ureteral stent in challenging environments (e.g., different amounts of hemorrhage). We believe that the information gained in this study extends beyond the field of urology. Endoscopic identification of color can be used by any specialty, such as gastroenterology and gynecology, where endoscopic technology is utilized. We clearly see a future where endoscopic color discrimination may be relevant. By understanding which stent color is most easily identified in a compromised liquid endoscopic environment, we hope to help clinicians minimize risk. In urology, for example, at the termination of many ureteroscopic cases, bladder identification is somewhat compromised by blood and debris. Complications such as inadvertently nudging a ureteral stent into the ureter are more likely to occur with compromised vision. Better stent identification may help to minimize this and other complications of endoscopy.
Methods
A bladder model submerged in saline was used to simulate the surgical environment. A single ureteral stent was placed in the usual fashion in the bladder model. Eight different colored stents were used: white, gray, silver, purple, yellow, blue, green, and pink. The stents were otherwise identical in size, shape, and construction (Fig. 1).
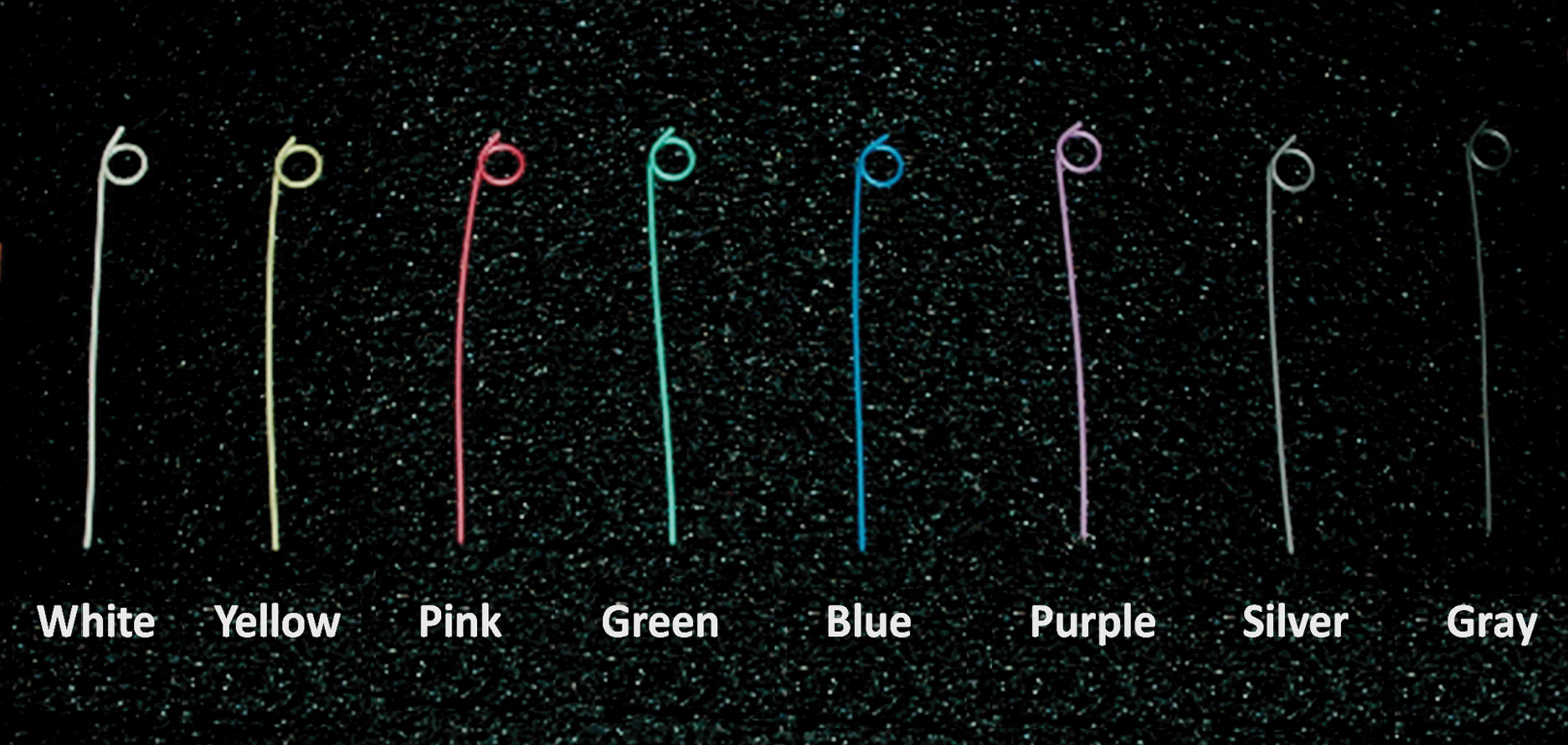
Colored stents.
