
Abstract
Background and Purpose:
Creation of an optimally apposed, tension-free, well-supported vesicourethral anastomosis remains the cornerstone for anastomotic healing after radical prostatectomy. We report the effect of three techniques of bladder neck reconstruction during robot-assisted radical prostatectomy on anastomotic leak, stricture formation, and continence recovery.
Patients and Methods:
Between January 2005 to September 2009, 1900 consecutive patients underwent robotic-assisted laparoscopic prostatectomy (RALP) by a single surgeon. Of these, the first 214 underwent vesicourethral conventional anastomosis (CA); the next 303 men underwent anterior reconstruction (AR) only; and last 1383 men underwent total anatomic restoration (TR). Data elements included patient age, body mass index, preoperative biopsy Gleason score and prostate-specific antigen level, prostate volume, total operative time, console time, time for performing vesicourethral anastomosis, estimated blood loss, tumor stage, and margin status on final pathologic findings. Primary end points were rates of clinically significant anastomotic leaks, bladder neck contractures, and time to return of continence. Chi-square and Fisher exact tests were used for analysis of categoric variables. The Cox proportional hazard model was used for both univariate and multivariate analysis.
Results:
Clinically significant anastomotic leakage and bladder neck strictures were significantly fewer in the reconstructed groups (2.3% vs 1.0% vs 0.3% and 3.7% vs 1.3% vs 0.5% in the CA, AR, and TR groups, P < 0.01). Continence rates at 1, 6, 12, 26, and 52 weeks after RALP were also significantly better at all time points with AR and TR compared with CA alone (P < 0.001).
Conclusions:
TR of the continence mechanism optimizes vesicourethral anastomosis healing and hastens early continence return after RALP.
Introduction
Recent technical innovations in fashioning the vesicourethral anastomosis have been reported to deliver earlier continence return and lower incidence of BNCs. 1 In our center, our technique for vesicourethral anastomosis construction during robot-assisted lasparoscopic prostatectomy (RALP) has evolved in three stages over the past 5 years. 2,3 We report our experience with urinary leaks, BNCs, and continence return in a cohort of 1900 patients who were receiving one of these three techniques during RALP and evaluate risk factors for development of these anastomotic complications.
Patients and Methods
Patient cohort
Between January 2005 to September 2009, 1900 consecutive patients underwent RALP by a single surgeon (AT). The first 214 men received conventional anastomosis (CA), the next 303 men received anterior reconstruction (AR) of the bladder neck, and last 1383 men received the total anatomic restoration (TR) technique.
Surgical techniques used
CA
After urethral transection, the vesicourethral anastomosis was fashioned with a continuous running technique that used two 3-0 poliglecaprone monofilament sutures on an RB-1 needle (Ethicon Inc, Somerville, NJ) whose tails had been tied together extracorporeally. Using a 0-degree lens and Endowrist® needle drivers on both sides, the dyed suture is passed in a clockwise hemicircumferential manner, starting from outside in on the bladder neck at the 5 o'clock position and inside out on the urethra up toward the 12 o'clock position. The undyed suture is similarly run in a counterclockwise hemicircumferential direction. The running sutures are snug down after each apposition to ensure there is no slack, and finally tied together with several knots at the 12 o'clock position.
AR of the bladder neck
The following steps were further incorporated for AR of the bladder neck 2 : (1) Minimal distal incision of the endopelvic fascia; (2) preservation of the arcus tendineus; (3) dissection and subsequent preservation of the puboprostatic ligaments during dorsal venous control; (4) reattachment of the arcus tendineus and puboprostatic ligaments to the anterolateral distal bladder.
