
Abstract
Purpose:
To describe the current and new developments in transrectal ultrasound (US) imaging of the prostate.
Patients and Methods:
Grayscale imaging of the prostate is the standard method for diagnostic evaluation and biopsy guidance. Color Doppler (CD) imaging, including CD and power Doppler US, allows for detection of macrovascularity and may therefore be helpful for assessment of prostatic blood flow. The use of US microbubbles for CD imaging and new contrast-specific techniques enable assessment of prostate microvascularity associated with prostate cancer (PCa). Recently, real-time elastography has been introduced to improve detection of cancer based upon changes in tissue stiffness.
Results:
Contrast-enhanced CD imaging has shown to enable PCa detection by performing targeted biopsies into suspicious areas. Comparisons between systematic and contrast-enhanced targeted biopsies have shown that the targeted approach detects more cancers and cancers with higher Gleason scores with a reduced number of biopsy cores. New microbubble-specific US techniques can improve sensitivity and specificity of US imaging for PCa detection. Real-time elastography has been demonstrated to be useful for the detection of PCa, and may further improve PCa staging.
Conclusions:
The new US techniques seem to have the potential to improve PCa detection, and also PCa grading and staging. As these diagnostic methods improve, the ultimate hope is to eliminate biopsy in patients without cancer.
Introduction
TRUS-guided, laterally directed 18-gauge core biopsy has become the standard way to obtain material for histopathological examination. The number of biopsies required for the optimal detection of PCa is controversial. Nearly all studies have shown a higher cancer detection rate with a greater number of biopsies in comparison with the standard sextant technique. 3 Currently, at least 10 biopsy cores or the use of the Vienna nomograms are recommended for routine use. The transition zone should not be the target area for a first set of prostate biopsies because of a consistently low cancer detection rate of ≤2%. If the first set of biopsies is negative, repeated biopsies can be recommended. In the second set of biopsies, a detection rate of about 10% to 35% has been reported in cases with a negative first set of biopsies. 2
The positive predictive value (PPV) of biopsies based on DRE, PSA, and TRUS is low and many unnecessary biopsies are performed. However, even in patients with low PSA values a significant number of PCa cases are found. Detection and localization of PCa using grayscale US is poor. TRUS is mainly used to guide systematic biopsies (SB) and can be safely omitted as a screening tool. Therefore, the search for improvement of diagnostic techniques is a necessity. 4
Several different approaches to improve detection are studied. Novel tumor markers have been researched, but showed so far to be inaccurate to replace PSA. 5 Improvement of PCa observation would lead to targeted biopsies, right in the center of the tumor. This probably would lead to a change in biopsy strategies with better grading and improved staging. The treatment could be improved, if the exact location and volume of the tumor is known. Also, the follow-up could be optimized if imaging could localize recurrence of malignant tissue. 6
On the basis of the above-mentioned, new imaging techniques are desirable to improve PCa diagnosis. In this article we will focus on the value of contrast-enhanced US (CEUS) and elastography.
Conventional US
TRUS had its clinical introduction in the year 1974. 7 Since then this classical urological imaging modality has been steadily improved. Undoubted is the use of the TRUS to assess the prostate size and to guide the prostate biopsy. The early and safe detection of PCa as well as the determination of local extension is a great clinical challenge for the TRUS.
