
Abstract
Aim:
To provide an evidence-based analysis on the status and perspectives of laparoscopic training in urologic surgery.
Methods:
A thorough review of the current literature was performed as of January 31, 2009, using the Medline database through a PubMed search. The search protocol included a free-text query using the following terms: “training,” “urologic laparoscopy,” “urology,” and “laparoscopy.” Suitable articles were selected on the basis of the study content. The following issues were addressed: prediction of laparoscopic skills and transfer of training in clinical practice; homemade and commercially available laparoscopic trainers and simulators; training models for specific laparoscopic procedures; mentored training programs; formal training programs; and the impact of robotics in laparoscopic training.
Results:
Currently available tools predicting laparoscopic skills lack adequate validation to justify their widespread adoption. There still is not enough evidence to show definite transfer of skills from currently available simulators to the operating theater. Learning opportunities continue to evolve. Specific models have been developed for complex procedures. Various informal training programs exist, yet most urologists will not be able to complete a formal fellowship. Postgraduate urologists may possibly be more rapidly and efficiently trained using a structured mentoring program. Robotics is likely to have an increasing role in teaching urological laparoscopy.
Conclusions:
Despite progress in recent years and an extensive amount of data from the urological literature, the ideal training program in urological laparoscopy remains a goal to be determined objectively.
Introduction
Certainly, laparoscopy does require a set of skills much different from those of open surgery; among them are spatial orientation in a two-dimensional environment, manipulation of longer instruments with reduced tactile feedback, and accommodating the fulcrum effect. Laparoscopic-skill acquisition is in fact more difficult than that for open surgery, further validating the need for training. 4 Fahlenkamp et al 5 reviewed 2407 urologic laparoscopy cases and observed a decrease in the complication rate from 13.3% to 3.6% after the first 100, highlighting the inadequacy of laparoscopic training before entering the operating room.
The aim of the present review is to provide an evidence-based analysis of the status and perspectives of laparoscopic training in urologic surgery.
Methods
A critical nonstructured review of the literature was performed as of January 31, 2009, using the Medline database through a PubMed search. The search protocol included a free-text query using the following terms: “training,” “urologic laparoscopy,” “urology,” and “laparoscopy.”
Suitable articles published in English from peer-reviewed journals were selected on the basis of the study content. Abstracts of congresses were not included. Potentially relevant articles from references of included articles were also retrieved.
The following issues were addressed: prediction of laparoscopic skills and transfer of training in clinical practice; homemade and commercially available laparoscopic trainers and simulators; training models for specific laparoscopic procedures; mentored training programs; formal training programs; and the impact of robotics in laparoscopic training.
For each of these issues, a response has been formulated in form of take-home message summarizing the current available evidence.
Results
Transfer of training to surgical practice: can we predict a good laparoscopic surgeon?
The ability to predict surgical performance remains an open issue in the use of simulators or wet-lab for competency assessment. It is not yet clear how effectively skills obtained within a laboratory environment can be transferred into a real-life clinical setting.
See et al 6 and Colegrove et al 7 followed urologists who had participated in laparoscopy training courses at the University of Iowa in 1991. Although their 1-year follow-up showed that 84% of the respondents had performed at least one laparoscopic procedure since the training course, follow-up at 5 years revealed a decline to 54%. Completion of a 12-month laparoscopic urology fellowship has been linked to an increased productivity by Cadeddu et al. 8 This was also confirmed by Shay et al, 9 who suggested that laparoscopic procedures are more likely to be performed by physicians receiving laparoscopic training during urology residency.
Gettman et al 10 found that basic human performance resources could be used to predict laparoscopic performance, suggesting that a surgeon's innate laparoscopic ability could be predicted by measuring objectives such as visual-information-processing speed, upper-extremity steadiness, and isometric strength. On the basis of the preliminary results of those researchers, McDougall et al 11 assessed whether basic elements of performance (i.e., immediate memory recall, hand–eye coordination, two-handed coordination, reaction time, hand steadiness, and upper-limb isometric strength) could discriminate among resident applicants and urologists with various extents of surgical experience, but they were not able to predict the surgeon's laparoscopic expertise or experience. Similarly, Abdelsheid et al 12 did not find any correlation between the performance of laparoscopy and participation in activities requiring bimanual dexterity.
Rosenberg et al 13 sought to discover if video-game aptitude predicted performance in a live laparoscopic model and concluded that video games do improve one's hand–eye coordination, possibly predicting inherent laparoscopic skill in the novice surgeon.
