
Abstract
Purpose:
Occasionally during percutaneous surgery, significant contrast extravasation obscures the field, making fluoroscopic access no longer feasible. Herein, we describe a salvage technique.
Materials and Methods:
The cystoscopically placed, open-end ureteral catheter is exchanged with an angled-tip angiographic catheter. With the aid of a guidewire and under fluoroscopic guidance, the tip of the catheter is placed in a posterior calix. The “bull's eye” technique is then applied to direct the needle into the tip of the catheter. This technique was used in four cases over a 7-year period.
Results:
Successful access was accomplished in all cases through a middle or upper calix.
Conclusion:
The catheter serves as a target for providing access to the renal collecting system and facilitates final tract dilatation.
Problem
Technique
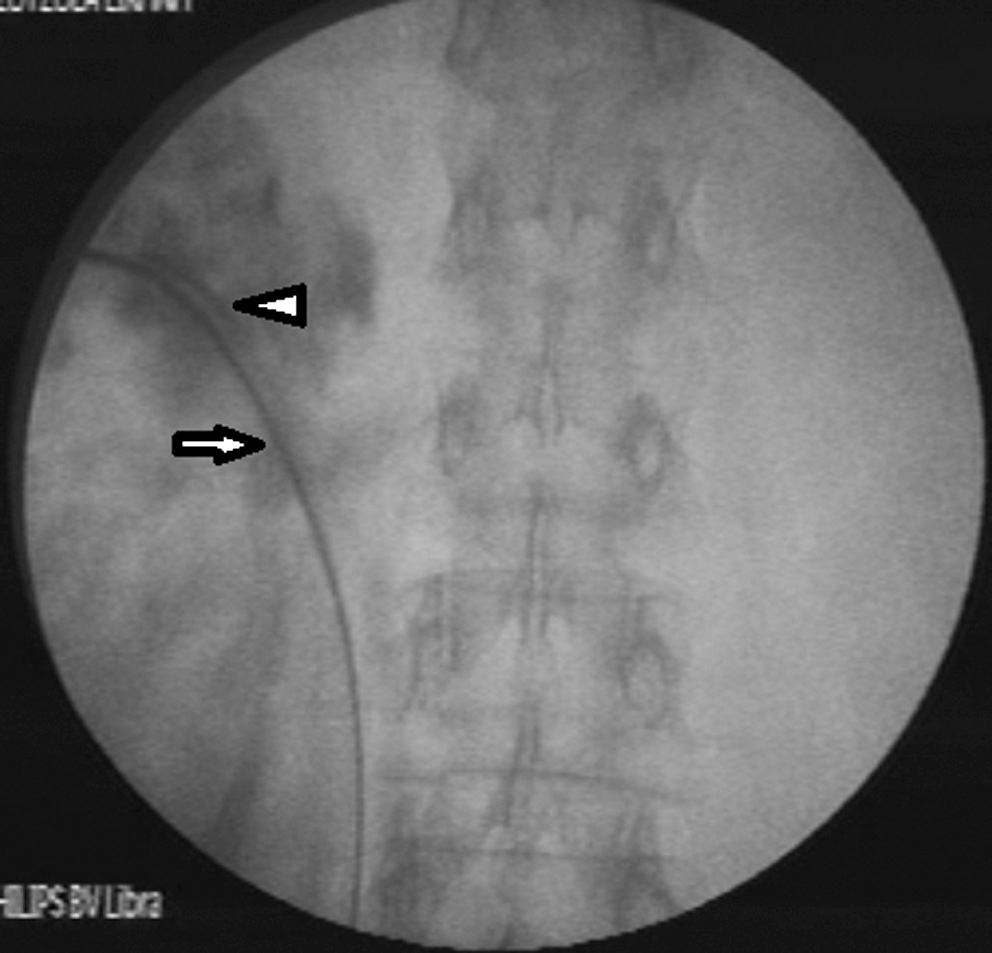
While the patient is in the prone position, a 0.038-inch guidewire is inserted through the initially placed, open-end ureteral catheter, and the latter is exchanged with an angled-tip angiographic catheter (5F, MPA angiographic catheter; Cook, Bloomington, IN) (Fig. 1). The enhanced radiopaque angled tip of the angiographic catheter allows for easy identification using fluoroscopy despite diffuse contrast extravasation (Fig. 2). With the aid of a guidewire inserted through the angiographic catheter and under fluoroscopic guidance, the tip of the catheter is placed in a posterior calix of the middle or upper caliceal group. Because the pelvicaliceal system is no longer visible fluoroscopically, the correct position of the catheter in a posterior calix is confirmed by rotational movement of the C-arm. When the image intensifier is rotated toward the surgeon, the angled tip of the catheter moves toward the midline, which is similar to what a posterior calix would typically do. Additionally, when the image intensifier is placed at an angle of 20° to 30° from the vertical plane, the angled tip of the catheter is seen end-on. Conversely, when the image intensifier is rotated away from the surgeon, a lateral projection of the tip of the catheter is obtained, demonstrating the full length of the angled tip on the screen (Fig. 3). These movements mimic the respective movements of a posterior calix when fluoroscopy is used for correct orientation before attempting puncture. However, these movements are obtained only with an angled-tip catheter and not with a straight-tip ureteral catheter. If the expected movements of the tip are not seen on the screen, the tip of the catheter has to be repositioned with the aid of the guidewire and fluoroscopic control. This is feasible with patience and persistence on behalf of the surgeon. Manipulation of the catheter in conjunction with the guidewire ensures that the tip is not left inadvertently within the renal pelvis because the guidewire indicates the route toward the most distal parts of the collecting system (i.e., the calices). It is very helpful to have an intravenous urogram film available or an initial normal fluoroscopic image before extravasation, which is captured on the second monitor of the fluoroscopy unit. Either of these help the surgeon discern the caliceal anatomy and help to accordingly manipulate the catheter toward a posterior calix. If any doubt regarding the correct position still exists, it is preferable to insert the catheter directly into the upper calix, which usually offers excellent access to the entire collecting system, though a supracostal access is often inevitable.