With the B-mode TRUS the prostate can be good delineated from the surrounding tissues such as rectum, neurovascular bundles, or fat. Also the zonal anatomy described by McNeal can be good distinguished. Asymmetry of the prostate, seminal vesicles, and hypoechogenic patterns are believed to be associated with malignancy. The classic grayscale US description for PCa is a hypoechoic lesion, but PCa may also appear echogenic or isoechoic. About half of PCa lesions are invisible by grayscale US. The sensitivity of the B-mode TRUS for the detection of PCa ranges from 44% to 90% and the specificity from 30% to 74%. Also, prostatitis and benign prostatic hyperplasia mimic the grayscale appearance of PCa. Therefore, conventional prostate US has little advantage over DRE for detecting PCa. 8
Doppler US Techniques
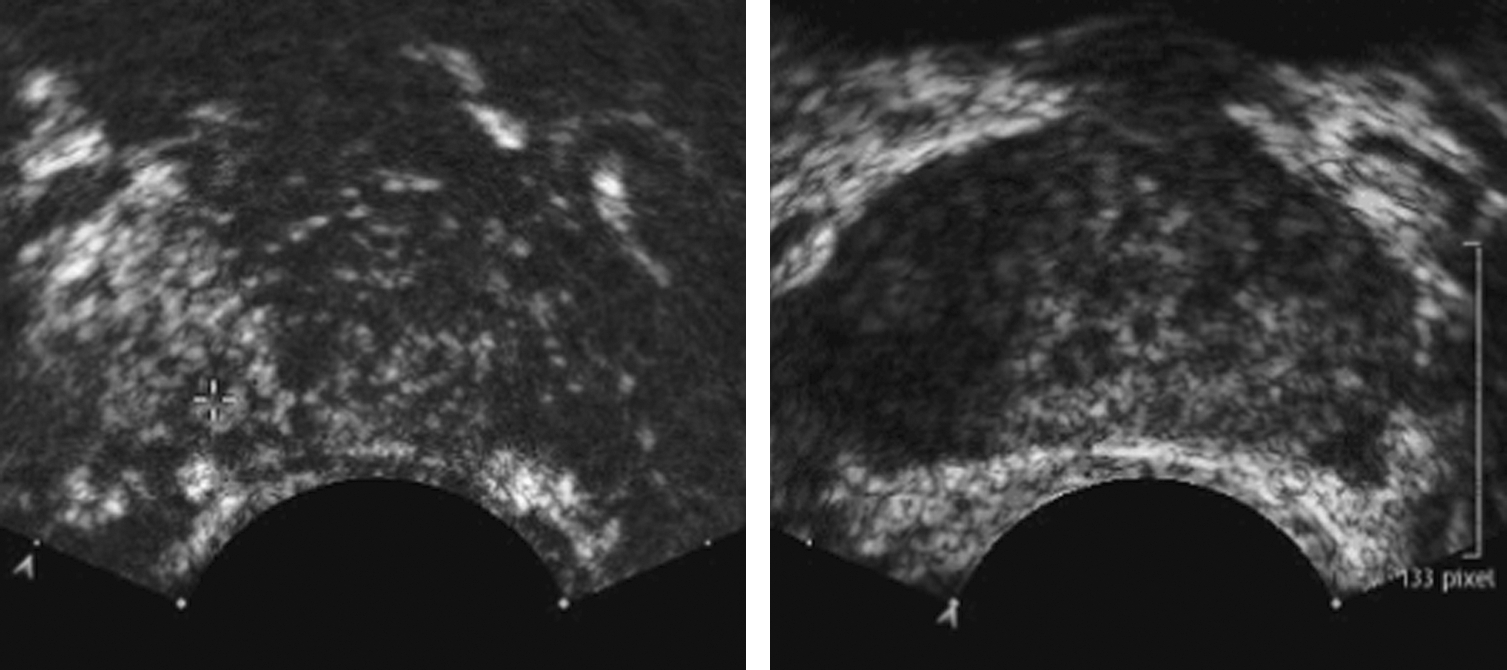
Doppler US techniques demonstrate the presence of blood flow by detecting a frequency/phase shift in the US radiofrequency signal reflected from moving blood. PCa is associated with increased perfusion; therefore, the sensitivity of US for detection of PCa may be increased with color Doppler (CD) imaging of blood flow within the prostate. The CD signal correlates positively with both stage and grade of a prostate tumor and also with the risk of recurrence after treatment. Rifkin et al 9 have categorized pathological flow patterns (increased flow rate within the lesion, increased flow rate around the lesion, and asymmetric flow compared with surrounding normal tissue). Power Doppler (PD) reflects the amplitude of the Doppler signal and does not demonstrate directionality of flow. PD is more sensitive to small amounts of low-velocity flow. Several small studies have suggested that PD may be even more useful than CD in detecting PCa. However, the sensitivity of grayscale and Doppler US-guided targeted biopsy is not sufficient to eliminate the need for SB, 10 though conventional US is mainly used to guide SB and volume determination of the prostate only (Fig. 1).

