
Abstract
Background and Purpose:
Significant bleeding necessitating use of a tamponade balloon, embolization, or renal exploration is a rare but catastrophic complication after percutaneous nephrolithotomy (PCNL). The purpose of this study is to review the success of a novel, minimally invasive technique for controlling percutaneous tract bleeding that is refractory to conventional measures.
Materials and Methods:
A retrospective review was performed on four patients with refractory tract hemorrhage that was managed with a novel gelatin matrix hemostatic sandwich technique. In this technique, a 5F angiographic reentry catheter was placed through the kidney into the bladder and a 22F Councill-tip catheter balloon was passed over this catheter and positioned so that the inflated balloon would occlude the inner surface of the nephrostomy tract. Next, a 16F Councill-tip catheter was placed over a second wire so that the uninflated balloon was just underneath the skin surface. Gelatin matrix hemostatic sealant was then injected to fill the tract. Inflation of the outer balloon completely sealed the tract, completing the hemostatic sandwich.
Results:
This technique was successfully applied to four patients with tract bleeding that would not stop with pressure or a conventional nephrostomy tube alone. The average estimated blood loss was 562 mL, and three of four patients avoided transfusion. All postoperative hemoglobin values stabilized within 2 days of surgery. There were no major or minor complications after use of this technique. No patients needed angioembolization or renal exploration.
Conclusions:
This novel hemostatic sandwich technique should be considered as an option for the control of refractory tract hemorrhage after PCNL.
Introduction
Situations in which significant bleeding might occur may include segmental vessel injury, intercostal vessel injury, and renal fracture. The best method for hemorrhage control in these difficult situations is not known, but the ideal technique would reduce the need for open exploration, angioembolization, and the necessity for blood transfusion. Avoiding these complications would preserve renal function and avoid acute or permanent nephron loss.
Hemostatic agents that have been applied during PCNL in an attempt to decrease bleeding and thereby reduce morbidity include hemostatic gelatin matrix (FloSeal,® Baxter, Deerfield, IL), fibrin glue (Tisseel,® Baxter, Deerfield, IL), oxidized regenerated cellulose (Surgicel,® Ethicon, Somerville, NJ), and polyethylene glycol. 6 –10 At present, the application of these hemostatic agents is primarily in an adjunctive role and not as the primary hemostatic mechanism in the face of significant tract bleeding. 11
We developed a technique that includes the use of gelatin matrix hemostatic sealant (GMHS) sandwiched between two balloon catheters. The primary purpose of this study is to explain the methodology for this novel technique for controlling refractory percutaneous tract hemorrhage. As a secondary outcome, we review our initial results of the application of the hemostatic sandwich.
Patients and Methods
A retrospective case review was performed of PCNL procedures performed between February and November 2007. In four patients who underwent PCNL, tract bleeding was encountered at the end of the procedure, and the hemostatic sandwich technique was used to control tract bleeding.
The inclusion criteria for this study were intraoperative scenarios in which significant bleeding originated from segmental renal vessels, the percutaneous tract, or parenchymal injury and the bleeding did not stop with conventional pressure and nephrostomy tube placement. Each of these scenarios would have resulted in deployment of a Kaye tamponade balloon (Cook Medical Inc, Bloomington, IN) if the hemostatic sandwich had not been used. No other hemostatic technique was used in the other patients during this period. All cases were performed at a single institution by a single surgeon (DDB).
PCNL was performed with a 30F inner diameter nephrostomy tract sheath and in all cases used a rigid nephroscope with an ultrasonic lithotripter. Two standard 0.038 inch guidewires were placed routinely in each PCNL patient—one outside the sheath to act as a safety wire and one wire through the sheath that was used for balloon dilation and sheath placement. PCNL was completed either when all visible stone fragments were removed or when bleeding compromised visibility enough to necessitate termination of the procedure.
In each patient, a 5F angiographic reentry catheter was placed down the working guidewire into the bladder (Fig. 1a). Over the 5F angiographic catheter, a 22F Councill-tip catheter was placed into the renal collecting system. The catheter balloon was filled with 3 mL of sterile water and gently pulled against the kidney parenchyma to occlude the inner surface of the nephrostomy tract (Fig. 1b). This prevented blood from entering the renal collecting system and prevented urine from entering the percutaneous tract. In our experience, this maneuver, combined with external skin pressure applied by the surgeon's hand for 5 to 10 minutes would stop tract bleeding in nearly all patients with mild to moderate tract bleeding. If, however, brisk bleeding persisted after 10 minutes of pressure, these patients were selected for treatment with the hemostatic sandwich technique (Fig. 1).