Traxer et al 14 used urology residents to assess the impact of intense laparoscopic skills training on the performance of porcine laparoscopic nephrectomy. They found no significant difference between study and control groups when reassessed at the end of the 10-day study and concluded that completing an initial baseline laparoscopic nephrectomy appeared most important for improving operative performance.
Standardized programs on box trainers can be used to assess baseline laparoscopic skills and to track residents' improvement over time. 15 The McGill Inanimate System for Training and Evaluation of Laparoscopic Skills (MISTELS) consists of a series of five laparoscopic exercises (peg transfer, pattern cutting, ligating loop, and suturing with extra- and intracorporeal knots) performed in an endotrainer box. Dauster et al 16 verified the construct validity of the MISTELS simulator in urology by comparing the performances of two groups of urologic surgeons with different degrees of clinical laparoscopic experience.
The use of fundamentals of laparoscopic surgery (FLS) is basically developed from the MISTELS Training and Evaluation System. This program is now required as part of General Surgery Residency Training by the American College of Surgeons (
Looking at the quality of performance in the pelvic box trainer, Katz et al 18 were unable to distinguish between novices and someone with minimal experience. In commenting on this article, Guillonneau stated that the idea that all surgeons with a given score are interchangeable is dangerous.
Take-home message
Although there is a wide variability in the literature, we can assume that simulators currently have the ability to teach basic laparoscopic skills, enabling novice surgeons to progress along the learning curve before performing the procedure on a patient. However, currently available tools predicting laparoscopic skills lack adequate validation and there still is not enough evidence to show definite transfer of skills to the operating theater. 19
To note that, recently, the American College of Surgeons and the American Board of Surgery have adopted a very specific basic laparoscopic skills testing, based on general surgery simulation literature, for certification requirements.
From commercially available simulators to homemade lap-trainers: where are we?
A number of simulators with various degrees of complexity have been introduced in almost all medical fields. They can be divided into three main groups depending on the type of technology used 20 (Table 1).
Table adapted from Undre S, Darzi A. 19
Efforts to create a home training system resulted in products such as the SIMENDO™ virtual reality trainer (
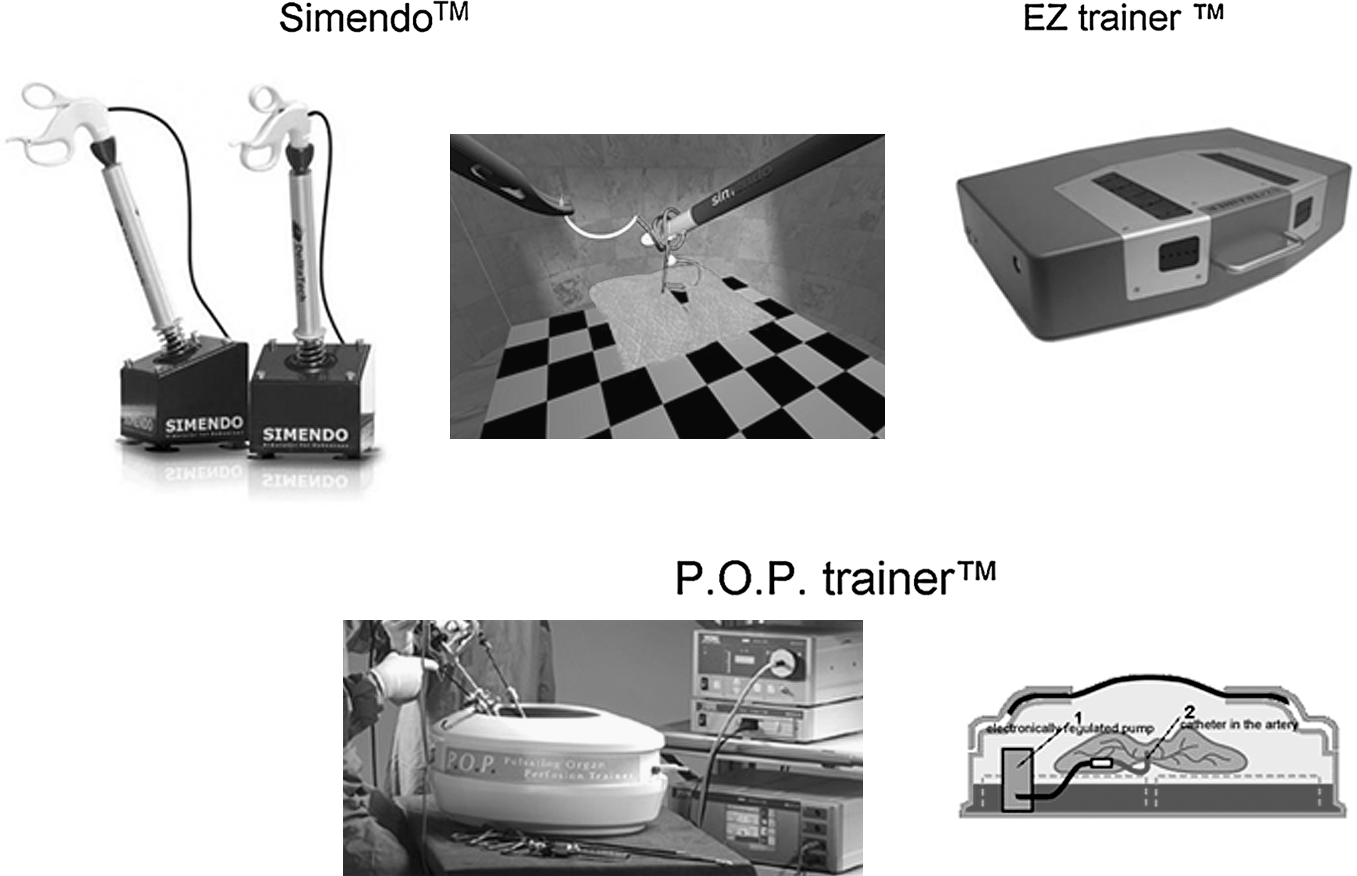
Recent commercially available laparoscopic simulators.
The idea of homemade simulators has been much developed in the last decade (Table 2). Chung et al 24 reported on a trainer consisting of a cardboard box using a webcam to transmit images to a computer. A similar model has been described by Blacker. 25 Beatty 26 carefully described how to build an inexpensive webcam-based trainer, yet no formal assessment of his training tool was performed. Similarly, Ricchiuti et al 27 described a template for a cheap easy-to-construct lap trainer. Griffin and colleagues 28 prospectively evaluated whether a home-constructed laparoscopic training system, consisting of a camcorder, television, and box trainer, could be used to learn intracorporeal suturing skills.