Transverse grayscale ultrasound image of the prostate. The hypoechoic area on the right side demonstrates benign prostatic tissue on biopsy.
Contrast-Enhanced US
It is known that tumor growth induces neovascularization. Further, an increased microvessel density is associated with the prognosis and progression of PCa. Therefore, observation of the induced altered perfusion patterns may improve PCa detection. 11
CEUS imaging was developed to image perfusion. Because of the high spatial and temporal resolution of US, detailed and real-time perfusion imaging became possible. US contrast agents consist of small encapsulated gas bubbles that are administered intravenously and remain intravascular. Adding microbubbles as additional reflectors into the bloodstream increases the sensitivity of CD and PD imaging. These techniques use relatively high US energy levels; therefore, a large proportion of the microbubbles are destroyed as they are imaged. New imaging techniques have been developed that enable sensitive microbubble imaging even in the microvasculature. A long list of CEUS techniques is now available: harmonic imaging (using the nonlinear behavior of microbubbles in an US beam), pulse inversion techniques (using various pulses to isolate the nonlinear reflections), or even more specific imaging techniques that provide selective imaging of the signals reflected by the bubbles, canceling out most of the tissue reflections. 6
Sedelaar and colleagues 12 had already concluded in 2001 that transrectal three-dimensional PD (3D-PD) CEUS has the potential to observe lesions with an increased microvessel density. Discrimination between left- and right-localized tumors could be accurately performed in 78%. Goossen and co-workers 13 evaluated a large patient group with 3D-PD CEUS before radical prostatectomy (RP), and 68% to 79% of all tumor foci larger than 5 mm were detected. Unal et al 14 concluded that 3D-PD CEUS was the best single diagnostic tool for the detection of PCa in a study including men with and without cancer. In a small series using microvascular imaging, all T3 tumors could be observed. These results are promising, but the clinical value should be tested in a diagnostic setting. Studies with the latest contrast-specific imaging techniques have been performed, showing an increased sensitivity for the detection of perfusion patterns, but are not yet published as an article. 6
Frauscher and colleagues 15 compared CD-CEUS targeted biopsy (CB) of the prostate with grayscale-US-guided SB. Two hundred and thirty male screening volunteers were included. The detection rate was 30%, including 56 (24%) by CB and 52 (23%) by SB. Cancer was detected by CB alone in 17 patients (7%) and by SB alone in 13 (6%). The detection rate for CB cores (10%) was significantly better than that for SB cores (5%). CB in a patient with cancer was 2.6-fold more likely to detect PCa than SB, and CB detected as many cancers as SB with fewer than half the number of biopsy cores.
Pelzer and associates 16 thereafter investigated the impact of a combined approach of CB and SB on the PCa detection rate in men with PSA 4 to 10 ng/mL. They examined 380 screening volunteers and found that cancer was detected in 38%. The cancer detection rate for CB and for SB was 27% and 28%, respectively. The cancer detection rate with the two methods combined was 38%. For targeted biopsy cores, the detection rate was significantly better than for SB cores (33% vs. 18%). CB in a patient with cancer was 3.1-fold more likely to detect cancer than SB. Only the combined use of CB and SB allows for maximal cancer detection with a detection rate of 38%.
Further, Mitterberger and associates 17 evaluated SB versus CB for the impact on Gleason score findings. The study included 690 men. PCa was identified in 221 of 690 subjects (32%) with a mean PSA of 4.6 ng/mL. PCa was detected in 180 subjects (26%) with CB, and in 166 patients (24%) with SB. The Gleason score of all 180 cancers detected by CB targeted biopsy was 6 or higher (mean 6.8). The Gleason score of all 166 cancers detected by SB ranged between 4 and 6 (mean 5.4). CB detected significantly higher Gleason scores compared with SB. Further CB techniques may allow identification of more aggressive cancers, which is important for defining prognosis and deciding treatment.