(
Using the safety wire that was still in place in the tract, an additional 16F catheter was placed using direct visualization so that the catheter balloon was just beneath the skin (Fig. 1c). Next, the hemostatic gelatin matrix was injected into the tract by placing the injection tip between the 22F and 16F catheters (Fig. 1d). Five milliliters of GMHS was injected into the tract with subsequent inflation of the second 16F balloon with 2 to 3 mL of sterile water, completing the sandwich (Fig. 1e).
Postoperatively, patients were closely monitored with complete blood cell counts every 6 hours until the hemoglobin level stabilized. The outer balloon was deflated on postoperative day 1. In most patients, the nephrostomy tube was left in place several days to allow tract maturation before removal of the 22F catheter.
Preoperative demographics and stone parameters were evaluated in all patients who were treated with this technique. In addition, operative parameters and postoperative outcomes were reviewed in all patients who were treated with the hemostatic sandwich.
Results
Four of 57 total PCNL cases experienced significant tract bleeding during the study period. The hemostatic sandwich was successfully applied in all four of these patients, 2 men and 2 women. The mean patient age was 50 ± 13 years. Three patients had full staghorn calculi, and one patient had a partial staghorn. The mean estimated blood loss was 563 ± 350 mL (range 250 to 1000 mL). One patient had bleeding of 1000 mL intraoperatively from a parenchymal laceration. In the remaining patients, blood loss ranged from 250 to 700 mL. One of four patients needed a transfusion (2 units packed red blood cells) postoperatively. The mean drop in hemoglobin was 1.9 ± 1.8 g/dL (Table 1).
SD = standard deviation; ASA = American Society of Anesthesiologists; EBL = estimated blood loss; Hgb = hemoglobin.
The outer balloon was let down on postoperative day 1 in all patients. The 22F inner catheter was left in place to mature the tract in two patients, and the other two patients needed a second-look procedure on postoperative days 5 and 7, respectively. In these patients, the hemostatic sandwich did not compromise the second-look procedure, and no residual GMHS was noted in the renal collecting system or in the tract at the time of the second-look procedure.
When pressure and a nephrostomy tube failed to control tract bleeding, the deployment of the hemostatic sandwich resulted in immediate cessation of tract hemorrhage after PCNL in these four patients. No patient needed any additional procedures to control hemorrhage, such as angioembolization, use of a tamponade balloon, or open exploration. There were no complications observed because of use of the hemostatic sandwich or related to the GMHS migrating into the nephrostomy tract or causing ureteral colic. Creatinine levels for all patients stabilized by the time of hospital discharge (Table 2).
Discussion
PCNL is the procedure of choice for patients with large renal stone burdens, with stone-free rates of 74% to 83%. 2 PCNL is also used in patients with anatomic abnormalities, those resistant to other treatment modalities, and patients with lower pole calculi. 12 Despite improvements in surgical techniques, PCNL is accompanied by significant surgical risk. One of the most common complications of PCNL is the risk of hemorrhage necessitating transfusion, which occurs in 14% to 24% of patients. 2 Simple supportive care and transfusion will control most bleeding, but in 0.8% of cases, surgical intervention with angiographic embolization or open exploration will be needed. 3
When initial attempts at management of bleeding are unsuccessful, refractory tract bleeding presents a serious and challenging problem. The development of techniques that control bleeding and minimize blood loss from severe hemorrhage during PCNL can further increase the safety of this procedure. Currently, there are limited reports detailing strategies utilizing hemostatic agents to control refractory bleeding after PCNL. 13,14 The hemostatic sandwich technique effectively controlled significant hemorrhage after nephrostomy tract removal or parenchymal fracture in the cases presented, indicating that it is a viable option to consider under these circumstances.
The hemostatic sandwich technique has demonstrated the ability to minimize and control severe bleeding in PCNL. Only one patient needed transfusion, and this was likely because of a significant infundibular fracture with considerable blood loss during the procedure and before the hemostatic sandwich was applied.
The minimally invasive nature of this technique may make it the initial choice for refractory bleeding before consideration of more invasive procedures with their associated morbidity. Not only is the procedure less invasive, it also has the potential to preserve nephron function, which can be permanently or acutely lost with procedures such as angioembolization or nephrectomy.