TR technique
Further appreciation of points of biomechanical instability around the vesicourethral anastomosis led us to hypothesize that (1) the posterior bladder neck lies unsupported in the empty retrotrigonal fossa formed after seminal vesicle excision; (2) the Ω-shaped remnant urethral rhabdosphincter is deficient posteriorly; and (3) caudal recession of the urethral stump places tension on the anastomosis. 4 We then incorporated the principles of posterior bladder neck reinforcement 5 and the Rocco technique of posterior reconstruction of the Denonvilliers musculofascial plate (PRDMP) 6,7 to our anterior reconstruction technique to arrive at our current technique of total anatomic restoration (Figs. 1A, 1B).
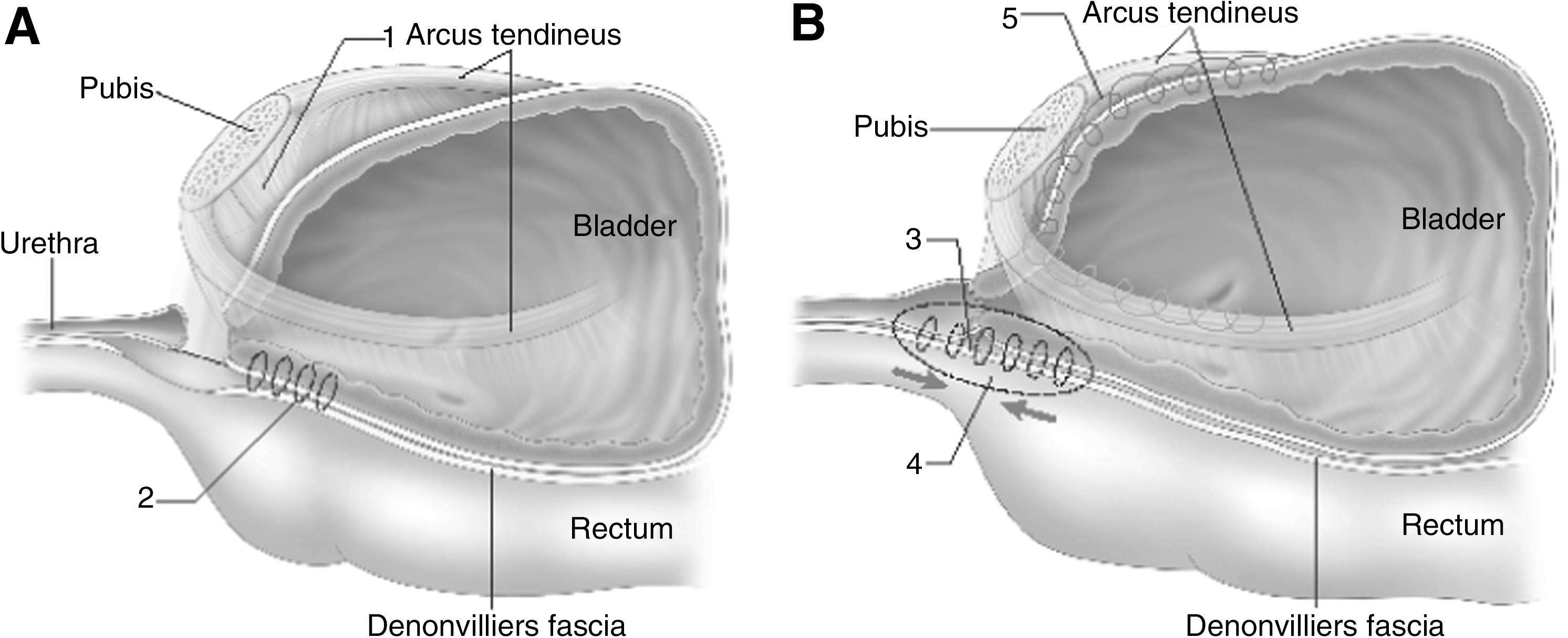
Anatomic restoration of vesicourethral junction.