Also, the effect of premedication of Dutasteride, a dual 5-alpha-reductase inhibitor, on prostatic blood flow prior prostate biopsy and the impact on PCa detection was assessed. 18 Thirty-six patients with elevated PSA (≥1.25 ng/mL) were treated with Dutasteride 14 days before prostate biopsy. CD-CEUS was performed before, 7 days after, and 14 days after treatment. Dutasteride has shown to reduce prostatic blood flow in benign prostatic tissue, whereas in PCa areas blood flow is still observed after a 14 days course. Twelve patients (33%) were found to have suspicious blood flow and PCa, and six cancers (17%) were detected solely by targeted contrast-enhanced biopsy.
In a recent prospective trial comparing contrast-enhanced targeted versus systematic US-guided biopsies for PCa detection, the previous findings were confirmed. The chance to find cancer in a targeted biopsy core was significantly higher than in a random biopsy core. Moreover, the total detection rate for 5 targeted biopsies alone was higher than for 10 random biopsies. 19
CEUS was also used to investigate the follow-up of medical and minimally invasive treatment modalities that influence the prostate perfusion. In 2002 CEUS monitoring of hormonal treatment was described. Thirty-six men with PCa were studied at baseline and at intervals during treatment using CEUS imaging. Quantitative analysis demonstrated a decrease in CEUS signal over time and a strong correlation with changes in the mean PSA was found. 20 Already in 2000 Sedelaar and co-workers 21 showed that 3D-CE-power Doppler ultrasound (PDU) can determine the size of the defect of high-intensity focused ultrasound (HIFU) ablative therapy for PCa. The absence of blood flow reflected affected tissue after HIFU treatment.
Recently, Wink et al 6 reported about CEUS and PCa detection from a European multicenter research coordination project. The pooled analysis provided valuable safety, operator dependence, and time/cost data derived from a remarkable number (more than 3000 biopsies) of CEUS studies. These studies showed that PCa could be observed and localized in up to 78%. Observation of the tumor enabled better detection. Further, targeted biopsies lead to fewer biopsies per session without loss of detection rate. A combined approach offered the highest detection rate. However, the authors conceded that they have not yet met their stated goal of bringing CEUS into routine practice. Although the ultimate utility of CEUS in routine practice remains unknown, this project may serve as a model of multi-institutional collaboration to advance prostate imaging.
In a recent study we evaluated CEUS using cadence-contrast pulse sequencing (CPS) technology for PCa detection. Forty-four men with suspicious PSA levels and CPS findings were assessed; all had CPS targeted and SB. Transrectal CPS images were taken with a low mechanical index (0.14). A microbubble contrast agent (SonoVue; Bracco International BV, Amsterdam, The Netherlands) was administered as a bolus, with a maximum dose of 2.4 mL. CPS was used to assess prostatic vascularity. Areas with a rapid and increased contrast enhancement within the peripheral zone were defined as suspicious for PCa and targeted biopsies were taken. Subsequently, a 10-core SB was taken. Cancer was detected in 35 of 44 patients (80%). Lesions suspicious on CPS showed cancer in 35 of 44 patients (80%), and SB detected cancer in 15 of 44 patients (34%). CPS targeted cores were positive in 105 of 220 cores (47.7%) and in 41 of 440 SB cores (9.3%) (p < 0.001). Lesions suspicious on CPS were false-positive in 9 of 44 patients (20%), but CPS enables excellent observation of the microvasculature associated with PCa, and can improve the detection of PCa compared with SB.
In conclusion, CEUS enables observation of PCa. Sensitivity and specificity are still not high enough to be able to avoid systematic random biopsies. Targeted biopsies added to a random protocol increase the PCa detection rate. The ability of CEUS to observe perfusion in an organ that has limited blood flow enables observation of various medical and minimally invasive treatment effects.