n/r = not reported; n/d = not done; n/a = not applicable; FA = face validity; CR = criterion validity; USD = United States dollars; GBP = Great Britain pounds.
However, these above-mentioned models still involved the use of a camera system with an audio-visual unit that, though less expensive than conventional commercially available video-laparoscopy pelvic trainers, still requires significant investment. A camera-less system has been described by Sharpe et al. 29 In their study, residents had similar rates of improvement using that system compared with a conventional trainer. Similarly, Chandrasekera et al 30 assessed the effectiveness of a cheap and simple training model made using a cardboard box compared with a conventional pelvic trainer. Medical students without previous surgical skills were randomized into two groups. When assessed on the video trainer, the cardboard-box-trained group had significantly faster times with equivalent scores in the majority of tasks.
A series of tests (validity measures) are necessary to provide the required evidence that the trainer is able to teach the skills it purports to teach: face, content, criterion (including concurrent and predictive), and construct validity 31 (Table 3). In particular, the process of transferring skills from simulators to patients (predictive validity) seems to be quite complex, for several possible reasons. On one hand, it appears to be affected by factors other than only specific task-related skills. On the other hand, the lack of studies assessing the predictive validity in laparoscopic urology may be partly due to difficulties in designing randomized studies similar to those reported in general surgery for cholecystectomy as the most frequently performed laparoscopic procedures in urology involve complex surgical steps.
Table adapted from Chandrasekera SK, Donohue JF, Orley D, et al. 30
Take-home message
Overall, a surgical simulator must have proven validity as a training device. Unfortunately, most of the reported home training devices mostly lack any scientific validation, not allowing any definitive conclusion in this evolving field.
Challenging urolaparoscopic procedures: do we have reliable training models?
Partial nephrectomy
Laparoscopic partial nephrectomy (LPN) remains extremely challenging and has a steep learning curve (Table 4). 32 To date, few options exist for in vivo LPN training models. Taylor et al 33 were the first to provide a report of a mimic model for renal tumors. They used an agarose-based model injected percutaneously into porcine kidneys to create endophytic lesions. Hidalgo et al 34 assessed the reliability of a porcine tumor training model as a surgical education tool for teaching LPN. They used a subcapsular injection of liquid plastic in pig kidneys to produce a mean tumor diameter of 2.2 cm. Attempts to create more central lesions were recognized as the limitation of this model. More recently, Eun et al 35 developed and described a novel technique of creating solid renal tumors and tumor thrombi to be used for training. They injected various substances and found that the most ideal pseudotumor models were created from a mixture of gelatin, Metamucil,® and methylene blue (metagel) or from Kromopan® hydrocolloid. Renal pseudotumors were created percutaneously and endoscopically using eight live pigs and a human cadaver model. A renal vein pseudothrombus porcine model was also created by injecting pseudothrombus material into the renal vein after renal hilar clamping.