Managed care and follow-up protocol
After bladder neck reconstruction, integrity of the anastomosis was routinely checked with bladder distention using 150 mL of physiologic saline to confirm that there was no visible leakage. Pelvic placement of a Jackson-Pratt drain was then removed on postoperative day 1 unless output exceeded 150 mL over a 24-hour period. All patients were routinely discharged from the hospital on postoperative day 1 receiving oral analgesics; they returned on postoperative day 7 for catheter removal.
Outcomes measurement
Under a protocol reviewed and approved by the Institutional Review Board, patients were followed and their outcomes data collected at regular intervals. During their clinical office evaluation before surgery, patients were asked to provide demographic information and to complete self-administered versions of standardized health-related quality-of-life (HRQOL) measures, including the Expanded Prostate Cancer Index Composite (EPIC) 22 and International Prostate Symptom Score (IPSS). In addition, pre-urgical clinical data such as prostate-specific antigen (PSA) level, clinical stage, and biopsy Gleason score were abstracted from medical records. Outcomes questionnaires containing items from the urinary function section of the EPIC HRQOL were dispatched to patients via postal or electronic mail at 1, 6, 12, 26, and 52 weeks after surgery. Patients were also contacted via telephone by a member of the research team (DP, AS, SG, YE) at each of the above follow-up intervals to ensure receipt of the questionnaire.
Data collection and follow-up correspondence were performed in compliance with the Health Insurance Portability and Accountability Act. A follow-up rate of 90% was achieved in all three groups. The returned responses to the outcomes questionnaires, along with the patients' preoperative, operative, and postoperative clinicopathologic data, were prospectively entered into a password-protected Microsoft® 2007 Access database (Microsoft Corp, Redmond, WA).
Continence recovery was defined as the use of zero pads or one security liner/24 hours. Perioperative complications were identified from patients' electronic records and minutes of department mortality and morbidity meetings. Anastomotic leaks that were diagnosed on cystography were graded as mild, moderate, and clinically significant. Mild and moderate leaks were defined as those limited to the extraperitoneal space managed conservatively with prolonged catheterization until spontaneous resolution was confirmed on repeated cystography. Clinically significant leaks were (1) those that extended intraperitoneally; (2) those that necessitated interventional drainage; (3) those that resulted in ileus necessitating readmission and intravenous fluids; and (4) those that were associated with fever and signs of sepsis necessitating antibiotic therapy or drainage. Postoperative bladder neck contractures were identified from patients' electronic records using the International Classification of Diseases-9 codes for urethral stricture and related interventions: eg, internal urethrotomy, urethral dilation, and transurethral bladder neck incision. Primary end points for our analysis were time to return of continence, clinically significant anastomotic leaks, and postoperative bladder neck strictures.
Statistical analysis
Statistical analysis was performed using PASW v18.0 (SPSS Inc, Chicago, IL) and Intercooled Stata 9.1 (Stata, College Station, TX); P values of <0.05 were considered significant. Comparison of continence return between the reconstruction groups was performed with a chi-square test. The Cox proportional hazard model was used for both univariate and multivariate analysis. Preoperative PSA levels and prostate volume were transformed using the natural log for both univariate and multivariate analysis to account for skewed distribution. In the univariate model, each variable was correlated with time to return to continence independently. Variables significant in univariate analysis were then included in the multivariate model, and relative risk and 95% confidence intervals reported for each significant variable. Results from the multivariate analysis were then used to generate one-minus survival curves stratified by reconstruction method.
Results
Patient demographics
Between January 2005 to September 2009, 1900 men underwent RALP, receiving either CA, AR, or TR. Clinical and pathologic demographics of the study cohort are listed in Table 1. The mean age of patients in these groups was 59.8 ± 6.6 years, 59.8 ± 7.3 years, and 60.3 ± 7.4 years in the CA, AR, and TR groups, respectively. Age, prostate volume, preoperative PSA level, and IPSS were similar in the three groups (Table 1). With regard to intraoperative parameters, estimated blood loss, operative time, and console time: These were not statistically significant between the three groups (Table 2).