Increasing PPV and decreasing false-positives are interesting, but this is not the main target, because of the high percentage of overdiagnosis and subsequent overtreatment. Patients do not want to know if they have an insignificant cancer; they only profit of a diagnosis of cancer, if the tumor is relevant concerning stage and grade. It seems that for detecting relevant PCa further technical developments will be necessary.
Further, patients are interested in a lower number of biopsies including less morbidity, but without the risk, that relevant cancers are missed. CEUS allows to detect PCa much more likely than SB. However, also on this topic further studies are necessary. The ultimate goal will be with imaging to refrain patients from prostate biopsy.
Until now CEUS is an addition to the existing modalities for imaging, diagnosis, and follow-up of PCa, but still needs further investigation (Fig. 2).
Dual transverse view of prostate imaged by cadence contrast-pulse sequence ultrasound technique (Siemens Medical Solutions, Mountain View, CA). Increased enhancement of the right side was suspicious for malignancy. Prostate cancer was proved by biopsy.
New microbubble-specific techniques including CPS or microvessel imaging may increase significantly the PCa detection. Limitations include the limited availability of high-end US systems in urological departments, current inadequate training, and, of course, associated higher costs.
Elastography
US-based real-time elastography imaging is a new technique that observes the differences in tissue strain produced by freehand compression. 11,22 Using elastography, the investigator is able to discriminate hard from soft tissue regions within the prostate. The phenomenon is based on the fact that the back-scattered US signals undergo displacement if the tissue is slightly compressed or decompressed. Stiffer tissues show less displacement than normal soft tissues. For observation, stiffness values are marked in different colors and are shown in real-time images. Following the hypothesis that solid tumors differ in their consistency compared with the adjacent normal tissue, elastography has been investigated as a novel tool for detecting PCa. Promising results have been recently reported in small cohorts. 23,24
Cochlin et al 25 introduced real-time elastography for the detection of PCa in biopsy specimens. In their study elastography had a sensitivity of 51% and a specificity of 83% for the detection of PCa in individual patients, and a sensitivity of 31% and a specificity of 82% for the detection of individually biopsied areas of the prostate. Sperandeo and associates 26 in 2003 reported the usefulness of elasticity imaging to differentiate malignant from benign lesions. In their study they used tissue elasticity to detect cancer based on tissue deformation of grayscale images under manual compression of the prostate with a transrectal probe.
Also, Konig et al 27 evaluated elastography for biopsy guidance for PCa detection. After imaging with conventional grayscale US in conjunction with real-time elastography, 404 men underwent systematic sextant biopsy. PCa was found in 151 of 404 cases (37.4%). In 127 of 151 cases (84.1%), PCa was detected using real-time elastography as an additional diagnostic feature. They concluded that it is possible to detect PCa with a high degree of sensitivity using real-time elastography in conjunction with conventional diagnostic methods for guided prostate biopsies.
In a pilot study, patients with clinically localized PCa who underwent RP were examined. 28 Before surgery these patients were evaluated with conventional grayscale US as well as with real-time elastography. Areas suspicious for PCa were depicted. After surgery the histological specimens were compared with the transverse US images and with elastography findings. Thirty-two foci of PCa were present at pathologic evaluation, with multiple foci of cancer in 13 of the 15 glands. Real-time elastography detected 28 of 32 cancer foci (sensitivity: 88%). Four sites were false-positive with no pathological abnormality. The by-patient analysis demonstrated that real-time elastography detected at least one cancer foci in each of the 15 patients. Therefore, it was concluded that real-time elastography of the prostate is a sensitive imaging modality for the detection of PCa.