Four separate environments were simulated by varying the concentration of blood in saline: clear (saline without blood), mildly bloody (1 mL of blood in 600 mL of saline), moderately bloody (2 mL of blood in 600 mL), and severely bloody (3 mL of blood in 600 mL).
A distal sensor flexible cystoscope (DCN-2010; Gyrus ACMI, Southborough, MA) was then used to record video of each stent. Exactly same stent model was placed into the bladder model with exact same protruding length, and video was recorded from the same video angle for all stents. Each video was reviewed by a urologist to ensure a realistic environment had been simulated. The videos were each 15 to 20 seconds in duration. The computer file properties of the video were tagged to reflect the color of the stent and environment. This information was not available to participants.
Participants from our department of urology (medical students, residents, and attending physicians) were invited to review the videos and complete a survey (Fig. 2). Each participant was asked to review all of the videos, presented in a random sequence by a research staff member, to describe the color of the stent seen, and the subjective ease of identification of the stent on a 10-point scale (10 for best identification).
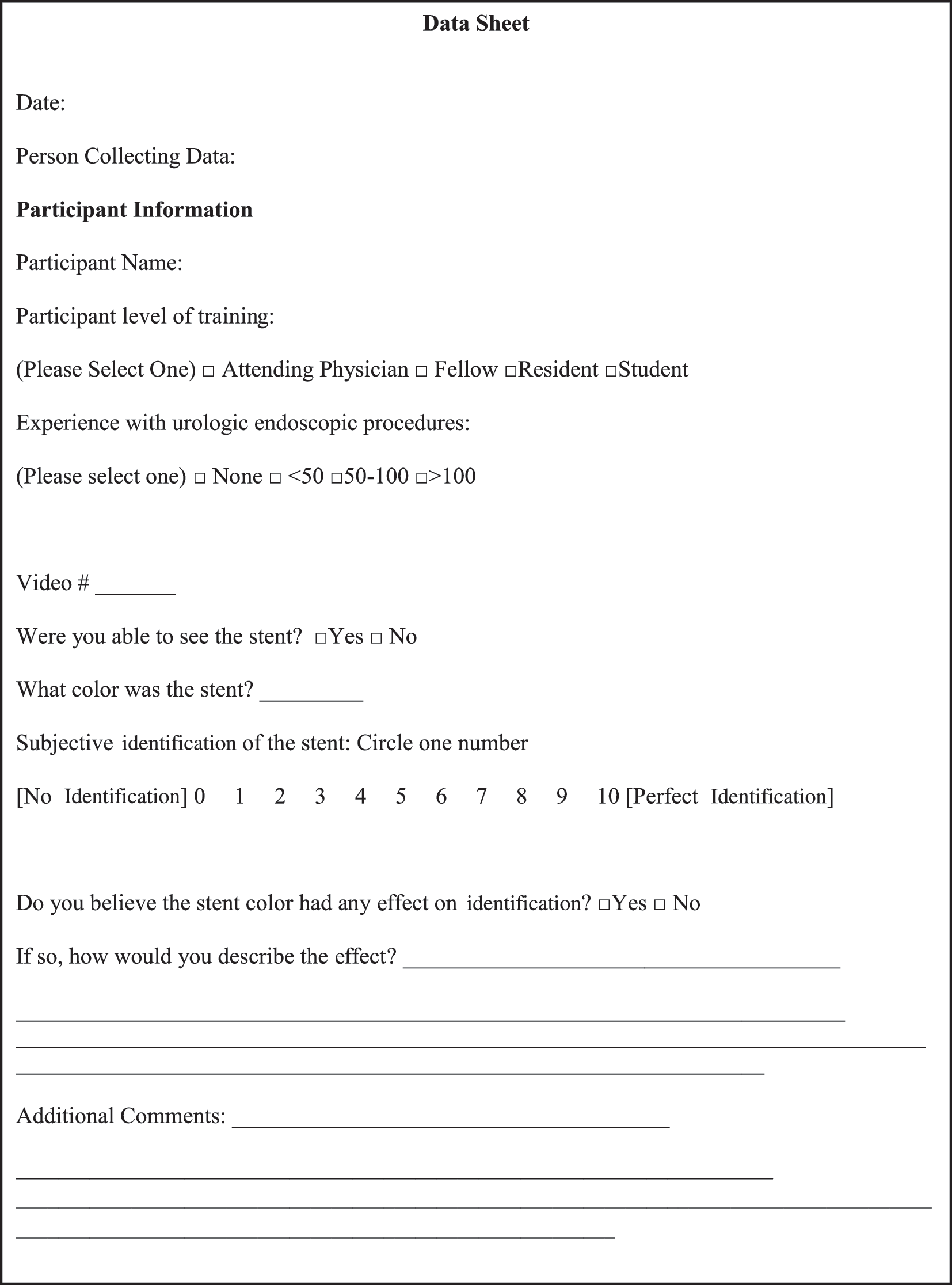
Study questionnaire.