BMI = body mass index; IQR = interquartile range; PSA = prostate-specific antigen; preop = preoperative; IPSS = International Prostate Symptom Score; SM = surgical margin.
IQR = interquartile range; NS = not significant.
Anastomotic complications
Clinically significant urinary leakage developed in 12 patients. The incidence of clinically significant anastomotic leaks was 2.3%, 1.0%, and 0.3% in the CA, AR, and TR groups, respectively (P = 0.01), with no patient in the TR cohort needing interventional drainage. The rate of bladder neck stricture was 3.7%, 1.3%, and 0.5% in patients receiving CA, AR, and TR, respectively (P < 0.001) (Table 3). On univariate analysis, bladder neck reconstruction technique was the only significant variable for development of anastomotic leakage (P = 0.01).
Recovery of continence after RALP
Recovery of continence at 1, 6, 12, 26, and 52 weeks with each reconstruction technique is represented in Table 4 (Fig. 2). The mean time to return of continence was 19.0, 7.3, and 5.7 weeks in the CA, AR, and TR cohorts, respectively (P < 0.001). The chi-square test and one-way analysis of variance validated statistically significant improvement in continence return with TR compared with the other two techniques of bladder neck reconstruction at each follow-up interval. Lower age, smaller volume, absence of capsular invasion, and anterior and total reconstruction techniques were significant predictors for early continence on univariate analysis. Incorporating these significant variables into a multivariate model, age and reconstruction method were the only significant factors for early continence. Holding all other variables constant, TR was the most significant variable for early continence (Table 5).
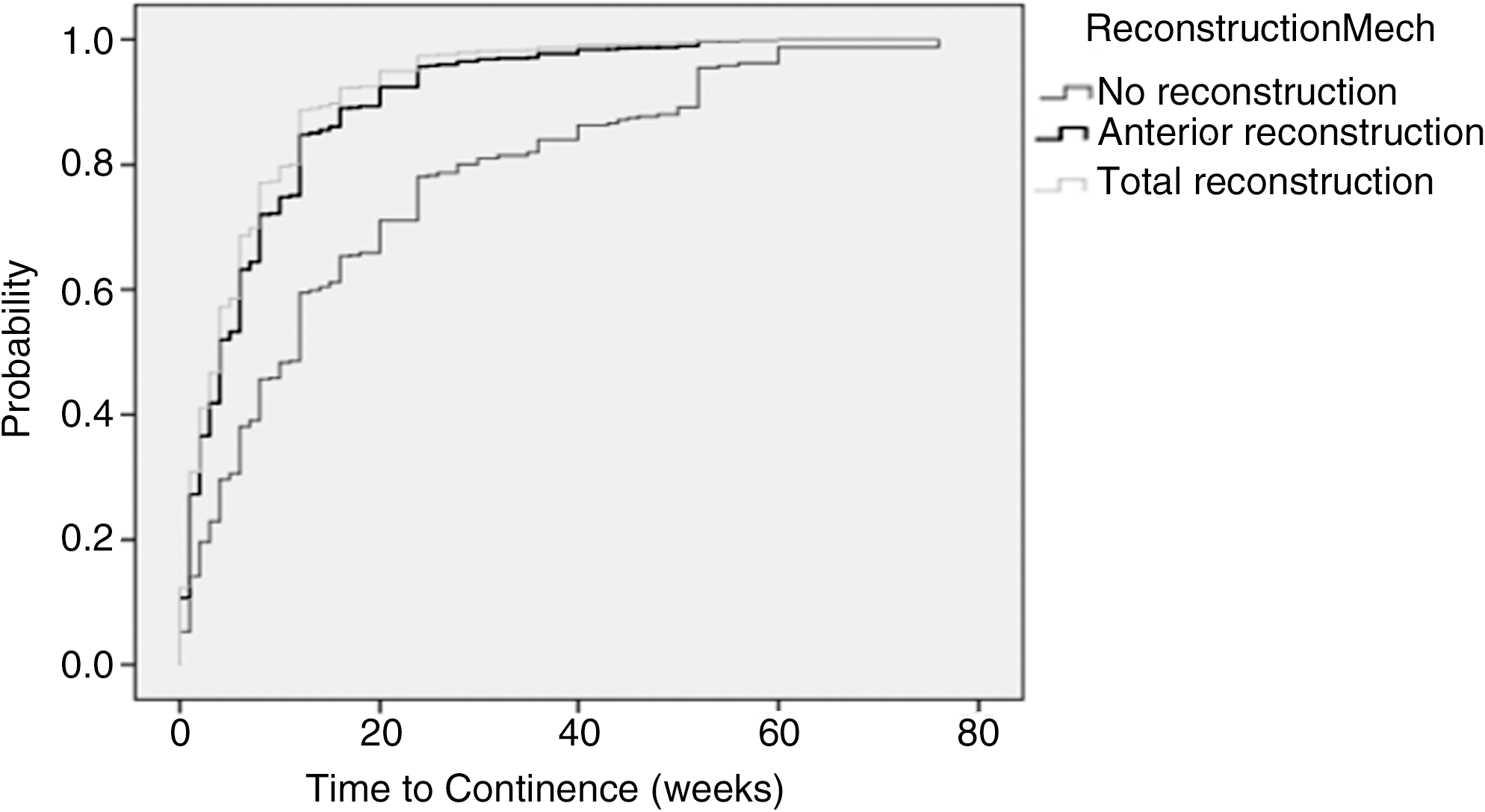
Cumulative probability of return of continence by reconstruction technique.
Significant at the 0.05 level (two-tailed).
Significant at the 0.01 level (two-tailed).
Relative risk compared with no reconstruction group as reference.
RR = relative risk; PSA = prostate-specific antigen.
Discussion
