
Abstract
Objectives:
To determine and compare the status of urologic laparoscopic and robot-assisted surgery (RAS) across the world.
Methods:
Two hundred ninety-one surveys were completed by urologists at various national and international conferences in 2008. The 58-item questionnaire assessed the individual and institutional practice patterns of minimally invasive surgery with a focus on RAS. Surveys from Europe and North American continents (ENA) were compared with surveys from the Middle East and Asian continents (MEA).
Results:
One hundred sixty-six (57%) surveys were completed by urologists from MEA and 125 (43%) from ENA. Eighty percent of respondents performed minimally invasive surgery, with 64% having prior formal training. Respondents in ENA were more likely to have had formal training in RAS and performed more RAS cases (p < 0.01). Sixty percent of those surveyed from ENA had used robotic consoles in training courses compared with only 20% in MEA (p < 0.01). Dedicated RAS support teams were less common in MEA (p < 0.01). Lack of a robotic system was the most common deterrent for RAS in MEA (56%). Respondents in ENA performed more robot-assisted radical prostatectomy, robot-assisted radical cystectomy, and robot-assisted nephrectomy. In the more established robotic environment of ENA, robot-assisted radical prostatectomy, robot-assisted radical cystectomy, and robot-assisted nephrectomy represented the gold standard in 34%, 14%, and 26% of surveys, respectively. Comparatively, MEA respondents were more likely to believe RAS represented the gold standard.
Conclusions:
Usage of RAS in urology continues to grow across the globe, though to most it represents a surgical alternative rather than benchmark. Even with reduced exposure, training, and access, more urologists in the MEA considered RAS to be the surgical standard for prostatectomy, cystectomy, and nephrectomy. The evolution of attitudinal change should be the focus of further study.
Introduction
Established hindrances to adoption of MIS include adjusting to a learning curve, costs, and accessibility to technology. Access and acceptance of MIS, especially robot-assisted surgery (RAS), may vary according to geographic location. For some urologists, the surgical robot has aided their foray into the field of MIS by easing the steep learning curve. Current worldwide views of RAS have not been well documented. In this study we seek to analyze utilization, practice, and perception patterns among urologists specifically comparing the Eastern and Western Hemispheres.
Materials and Methods
A 58-item questionnaire was administered to general urologic meeting attendees at various national and international academic conferences held in the United States, Europe, and Asia in the fourth quarter of 2008. The questionnaire was made available to all meeting participants and completed by urologic staff, trainees, and other urologic health professionals if they chose to partake. The survey consisted of seven sections querying demographics, individual and institutional surgical practice patterns, and specific perceptions related to robotic surgery on the prostate, bladder, and kidney. Kidney operations included robot-assisted radical or partial nephrectomy and nephroureterectomy. Questionnaires were self-completed after a brief orientation by a research assistant, nurse, or physician assistant who explained the various sections of the survey. Ten minutes was the approximate time to complete the survey. All responses were kept anonymous.
The questionnaire was designed by an expert panel of robotic surgeons to assess current opinions and practice models. Formulation was based on panel discussion, literature review, and previous utilization surveys. All sections of the survey were further assessed for content and validity. Trends in Europe and the United States mirrored one another; thus, these two populations were combined (Europe and North American continents [ENA]). Similarly, trends in the Middle East and Asian continents (MEA) showed similarities and were pooled. Preliminary examination revealed a significant disparity in geographical access and perceptions; therefore, primary analysis was completed with ENA group data. MEA group data were compared to report observational differences.
Statistical analyses for categorical variables were performed using Fisher's exact test, while continuous variables were analyzed using the exact Wilcoxon nonparametric test. Values for continuous variables are given as mean (standard deviation), while values for categorical data are specified as n (column percent). Statistical analysis was performed using the Statistical Analysis System version 9.1.3 (SAS Institute, Inc., Cary, NC). A nominal significance level of 0.05 was used.
Results
A total of 302 surveys were collected with respondents from 3 continents and 43 countries. Eleven surveys were excluded because of incompletion of more than one section (4%). The remaining 291 responses were tabulated and compared. One hundred sixty-six (57%) of the respondents practiced in MEA and 125 (43%) from ENA. Table 1 lists respondent demographics. Of 291 participants, 153 (54%) were practicing urologists and 103 (36%) were in training. Respondents in MEA were more likely to be in practice (p < 0.01) and consequently tended to be older. The majority of respondents had practiced for >10 years, and there was no significant difference in practice time.
ENA = European and North American continents; MEA = Middle Eastern and Asian continents; MIS = minimally invasive surgery; RAS = robot-assisted surgery.
Minimally invasive practice
Overall, ∼80% of respondents performed MIS with 64% having received some formal training in MIS. Formal training in laparoscopic surgery was similar in ENA and MEA; however, formal training in RAS was much more prevalent in ENA (40% vs. 11%, p < 0.01; Table 1). Also, significantly more surgeons had sat on a training surgical console in the ENA group than in the MEA group (60% vs. 20%, p < 0.01). ENA surgeons performed significantly more operations robotically (p < 0.01, Fig. 1).