Further, Pallwein and colleagues 29 performed a study to determine whether a limited biopsy approach with sonoelastography (SE) targeted biopsy of the prostate would detect cancer as well as grayscale-US-guided SB with a larger number of biopsy cores. Two hundred and thirty male screening volunteers with a total PSA of 1.25 ng/mL or greater were examined. In each subject, five SE targeted biopsies into suspicious regions in the peripheral zone during elastographic examination versus 10 SB were carried out. Final cancer detection rate of the two techniques was compared. Cancer was detected in 81 of the 230 patients (35%), including 68 (30%) by SE targeted biopsy and in 58 (25%) by SB. Cancer was detected by targeted biopsy alone in 23 patients (10%) and by SB alone in 13 patients (6%). The overall cancer detection rate by patient was not significantly different. The detection rate for SE targeted biopsy cores (13%) was significantly better than for SB cores (6%). SE targeted biopsy in a patient with cancer was 2.9-fold more likely to detect PCa than systematic US-guided biopsy. In difference to the study of Konig et al 27 an increase in sensitivity and specificity was found including only the outer prostate gland. They concluded that although an increase in cancer detection was achieved by combining targeted and systematic techniques, elastography targeted biopsy alone would be a reasonable approach for decreasing the number of biopsy cores.
In a further study the value of elastography for PCa detection in comparison with SB findings in 492 patients was evaluated. 30 Elastography of the prostate was performed prior biopsy, to assess tissue elasticity, and areas with increased stiffness were considered as suspicious for cancer. On elastography 18% suspicious areas were detected and 48% of these areas showed cancer. Elastography findings showed a good correlation with the SB results. The best sensitivity and specificity was found in the apex region. In conclusion, elastography allowed exact assessment of the tissue elasticity and therefore for a good differentiation between benign and malign.
Salomon and colleagues 31 investigated US-based real-time elastography in a cohort of 109 patients undergoing RP. Correlating suspicious elastography findings with the whole-mount RP specimen yielded location-specific 75% sensitivity, 77% specificity, 88% PPV, 59% negative predictive value, and 76% overall accuracy. These results are superior to those obtained from conventional TRUS and suggest that elastographic observation of tumors may enhance the accuracy of biopsy and reduce the need for subsequent biopsies. Further, improved observation of tumors may lead to more targeted biopsies and reduce the number of biopsy cores that are required in a given biopsy session. The finding that elastography detected at least one tumor focus in every patient, implying 100% sensitivity for PCa diagnosis, has potential implications for PCa screening. It is important to note that this study was performed in men with an established diagnosis of PCa. Larger prospective trials that compare standard TRUS biopsy with elastography-enhanced TRUS biopsy and incorporating various biopsy schemes are required in undiagnosed men to determine the true benefit of elastography and whether it has a role in PCa detection and screening.
Recently, Hoyt and associates 32 evaluated tissue elasticity as a qualitative biomarker for PCa and SE as an emerging imaging tool for providing qualitative and quantitative measurements of prostate tissue stiffness. A viscoelastic model was used to characterize mechanical stress relaxation data measured from human prostate tissue samples. Mechanical testing results revealed that the viscosity parameter for cancerous prostate tissue is greater than that derived from normal tissue by a factor of approximately 2.4. It was also determined that a significant difference exists between normal and cancerous prostate tissue stiffness. Qualitative sonoelastographic results showed promise for PCa detection and may prove to be an effective adjunct imaging technique for biopsy guidance. Elasticity images obtained with quantitative SE agreed with mechanical testing and histological results. Overall, results indicated that tissue elasticity is a promising biomarker for PCa.
In summary, real-time elastography seems to be a good tool to improve PCa detection in US investigations and can be even used as a promising biomarker for PCa. However, further studies have to determine if it can be used to develop a targeted biopsy scheme that is at least as sensitive in tumor detection as an extended biopsy scheme (Figs. 3 –5).