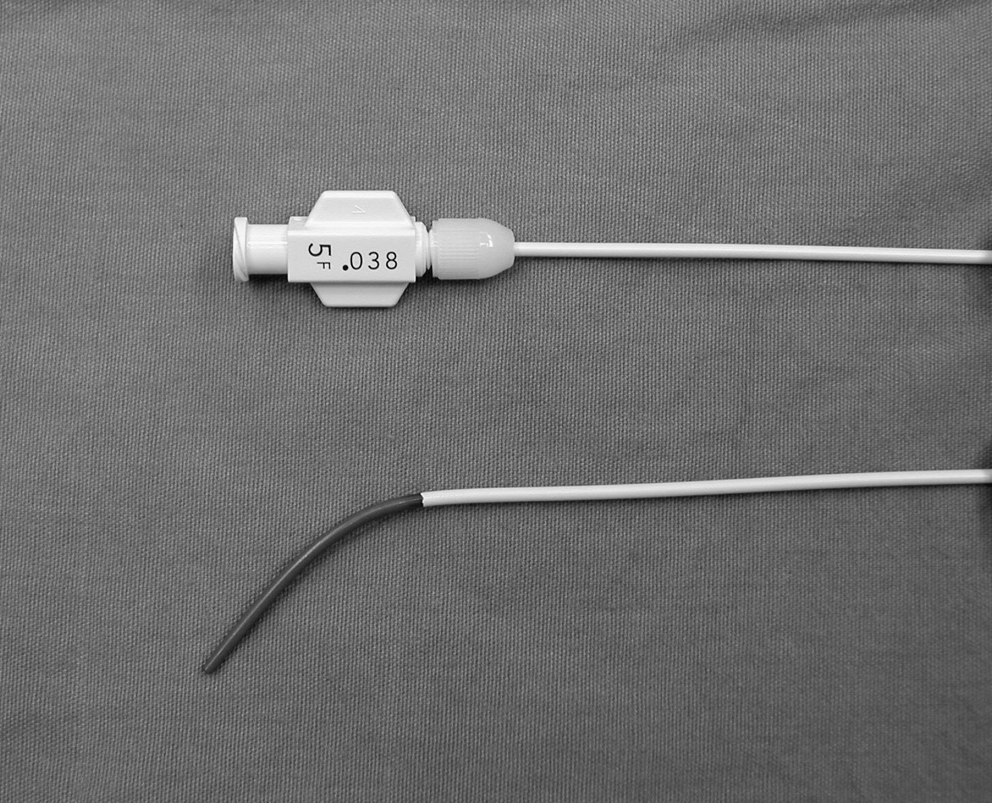
The angiographic catheter (5F MPA; Cook). The enhanced radiopaque distal part is in black.

(

(
When the position of the catheter is considered satisfactory, the C-arm is rotated ∼30° toward the surgeon so that the tip of the catheter is seen end-on, and the “bull's eye” principle is applied. Using a hemostat, the needle is directed into the tip of the catheter (Fig. 4). After the needle is stabilized at its trajectory, the C-arm is rotated away from the surgeon, and the tip of the needle is appropriately advanced so that it is placed next to the tip of the catheter, thereby placing it within the calix (Fig. 5). A guidewire is inserted into the renal collecting system and advanced down the ureter (Fig. 6). The subsequent final dilatation of the tract is performed with the angiographic catheter in place. The tip of the catheter again serves as a guiding point, which indicates the calix and helps determine the correct depth of insertion of the dilators. Although Amplatz plastic dilators still can be used, we have found that the procedure is much easier at this stage by using a balloon dilator. Placing the distal radiopaque marker of the balloon dilator next to the radiopaque tip of the catheter, inflation of the balloon is safe. After placement of the Amplatz sheath, the rest of the procedure is executed in a typical fashion.