Face validity: ability to depict what trainer is supposed to represent as assessed by nonexperts; Content validity: subjective measure of the appropriateness of the trainer; Construct validity: ability to discriminate between naive and experienced subjects; Concurrent validity: correlation with performance in the gold-standard model for training; Predictive validity: correlation with the actual performance in the operating room.
LPN = laparoscopic partial nephrectomy; LP = laparoscopic pyeloplasty; LRP = laparoscopic radical prostatectomy.
Pyeloplasty
Ooi et al 36 proposed a training model for both open and laparoscopic pyeloplasty. They constructed a renal pelvis from reconfigured chicken skin, which is readily available at low cost. More recently, Ramachandran et al 37 created a model for laparoscopic pyeloplasty training using the crop and esophagus of a chicken. The chicken was positioned within a homemade laparoscopic training box, and laparoscopic dismembered pyeloplasty was performed. The model was used over a period of 1 month by three urology trainees who were assessed on time needed to complete anastomosis and quality of anastomosis. There was a significant improvement in the quality of anastomosis from the first to the fourth attempt. At the end, all trainees were able to satisfactorily complete a good-quality anastomosis.
McDougall et al 38 first described a porcine model to explore the feasibility of laparoscopic pyeloplasty. In this model, ligating the ureter created secondary ureteropelvic junction obstruction, and after 6 weeks the enlarged renal pelvis was suitable for operation. Chiu et al 39 also described a porcine model of ureteropelvic junction obstruction using a laparoscopic technique and assessed the outcome of standard suture-assisted and chemical-glue-assisted laparoscopic pyeloplasty. Recently, Fu et al 40 also detailed a porcine model for teaching laparoscopic pyeloplasty. With training, all participants were able to perform ureteropelvic anastomosis and intraoperative antegrade stenting skillfully.
Radical prostatectomy
Laparoscopic radical prostatectomy (LRP) represents a test of several ablative and reconstructive skills. 41 Even if the learning curve for LRP has been estimated to be 40 to 100 cases, 42 it has been shown that surgeons continued to improve in terms of operative time even after 300 cases. 43 However, the adherence to numerical values is of no particular importance as one must consider that the knowledge and manual skill of various trainees may differ significantly, which means that some will achieve competence before others. 44
The urethrovesical anastomosis is a crucial challenging step in LRP. Katz et al 45 developed an in vitro model for the urethrovesical anastomosis using chicken skin. The training was performed on a pelvic trainer with a video laparoscopic unit and consisted in five tasks: passage of a ligature, intracorporeal knot-tying, intracorporeal suturing, linear anastomosis, and circular running suture anastomosis. In another report by the same group using the same training model, two junior trainees practiced a circular urethrovesical anastomosis exactly reproducing the steps that are followed during the clinical operation. Memorizing these steps and gaining of manual dexterity in manipulating the needle were the main factors influencing the time needed to complete the task. After practicing with the chicken skin model, the trainees were able to create a watertight vesicourethral anastomosis in a mean time of 40 minutes. 46
Yang and Bellman 47 demonstrated how the simple and inexpensive model proposed by Katz and Nadu model can be used by Accreditation Council for Graduate Medical Education-certified urology residency programs to assess the laparoscopic skills of residents.
Laguna and coworkers 48 explored the construct validity of a simulation for the urethrovesical anastomosis. Five subjects with different levels of experience in laparoscopy tested two types of suture. The tested model discriminated between inexperienced and experienced subjects, but failed to reflect the different levels of experience among the most experienced subjects.
Boon et al 49 examined the construct validity of a porcine intestine model for performing a laparoscopic urethrovesical anastomosis. Subjects with different levels of experience performed a running laparoscopic anastomosis. Tests of performance time and postoperative leakage accurately reflected the subjects' degree of experience.
Jiang et al 50 evaluated another in vitro training model using the posterior trunk of a chicken (to simulate a human pelvis), a cloacal stump (to simulate a human urethral stump), and a porcine colon with an orifice (to simulate a human bladder).