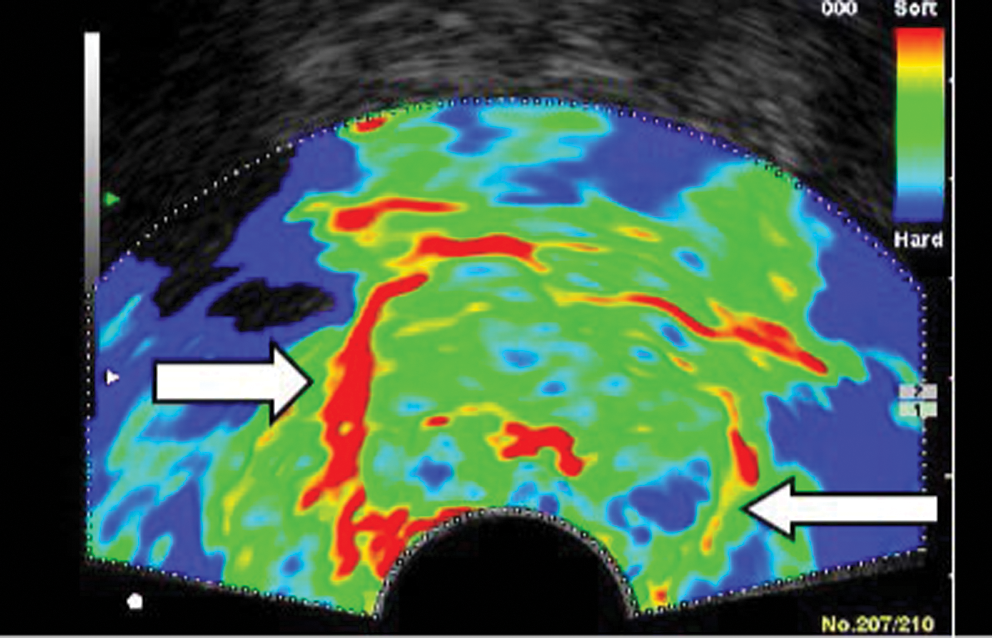
Real-time elastogram of the prostate. The transverse elastogram shows a clearly visible stiffer area (blue color) with suspicion of a prostate cancer on the left side of the prostate (arrow). The arrow on the right side shows the soft rim artefact (red color) of the prostate capsule.
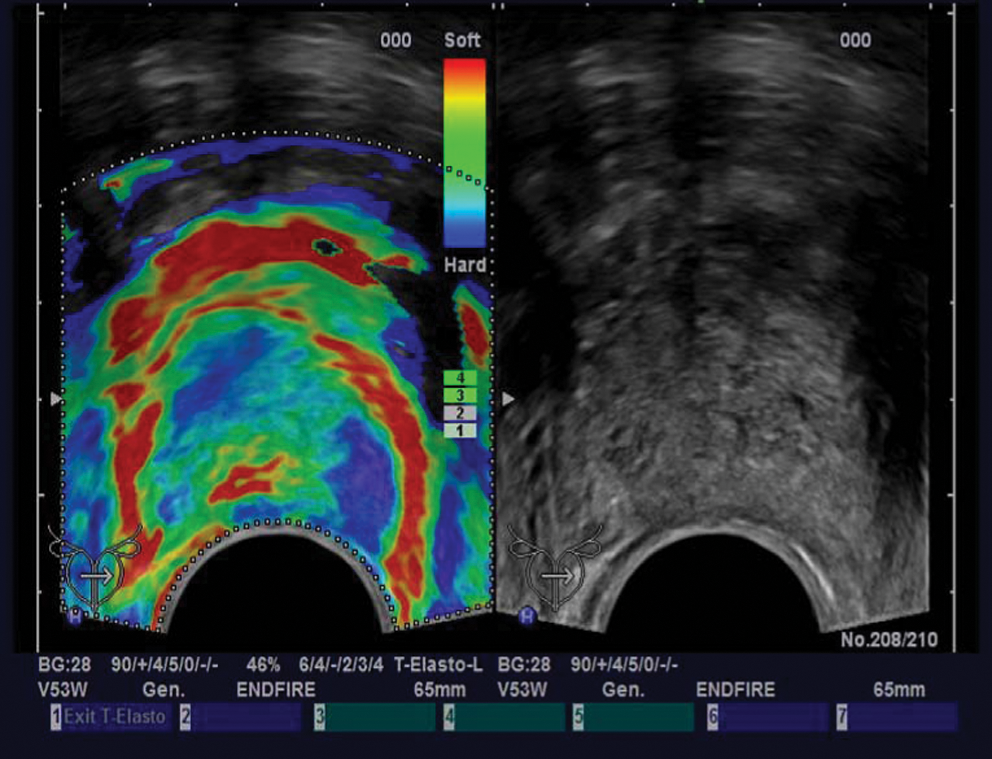
Real-time elastogram of the prostate. The transverse elastogram shows a clearly visible stiffer area (blue color) with suspicion of a prostate cancer on the left side of the prostate.