Over the last decade, novel techniques for reconstructing the bladder neck have contributed to improved continence return and a lower incidence of anastomotic leaks and BNCs in recent series of open, laparoscopic, and robot-assisted radical prostatectomies (Table 6). In 2000, Hoznek and associates 8 described their experience using two hemicircumferential running sutures during laparoscopic radical prostatectomy (LRP) with no reported BNCs. van Velthoven and colleagues 9 reported a continuous running single-knot suture technique for fashioning the vesicourethral anastomosis during LRP, using two 3-0 polyglycolic acid sutures whose tails had been tied extracorporeally. This simplified approach of anastomosis construction was rapidly adopted by other laparoscopic surgeons, and popularized by Menon and coworkers 10 from the Vattikuti Urology Institute in Detroit for robot-assisted radical prostatectomy.
BNC = bladder neck contracture.
More recently, Rocco and colleagues 6,7 have advocated PRDMP. Disruption during radical prostatectomy results in loss of the posterior insertion of the urethral rhabdosphincter, overall pelvic descent of the sphincteric complex, and perineal prolapse. PRDMP attempts to reconstruct the musculofascial plate by connecting the posterior median raphe of the dorsal wall of the rhabdosphincter to the remnant Denonvilliers fascia and suspending it to the posterior bladder wall 1 to 2 cm posterosuperior to the vesicourethral junction.
We postulate that during CA after radical prostatectomy, the vesicourethral anastomosis and bladder neck become unstable at the following sites (Fig.3): (1) Tension is exerted on the healing anastomosis from spontaneous urethral stump recession into the pelvic floor; (2) the posteriorly deficient Ω-shaped urethral rhabdosphincter lies unsupported posteriorly, impairing efficient contraction of the sphincter mechanism; (3) the posterior bladder neck lies unsupported in the retrotrigonal fossa created by excision of the seminal veiscles; and (4) the anterior and lateral bladder neck lie unsupported as well. The overall effect appears to be pelvic descent of the bladder pressing on the unsupported anastomosis, and stress on the continence mechanism during micturition.