Logistic regression models were used to model the relationship between identification, stent color, environment, and experience. A p-value of <0.05 was considered statistically significant. A research staff member collected the results, compiled the data, and analyzed the data using STATA statistical software (StataCorp, College Station, TX).
Results
A total of 47 members of the urology department participated. Accuracy of identification of stent color and mean identification scores for each stent were tabulated.
The mean identification scores for all the environments were significantly higher for blue and green stents compared with other colors (analysis of variance, p = 0.004; Fig. 3a). For the clear saline, blue stents had the highest identification scores (p < 0.06), and for the mildly bloody environments also blue stents had the highest identification score (p = 0.001). In the moderately bloody environment, yellow stents had the highest identification score (p < 0.01). Silver stents had the highest identification in severely bloody settings (p = 0.004; Fig. 3b).

(
After adjusting for environment, experience with endoscopy, stent color, and level of training, the environment and stent color remained independent predictors of correct stent color identification.
Participants were able to correctly identify blue and green stents most commonly (68.5% and 56.8%, respectively; p < 0.001). Blue stents were the most likely to have correct color identification (p = 0.01). Neither endoscopic experience nor level of training was shown to be statistically significant for accurate identification of the stent.
Discussion
Endoscopic procedures such as the placement and extraction of ureteral stents have continued to increase as a result of widened indications for the ureteral stent. 8 –10 The challenges of stent identification during these procedures, especially common complications such as gross hematuria, have made the design element of color an important consideration.
The present study demonstrates that both stent color and the endoscopic environment are statistically significant independent predictors for accuracy of identification of a stent and determination of its color. Regarding endoscopic identification of the actual color of a stent, this metric is not currently clinically important. However, in the future, it is feasible that endoscopic identification of stent or other endoluminal equipment may have some relevance. The present study demonstrates that blue and green stents are the most readily identified.
A more important clinical metric is the ability to identify and target a stent that has been deployed. In prior studies in optics, Brainard and Maloney 11 reported that the ability to identify an object is affected by the degree of illumination of the field, the spectral properties of the light source, and the layout of the objects in the environment. Similarly, Quayle and colleagues 12 have demonstrated that the type of endoscope being used affects identification. Our study did not attempt to demonstrate whether or not ease of identification and accurate color identification correlated with different types of cystoscopes. The present study refers only to distal sensor optics, which was used in this evaluation. It is unclear if the results would be different with fiberoptic technologies. Now that this has been demonstrated, further research may be done to consider different types of cystoscopes. However, as fiberoptic technologies will likely become increasingly rare in the near future, we did not test them.
Human visual processes need the color information of scenes and objects to process targets in scenes to which they cannot respond directly, irrespective of their attentional resources. Otsuka and Kawaguchi 13 examined whether color and grayscale natural scenes presented peripherally and ignored would be categorized using a negative priming paradigm. They focused on attentional resources allocated to natural scenes and direct versus indirect processing of them. Participants were required to detect and categorize the target objects in natural scenes in a central visual search task, ignoring peripheral natural images in both the prime and probe displays. Their results indicate that, in a situation in which participants indirectly process natural scenes, color information is critical in object identification and categorization. Sadly, to date, the ophthalmologic literature has not addressed vision as a function of distal sensor endoscopy. This will very likely be an important aspect of future research.
The data from the present study demonstrates that the color of an object and the environment in which it is evaluated affect the accurate perception of the color of the object of interest and the ability to identify the object. The effect of color is important for the reason that objects are similar to the scenes, and so this information plays an important role to identify targets in different scenes. Our study is consistent with the review of Tanaka and Presnell 14 about the color effects. Color information merely provides information about shape of the objects. Collectively, their findings provide further support for the role of surface information in object recognition.
Future stent design should take into account the color of the stent, in addition to factors that may improve the identification of the stent in different environments. The results of this in vitro evaluation suggest that blue and green stents are the most easily identified in most environments, and therefore, these colors may be the optimal choice for ureteral stents.
Conclusions
In this study, we demonstrated that the color of a stent plays an important role in endoscopic identification. Blue and green stents offered superior visibility in both clear and most hemorrhagic environments.
Footnotes
Disclosure Statement
No competing financial interests exist.