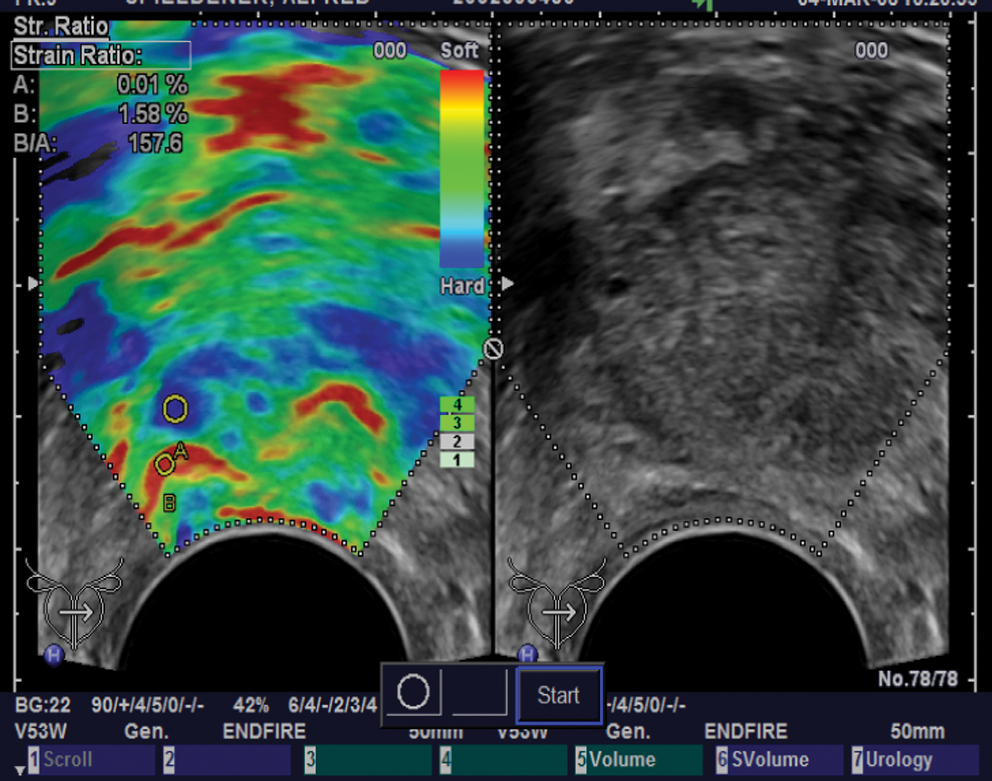
Real-time elastogram of the prostate. The transverse elastogram shows a clearly visible stiffer area (blue color) with suspicion of a prostate cancer on the right side of the prostate. The strain ratio (objective assessment of tissue elasticity) shows a value of 157.6.
Summary
Recent advances in US for the detection, grading, and staging of PCa are promising. New technical developments allow for improved detection of smaller, low flow vessels and better detection of areas of flow asymmetry. Mandatory quantification of enhancement will make an objective grading system available. CEUS and elastography seem to offer a novel and great potential in PCa diagnosis.
Footnotes
Disclosure Statement
Ferdinand Frauscher, M.D., was consultant to Bracco Imaging S.P.A.