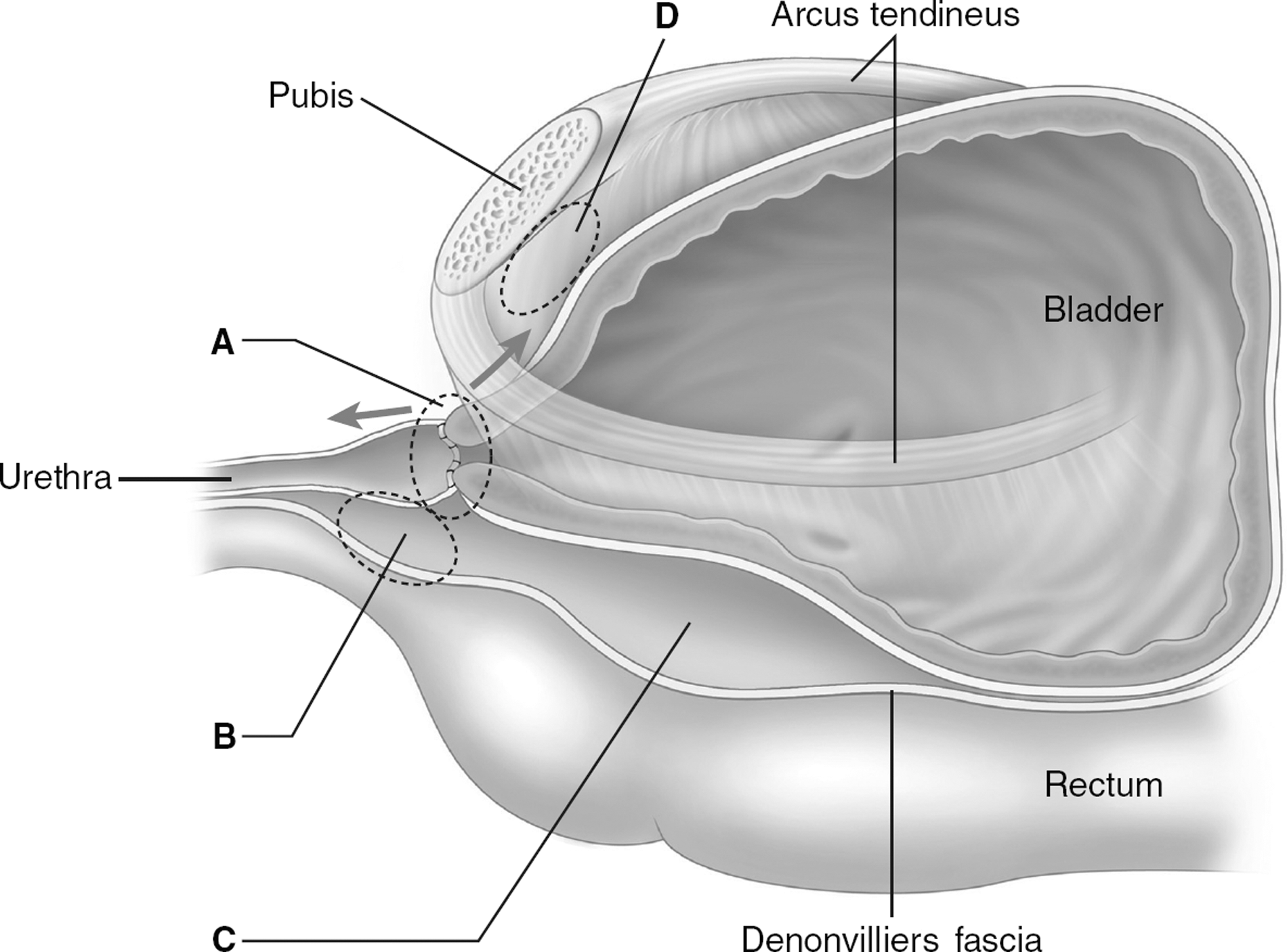
Points of postulated biomechanical instability associated with the conventional vesicourethral anastomosis (sagittal view): A. Tension on the vesicourethral anastomosis from spontaneous urethral stump recession into the pelvic floor; B. the posteriorly deficient Ω-shaped urethral rhabdosphincter lies unsupported posteriorly, impairing efficient contraction of the sphincter mechanism; C. the posterior bladder neck lies unsupported in the retrotrigonal fossa created by excision of the seminal vesicles; D. the anterior and lateral bladder neck lie unsupported as well. Reproduced with permission from Tan GY et al. Urology 2009. 4
To redress these points of instability, we first adopted AR of the bladder neck, and subsequently incorporated a modified technique of posterior bladder neck plication and reconstruction of the Denonvilliers musculofascial plate for circumferential dynamic suspensory support for the urethral sphincter complex. Postoperative cystography and endorectal MRI (Fig. 4) in several of our patients demonstrated suspension of the anastomosis and urethral rhabdosphincter well above the pelvic floor with all-round tissue bolstering.
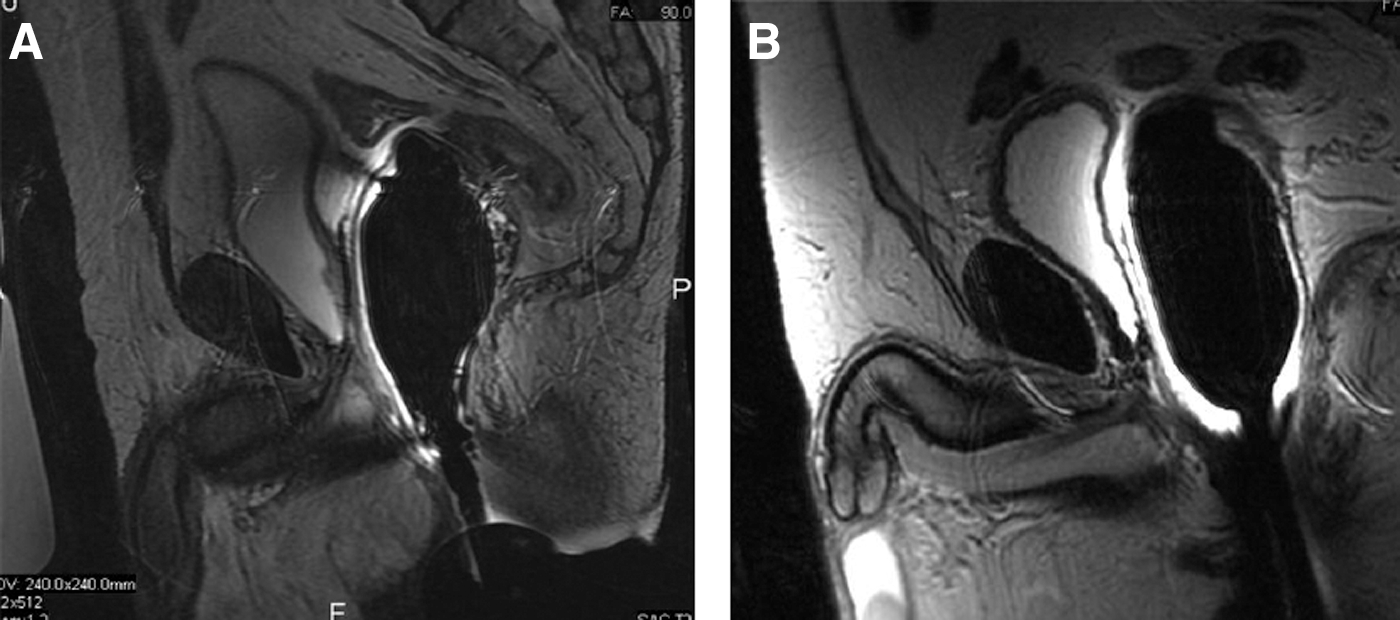
Postoperative endorectal magnetic resonance imaging (sagittal views) of the vesicourethral anastomosis in two patients who underwent total anatomic restoration technique
In our series, surgical technique was the most significant predictor for clinically significant urinary leaks (Table 5), with the incidence falling from 2.3% to 1.0% to 0.3% with CA, AR, and TR, respectively. The incidence of BNCs also significantly decreased from 3.7% to 1.3% to 0.5%, respectively (P < 0.01) with these three techniques of bladder neck reconstruction. These results compare favorably with BNC rates in the published literature that report stricture rates up to 32%. 