Using the “bull's eye” technique, the needle is directed into the tip of the catheter.

The C-arm is rotated away from the surgeon to monitor the depth of the puncture. The needle is advanced until its tip is in contact with the catheter tip, thereby lying within the calix.
The working guidewire is passed down the ureter, and an 8F dilator is placed over the guidewire (arrow). The tip of the catheter can also be seen (arrowhead), providing orientation during final dilatation of the tract.
Over a 7-year period, we used this technique in four cases of percutaneous nephrolithotomy. In two cases, extravasation occurred because of high pressure within the pelvicaliceal system after manual injection of the contrast; in the other two, extravasation occurred because of multiple failed caliceal punctures. The technique was successful in all cases and allowed access to the pelvicaliceal system, thus preventing early termination of the procedure. Access was through the upper pole calix or an interpolar calix in two cases each. In no case access was through the lower pole calix. In three cases, a rigid nephroscope was the only instrument used in conjunction with the ultrasound lithotripter. In one patient, complementary use of a flexible nephroscope was necessary to clear the stone burden completely.
Discussion
Fortunately, contrast extravasation that completely obscures the field is rare in percutaneous procedures. Precautions to avoid this phenomenon are gentle retrograde injection of contrast through the ureteral catheter, use of negative instead of positive contrast to delineate posterior calices, targeting caliceal stones directly with the needle whenever appropriate without injecting positive contrast, and most importantly, accurate puncture of the collecting system to avoid multiple failed attempts. Nevertheless, when this complication occurs, fluoroscopy-guided puncture is rendered difficult or impossible. Ultrasound-guided puncture is an alternative solution in these cases. However, an ultrasound machine must be readily available in the operating room, which is not always the case. Additionally, in cases of diffuse extravasation, caliceal dilation is significantly decreased or even completely lost, which makes percutaneous punctures difficult or impossible. Finally, even if the puncture is performed, subsequent dilation is unsafe because the anatomic landmarks of the collecting system are no longer fluoroscopically visible.
The technique we described herein has certain advantages. First, the angiographic catheter can be easily and rapidly inserted by simply exchanging it with the previously placed ureteral catheter over a guidewire. Second, despite contrast extravasation, the radiopaque tip can be seen fluoroscopically, which serves as the target for puncture. Third, the angiographic catheter itself can serve as a guide for the final dilation, indicating the calix (radiopaque tip) and the route from the calix toward the ureter.
The most crucial and difficult part of this salvage procedure is the correct placement of the catheter in a posterior calix. This is done by taking into account the anatomy of the collecting system as seen in the intravenous urogram or in a normal fluoroscopic image before extravasation. More importantly, the correct position is checked by rotational movements of the C-arm as described earlier. As a last resort, the catheter can be placed in the upper pole calix, and an upper pole puncture can be performed. Aiming at the tip of the catheter during needle insertion using the “bull's eye” technique is not very easy, but it is definitely feasible for experienced urologists performing their own access or for experienced interventional radiologists. One other question raised is whether the access offered by the punctured calix will be suitable for the stone to be treated. For pelvic stones, there should be no problem in the majority of the cases by simply using a rigid nephroscope. However, for more complex stones, one should be prepared to use a flexible nephroscope with a holmium laser to achieve stone-free status. The decision to proceed with this technique should be made by the surgeon on an individualized basis. In our hands, this technique has worked well as a salvage procedure and has saved us from the frustration of a completely failed surgery.
An alternative solution for significant contrast extravasation could be the use of a flexible ureteroscope to assist in percutaneous access. Ureteroscopically assisted percutaneous renal access was originally described by Grasso et al 2 as a salvage procedure in difficult cases. This technique was further evolved and even applied as a standard procedure with excellent results. 3 However, endoscopically assisted percutaneous renal access has not been described in cases of contrast extravasation. This technique seems applicable in such cases, although it requires an additional operator for the ureteroscope.
Conclusion
Herein, we described a salvage technique for fluoroscopy-guided percutaneous renal access in the case of diffuse contrast extravasation, which is based on the use of an angled-tip angiographic catheter. The catheter serves as a target for providing access to the renal collecting system and facilitates final tract dilatation, allowing completion of surgery in the same setting.
Footnotes
Disclosure Statement
No competing financial interests exist.