Lastly, it can be performed at the time of surgery by the urologist and without the potential delay of waiting for assistance from an interventional radiologist.
Even when performing superselective angioembolization, up to 15% of the parenchyma of the involved kidney can become ischemic. 15 In this study, the median age was 54, with one of the four patients having hypertension and diabetes. Preservation of renal function in this population is important, because a glomerular filtration rate (GFR) < 60 is associated with a higher hospitalization rate, increased cardiovascular events, and higher risk of mortality. 16 In this group, the creatinine level remained stable (Table 2), and in all patients, the estimated GFR was >60 at the time of discharge.
The hemostatic sandwich uses both an inner and outer balloon catheter in combination with a hemostatic agent to stop bleeding. One hemostatic measure results purely from mechanical compressive forces. Hemostasis is created when bleeding fills the closed space between two occlusive balloon catheters and the subsequent rise in pressure results in tamponade. The tamponade pressure is augmented by the unique expansile property of the GMHS, which is reported to swell by as much as 20% after application. 6,10
The second mechanism of hemostasis is based on the activation of the clotting cascade. The GMHS works as an adjunct to the pressure tamponade by also causing cessation of bleeding by activating the final step of the clotting cascade. 17 In our experience, the combination of these two mechanisms led to the effective termination of both moderate and severe tract hemorrhage.
The use of hemostatic agents as adjuvant therapy to control bleeding after PCNL has been successfully reported in the urologic literature. 6, 8 –11,13,14,18 Gelatin matrix and fibrin glue are two hemostatic agents that have been successfully used to augment hemostasis after PCNL. 8,9,18 The primary goal of these agents is to improve hemostasis, yet each acts by a unique mechanism.
Fibrin glue is an adhesive compound formed from a combination of fibrinogen and thrombin. After heating to 37°C, the two ingredients are simultaneously ejected from the applicator in equal volumes. When the two solutions mix, thrombin converts fibrinogen to fibrin and initiates coagulation.
Gelatin matrix, however, consists of thrombin and bovine collagen granules averaging 500 to 600 μm cross-linked with gluteraldehyde. 10 It works by allowing the thrombin present in the sealant to activate the fibrin that is present in blood. This creates a clot when the gelatin matrix comes into contact with blood. 17
Early studies in vitro suggest that GMHS may be less likely to cause stone formation than fibrin glue because of the solubility properties of gelatin matrix. 6,8 Uribe and colleagues 8 studied solubility properties of four different hemostatics, including gelatin matrix and fibrin glue in human urine. Fibrin glue was found to initially form a clot and then transition to a semisolid mucoid substance. Gelatin matrix was immediately reduced to a fine suspension and remained soluble for the course of the experiment. 8
Using the porcine model, however, Kim and coworkers 7 showed that after injection of 2 mL of either FloSeal or Tisseel directly into the collecting system, obstruction occurred in 50% of the kidneys after 5 days. 7 Lee and associates 9 and Borin and colleagues 10 advocated for the use of an occlusion balloon on the inner surface of the tract as a “backstop” during PCNL to prevent unnecessary spillage of gelatin matrix into the collecting system.
The hemostatic sandwich technique takes advantage of both the reduced likelihood of clot formation using GMHS and the added safety of an occlusion balloon to prevent migration into the collecting system. In the two patients who were undergoing a second-look procedure after the GMHS sandwich, there was no GMHS noted in the collecting system (Fig. 2).