11 –14 While the mechanisms for stricture formation remain incompletely understood, recognized risk factors include surgical technique, narrowing of the bladder neck, urinary leakage, prolonged operative time, excessive blood loss, and hematoma formation. 15,16
Patil and coworkers 17 reported development of clinically significant anastomotic leaks necessitating interventional drainage or management of ileus in 12 of 3327 (0.36%) patients, and development of BNCs necessitating secondary intervention in 37 (1.11%) patients. BNCs were more likely to develop in patients with larger anastomotic leaks, probably from prolonged inflammation at the anastomosis as well as persistent uremia and mass effect of the urinoma impairing tissue healing. In addition, TR also significantly accelerates continence recovery after RALP, reducing the mean time to pad-free continence from 19.0 weeks with CA to 5.7 weeks (Table 4).
Our results suggest that biomechanical stability with circumferential support and relief of tension at the anastomosis optimizes local conditions for tissue healing and continence return. Nonetheless, we recognize the following limitations of our study: First, it is a retrospective review of a single experienced surgeon's (AT) experience with three techniques and raises issues about reproducibility of results in less experienced hands. The effect of the learning curve is probably not a large one given the lead surgeon's extensive experience with RALP at his previous institution. Second, postoperative cystography was not performed routinely before Foley catheter removal, but only on clinical suspicions of patients with postoperative ileus, discomfort, or fever. The number of patients who ultimately underwent cystography was 70, 100, and 350 in CA, AR, and TR groups, respectively. As such, the overall leak rate may be higher. Routine cystography, however, has not been found to be a cost-effective practice, 18 with Guru and coworkers 19 reporting average costs of $1200 per cystogram at their institution.