Although the use of chicken skin mimics the characteristics of human tissues and is readily available, the use of this model requires special preparation and the conservation of fresh chicken tissue can also be difficult. More recently, Poulakis et al 51 developed a simple and practical model with the use of Gore-Tex® Vascular-Graft, which has comparable consistency as human urethra and bladder neck, representing the laparoscopic urethrovesical anastomosis. One limitation of this model was its cost.
Considering the need for an inexpensive readily accessible inanimate model, investigators from University of California–Irvine developed a simple, inexpensive, reusable model (LapED® 4-in-1 silicone model). This was the first to address procedure-specific training in laparoscopic reconstructive urologic procedures. Both content and face validity of this model were evaluated. 52
Take-home message
Much effort has been put in the last years into the development of training models for what are considered the most challenging laparoscopic procedures in urology. Despite this commendable effort, further validation of these models is necessary before defining their role in structured laparoscopic training programs.
From videotape analysis to mentoring: how to improve laparoscopic skill transfer?
Various options for learning specific laparoscopic skills have been developed over the years through which a combination of nonclinical (pelvic trainer, animal laboratory-based laparoscopic courses, and didactic lectures) and clinical (fellowship and mentorship) training is used (Table 5). In this way, laparoscopic skills can be developed during a longer period and under the direct guidance of a colleague with laparoscopic expertise. 53
McNeill and Tolley 54 made their suggestion of a training pathway to gain competency in laparoscopic urological surgery. It starts with a basic skills course followed by independent practice in simulator training models and assisting in laparoscopic procedures. Then, the trainee should attend an advanced skills course and an animal laboratory program, followed by performing mentorship-guided laparoscopic procedures until being competent enough to perform laparoscopy independently.
Thus, mentoring has been largely advocated as a critical component of laparoscopic skills acquisition. Investigators from Duke University assessed the impact of mentoring on the clinical practice of hand-assisted laparoscopy by evaluating clinical practice patterns of urologists following a postgraduate course and comparing course graduates who underwent subsequent mentoring with those who were not mentored. 55 Mentoring provided a useful adjunct to postgraduate training for integration of laparoscopic techniques into community-based practice.
In their experience, Shalhav et al 3 developed a three-phase “mini-fellowship” model including hands-on course on pelvic trainers and animal laboratories, observation, and mentored-performance. Their model, although challenging to accomplish, did improve the likelihood of the trainees assimilating this surgical technique in their clinical practice.
Similarly, Rane 56 proctored postgraduate urologists during a nine-phase training model. The trainee was recommended to perform a mean of 10 mentored cases before independently performing laparoscopic procedures. Fabrizio et al 57 reported that expert mentoring also was valuable to an experienced laparoscopist learning a new complex operation such as LRP.
There are obstacles to the mentored mini-fellowship approach, relevant among them being the time commitment required of both the trainee and the mentoring surgeon. Taking time out of a busy clinical practice to travel to and from another hospital to observe or mentor a series of operations is not time efficient. Compensation is another area of possible contention. The need to obtain temporary operative privileges and medical malpractice coverage at another hospital further confounds mentorship programs.
In an effort to reduce the overall time commitment of mentoring surgeons, Nakada et al 58 applied the “golf school” concept of videotape mentoring to teaching advanced laparoscopic techniques to urologists during a 2-day course. They were able to demonstrate that urologists with some laparoscopic experience could improve specific laparoscopic skills using mentored videotape analysis and experience gained from the course. The same investigators subsequently showed that videotape critiquing used in postgraduate laparoscopic training is durable and benefits the clinical practice patterns of former course participants by increasing their laparoscopic caseload. 59
An approach adopted by Jones and Sullivan 60 has been one of “mutual mentoring.” These two authors pursued a laparoscopic fellowship at the same stage and have then performed joint procedures at each of their new institutions. They found this invaluable in terms of camera assistance, a “second opinion” during surgery, and joint operating with the longer cases. This approach benefited both parties equally, thus being much more sustainable even if geographically restrictive and time consuming.
Investigators from Bordeaux devised a four-step program: observation, theoretical learning, assisting, and operating. 61 A standardized step-by-step program to improve laparoscopic skills and enable trainees not experienced in laparoscopy to perform urethrovesical anastomosis was proposed by Rassweiler and his group. 62 In an inanimate model (pelvic trainer) with defined trocar positions, participants were exposed to six reconstructive exercises. After a mean of 40 hours of training, participants were able to perform all steps within the specified times, completing an accurate urethrovesical anastomosis in 30 minutes.