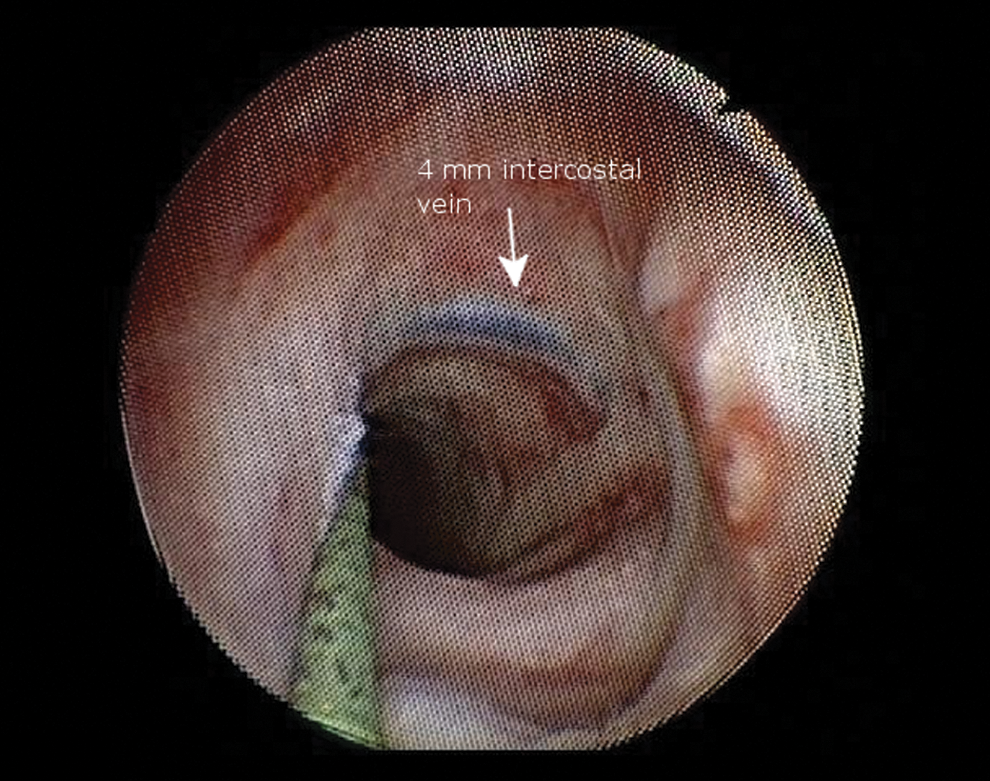
Appearance of the nephrostomy tract 5 days after application of the hemostatic sandwich. A large 4 mm intercostal vein is evident, which was the source of bleeding. No residual gelatin matrix hemostatic sealant was evident in the tract or collecting system.
In our practice, we have used the hemostatic sandwich technique to successfully control parenchymal fracture, small arterial, and small and large venous bleeding. Because of its relative cost, this procedure is recommended after PCNL only in patients with moderate or severe tract bleeding. A variation of the hemostatic sandwich technique without the use of GMHS may also be reasonable in circumstances in which bleeding is only modest. We have successfully used this technique without the gelatin matrix in two patients with moderate bleeding. It is unclear how effective the technique would be in the face of dramatic bleeding.
There are some limitations of this study. First, this is a retrospective study, and because there was no randomization performed, the natural history of tract bleeding in patients who did not undergo the hemostatic sandwich is unknown. It is possible that a longer period of conservative treatment might have also been accompanied by cessation of bleeding. Another limitation of this technique is the added cost of the additional catheter and the GMHS, which, in our institution, is $180. The hemostatic sandwich is only slightly more expensive than the Kaye tamponade balloon ($125) and is much easier to use and deploy. It is less costly than angiographic embolization ($4000) 19 or open exploration/nephrectomy ($4296). 20
Another possible concern with the use of GMHS is migration into the collecting system, which could cause ureteral obstruction or stones. This was not observed in any of the four patients, yet remains a potential concern despite balloon occlusion of the inner surface of the renal tract. In addition, GMHS seeping into the retroperitoneum is a possible concern, because this technique cannot directly prevent leakage from occurring. A larger experience will be necessary to determine whether migration of gelatin matrix into the retroperitoneum might potentially decrease the effectiveness of this technique.
Another potential concern with this technique is that the outer balloon could hide the evidence of bleeding, which might continue unrecognized into the perinephric space. Serial hemoglobin measurement and blood pressure monitering are essential in any patient with significant tract bleeding. Any patient who experiences continued instability should be considered for tamponade balloon placement or embolization. If leakage into the retroperitoneum did occur, however, no adverse effects were noted in the patients who were treated with the hemostatic sandwich technique in this series, and tamponade was not compromised in any patient.
Conclusion
In our experience, the hemostatic sandwich technique is safe and effective for controlling severe tract bleeding after PCNL. The procedure is easy to use and can be added easily onto a conventional nephrostomy tube if tract bleeding persisted after holding pressure for 10 minutes. The hemostatic sandwich also avoids the potential nephron loss that is associated with angiographic embolization. In this series, the use of a gelatin hemostatic sandwich between two catheter balloons successfully controlled bleeding without further need for angioembolization or open exploration. This technique should be considered in patients with persistent tract bleeding after PCNL.
Disclosure Statement
No competing financial interests exist.