Third, our study was not randomized. Menon and associates 20 recently published their experience comparing a double-layer vs single-layer anastomosis during robot-assisted radical prostatectomy in a randomized fashion. In their cohort of 116 patients, they found no significant difference in time to continence return between the two groups. A randomized multi-institutional study is undoubtedly the best way forward in validating the reproducible efficacy of our TR technique on anastomotic healing and continence outcomes.
Conclusion
Potential areas of biomechanical instability associated with vesicourethral CA construction during radical prostatectomy may be corrected with AR. This technique, targeted at optimizing mucosal coaptation and suspensory support for the urethral rhabdosphincter while minimizing tension on the anastomosis, significantly accelerates return of continence and improves anastomotic healing.
Footnotes
Disclosure Statement
Dr. Gerald Tan receives financial support from the Ferdinand C. Valentine Fellowship in Urologic Research, New York Academy of Medicine, and the John Steyn Traveling Fellowship in Urology from the Royal College of Surgeons of Edinburgh.
Dr. Alexis Te is an investigator and consultant for Sanofi-Aventis, Inc; an investigator for Pfizer, Inc; and an investigator for American Medical Systems, Inc.
Dr. Ashutosh Tewari has received research grants from Intuitive Surgical and the Prostate Cancer Foundation; he is also the endowed Ronald P. Lynch Professor of Urologic Oncology and Director of the Lefrak Institute of Robotic Surgery, Weill Cornell Medical College.