The same group divided LRP into sequential steps and developed a series of models to simulate the steps. 63 The model simulated urethrovesical anastomosis using porcine bladder and urethra, and 11 surgeons with different laparoscopic expertise were trained and then performed LRP in the operating room. For the novices, there was no significant difference in the time to complete the urethrovesical anastomosis model and the human urethrovesical anastomosis of LRP. Further, there was no significant difference in watertight quality between the levels of laparoscopic experience, supporting the predictive validity of the training model.
Stolzenburg et al 64 developed a modular scheme that enabled them to use individual steps of extraperitoneal LRP for teaching and training. The procedure has been divided into 12 segments with 5 levels of difficulty; the aim of this categorization is to maximize standardization. Rigid adherence to this modular teaching concept equipped the trainees with the appropriate skills to overcome intraoperative difficulties and progress rapidly from module to module. Residents were able to perform the entire procedure following almost 40 sessions with an operative time, success rate, and complication rate equal to their mentors.
These findings concur with those of Frede et al, 65 who had shown that, based on the Heilbronn step-by-step training program, the personal level of education and prior experience with open radical prostatectomy had a minor impact on the results and reproducibility of the LRP technique. Since none of the patients in the study by Stolzenburg et al 64 required conversion to open surgery, one could indeed question the classic belief that surgeons can only consider laparoscopic procedures once they have a considerable experience with the open operations.
Take-home message
Probably the most important issue regarding training is the ultimate outcome of surgery and safety of patients. The modular training scheme suggested enables the mentor to ensure that the trainee has acquired the requisite skill of each level before progressing to the next step of the procedure. This allows completion of each module to the highest of standards and allows prompt intervention by the mentor when the trainee is failing to progress, ensuring patient safety. Nevertheless, further assessment and validation of these modular programs is desirable.
Regardless of the number of complex learning models for training, the key common denominators required for a good program can be theoretical courses, out-of-theater training on box or pelvic trainers, wet laboratory experience, mentor guidance as assistant or participant in a minimum number of cases, and performance at the trainee's unit under the scrutiny of the mentor. 66
From mentoring to formal laparoscopic training: where do we stand?
Ideally, residency training should provide a basic skill set sufficient for residents to be comfortable when applying laparoscopy to their subsequent practice (Table 6). However, quantifying resident exposure to laparoscopy is difficult to ascertain and the number of index cases required for proficiency remains unknown. Duchene et al 67 surveyed via Internet residents and program directors in the United States and Canada in 2005. Overall, only 38% of residents thought that their laparoscopic experience was at least average or acceptable, whereas 31% stated that it was poor. Improvements have been made in laparoscopic experience at training institutions because 39% of chief residents believed that their laparoscopic experience was at least average in this survey compared with results in a 2003 survey of Midwest urologists, in which only 15% believed that they were adequately trained in residency to perform laparoscopy. 68
BAUS = British Association of Urological Surgeons; ACGME = Accreditation Council for Graduate Medical Education; NCI = National Cancer Institute.
An intensive 5-day mini-residency (M-R) program has been created at the University of California–Irvine. 69,70 Acquisition of laparoscopic skills is assessed by testing participants at the beginning and at the end of the M-R. A questionnaire on laparoscopic practice patterns was sent to the initial 32 participants in the laparoscopic ablative or reconstructive renal surgery M-R, after completion of the course. 69 Twenty-six participants (81%) were performing some form of laparoscopic surgery after their M-R. More of the participants were performing laparoscopic radical nephrectomy, nephroureterectomy, and pyeloplasty. These data support the use of a focused, intensive 5-day M-R in assisting postgraduate urologists with the acquisition of laparoscopic and robot-assisted laparoscopic skills that are applicable to their clinical practice.
Even if training in laparoscopic techniques is variably offered by some residency programs, advanced laparoscopic training has been reserved primarily for those pursuing fellowships. Historically, fellowship training in laparoscopy has been provided through fellowships supported by the Endourological Society. However, Society of Urologic Oncology (SUO) fellowships are now offering extensive laparoscopy experience, given the benefits of this technique in extirpative surgery for certain urologic malignancies.
Yap et al 71 compared the laparoscopy experience offered by Endourological Society and SUO fellowship programs to determine whether career paths differed between Endourological Society and SUO trained fellows. At the time of their survey, the majority of Endourological Society program directors reported fellows performed more than 100 laparoscopic procedures, whereas only 25% of SUO fellowships offered a similar experience. Thus, Endourological Society–trained fellows seem to have more exposure and experience in laparoscopic techniques. This may be because SUO fellowships provide a broader surgical training, with exposure also to open surgery.
The British Association of Urological Surgeons presented guidelines for urological laparoscopic training in the United Kingdom. 72 According to these guidelines, laparoscopic training should be rooted in simulation and augmented with intraoperative experience. Specifically, these guidelines suggest that training should combine hands-on practice of basic laparoscopic skills, consisting of practice on bench models, assisting in and observing various laparoscopic urological procedures, in addition to an advanced skills course with operative experience on cadaver or animal models.
When laparoscopic urology was in its infancy, there were no experienced urological surgeons to act as mentors; consequently, consultants who were still going through the learning process were trying to guide others. As many surgeons now have extensive experience, there is now a need to identify those who are able to act as mentors. Addressing this crucial question, the British Association of Urological Surgeons provided the minimum requirements to define a mentor. 73
One of the major deficiencies in all of the validity testing that has been done to date on various surgical education programs for minimally invasive urologic surgery is the lack of outcomes data related to these training programs. The closest program to come to acquiring these data is that related to the Japanese endoscopic surgical skill qualification system in urological laparoscopy, which has been established by the Japanese Urological Association, and Japanese Society of Endourology and ESWL. 74 This tool tests the ability to complete common laparoscopic surgeries in each field, and it is now being utilized in Japan as a criterion for surgeon privileging for doing these laparoscopic procedures in their local hospitals. It has also recently been shown to have construct validity.
In Denmark a new model was recently developed and guided by three principles: an agreement on the basic theoretical concepts and practical laparoscopic skills between surgery, gynecology, and urology; a collaboration between the specialties to ensure innovation in education; and a research to continuously evaluate the quality of training. Trainees are encouraged to borrow portable trainers to practice independently before the expert-guided learning portion of the course. In addition, the trainees receive a package with readings, access to websites, and a CD-ROM with expert instruction identifying various laparoscopic exercises. 75
Take-home message
Learning opportunities continue to evolve, including short courses, mini-apprenticeships, full-time fellowships. The traditional pathway to appropriate training appears to involve completing a residency program followed by an intense fellowship experience.
The number of trainees who have been accommodated by the available educational programs remains low compared with the total number of urologists within each of these countries that would require to be adequately trained. This represents an important existing limitations of the current educational curricula.
Formal institutional programs must continue to make a concerted effort to provide an intense hands-on experience to trainees in all minimally invasive surgical aspects. Training programs, however, are variable in the quantity and manner in which laparoscopy is incorporated within their curricula. The ideal future training program will likely include a concentrated experience with dedicated faculty members in residency or fellowship supplemented with a rich experience in large animal surgery and surgical simulation.
Robotics: what the future holds?
Robot-assisted surgery is rapidly gaining popularity among urologists, and there is no doubt that most residents believe that robotic training is necessary and important to their future. 76 On the other hand, the availability of the robotic systems to only a limited number of centers reduces surgical training opportunities.
Robotic technology may reduce the learning curve for complex laparoscopic procedures as the attributes of robotics, such as motion scaling, three-dimensional observation, and articulated instrumentation, allow complex reconstructive procedures to be performed with greater dexterity, more quickly, and more easily by a greater number of surgeons.
Even with these theoretical advantages, there are scant data in the medical literature that show that robotic technology can actually improve surgical procedures. In their in vitro model, Sarle et al 77 demonstrated how the da Vinci robot allows the novice laparoscopic surgeon to perform complex tasks and that robotic assistance might help skilled open surgeons learn. These in vitro findings were also consistent with another report from the same group suggesting that robotic assistance might help skilled open surgeons to learn laparoscopic procedures. 78 Ahlering et al 79 confirmed that both for experienced and for inexperienced laparoscopic surgeons, the learning curve of the device is shorter than that for standard laparoscopy.
Incorporating robotic training into any residency program poses significant challenges: above all, resident involvement should not have a negative effect on the outcome. Traditionally, this was ensured by the teaching surgeon's constant presence and direct instruction during surgery. With the robotic system, the surgeon sits separately at a console and the first assistant is at the table side. It is therefore essential that robotic surgical educators have a comfort level both with performing the surgical procedure and communicating with the assistant to teach the procedure. At present, however, the only laboratory-based experience available for training with the da Vinci surgical system is to use the system on inanimate, cadaveric, or animate models. 80 With the growing number of robotic procedures being performed each year worldwide and the growing applicability of robotic surgery in many subspecialty areas of urology, proficiency with surgical robotics may well become thought of as a basic urologic skill in the foreseeable future. 81
Take-home message
As the field of robotic surgery continues to grow, it is likely that robotic learning programs will be implemented in the near future and fully incorporated in postgraduate medical education.
Conclusions
A well-structured training curriculum in laparoscopy should combine education, that is, acquisition of knowledge, and training, that is, acquisition of cognitive and psychomotor skills. Ideally, a combination of inanimate models, animal labs, clinical exposure, and individual review of experience likely represents an effective curriculum for training in laparoscopy. The exact combination of these components to optimize experience and efficiency of learning is still debated (Fig. 2). Despite the progress of recent years and an extensive amount of data from urological literature, training in uro-laparoscopy remains a field of controversial issues requiring further investigation.
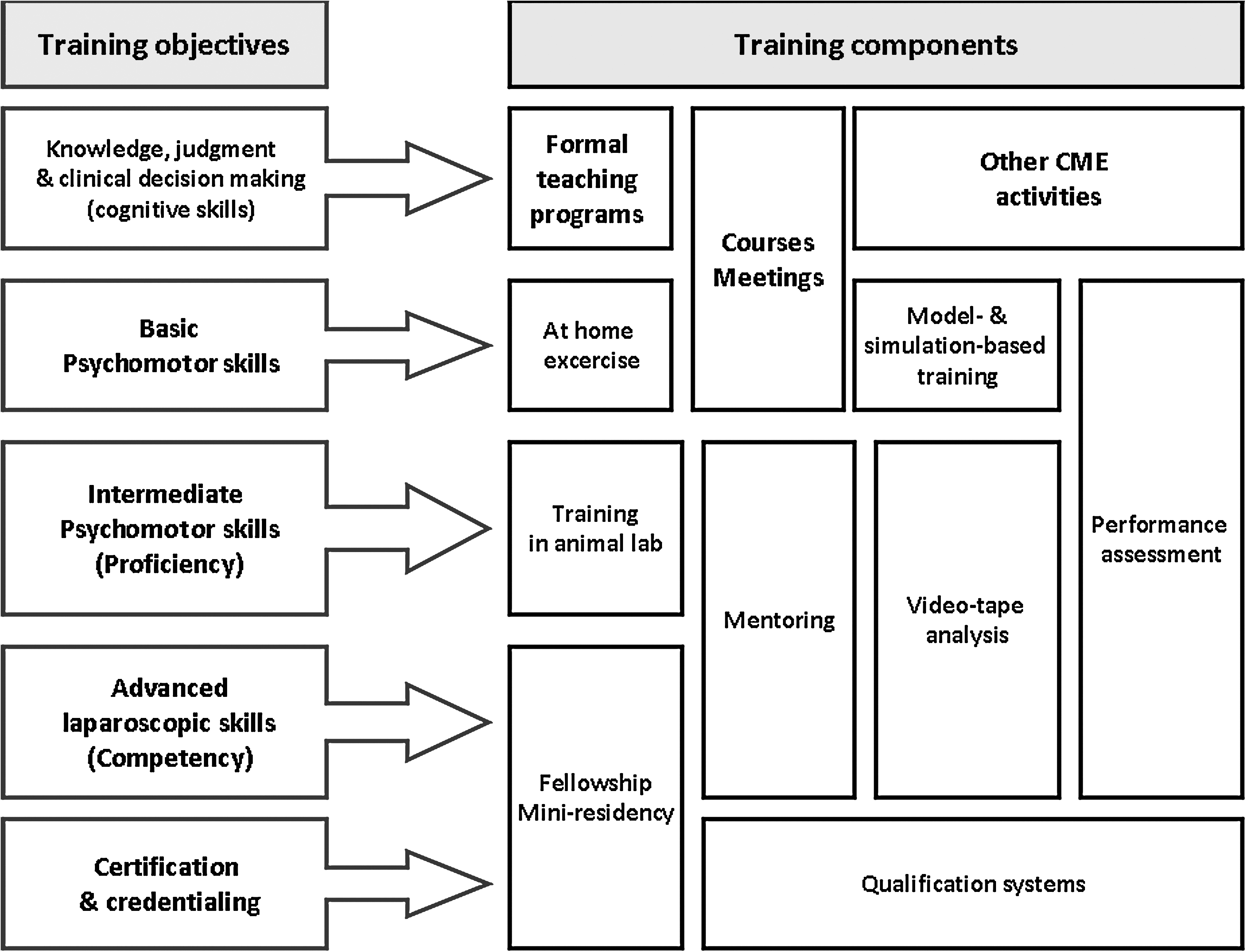
Minimum components of a curriculum in uro-laparoscopy.
Disclosure Statement
No competing financial interests exist.