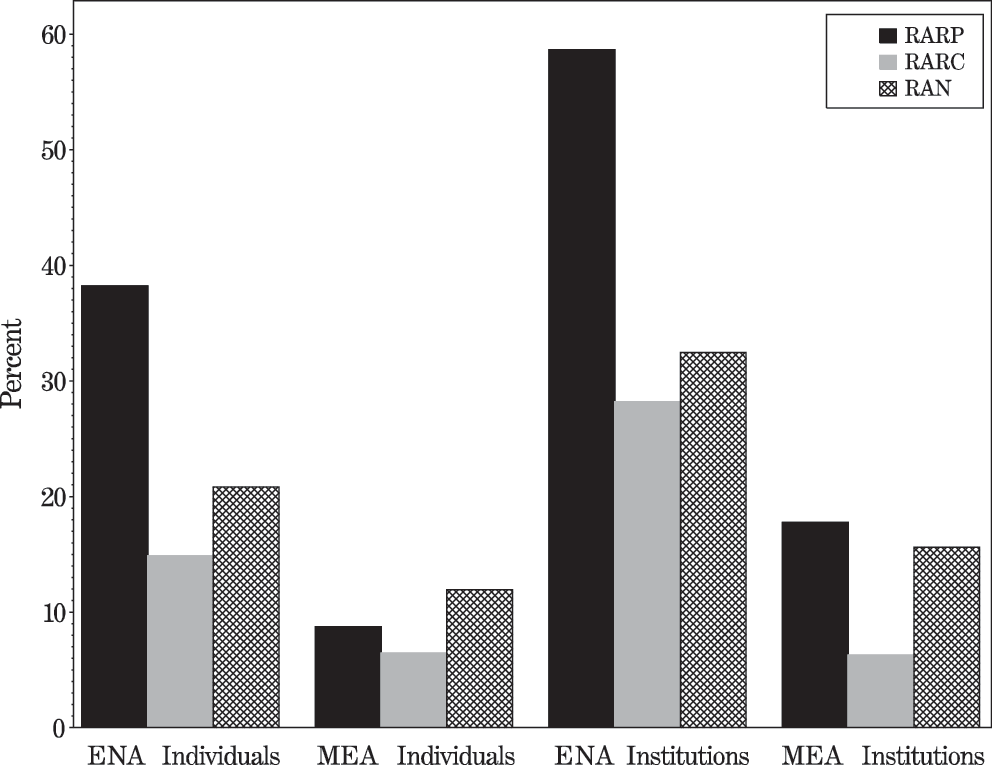
Usage of robot-assisted surgery. RARP = robot-assisted radical prostatectomy; RARC = robot-assisted radical cystectomy; RAN = robot-assisted nephrectomy; ENA = European and North American continents; MEA = Middle Eastern and Asian continents.
Although MIS was being performed in 86% of the respondents' institutions, there were significant differences between continents. Institutions in ENA were more likely to have multiple staff surgeons who performed laparoscopic surgery than MEA (87% vs. 76%, p = 0.02). There was a trend toward increased institutional availability of MIS fellowships in ENA (61% vs. 49%). In MEA institutions, MIS was primarily used to perform endourologic surgery (77%), while ENA institutions performed MIS for both endourology and oncology. More than 75% of respondents believed that RAS training could be either beneficial or required for their careers. A higher proportion of respondents in MEA (92% vs. 73%, p < 0.01) would consider an RAS fellowship if provided that opportunity. Additionally, MEA respondents were more likely to believe that MIS fellowships (p < 0.01) were needed for them to perform RAS and less likely to believe that proctorship was sufficient (p < 0.01).
A majority of overall respondents (>80%) believed that an RAS program would strengthen their departments academically and/or financially. Dedicated RAS support teams in the operating room were far less frequent in MEA than in ENA (28% vs. 54%, p < 0.01).
Reported barriers to establishing a dedicated RAS program varied according to geographic region. Respondents in ENA primarily noted a lack of administrative support (40%), whereas MEA respondents found a lack of an institutional robotic system to be the largest hurdle (56%). Together, these two hindrances made up the vast majority of barriers in both comparison groups.
Robot-assisted radical prostatectomy
Urologists surveyed in ENA were more likely to have performed robot-assisted radical prostatectomy (RARP) than MEA urologists (38% vs. 9%, p < 0.01) (Table 2). This difference was also seen on an institutional basis (59% vs. 18%, p < 0.01). The number of RARPs performed per year was significantly higher in ENA than in MEA (p = 0.03). Open radical prostatectomy (ORP) was still performed at most centers, though many had witnessed a decrease in case volume. Laparoscopic radical prostatectomy (LRP) was performed in a minority of centers, with no significant differences between comparison groups (23% vs. 32%, p = 0.55).
LN = laparoscopic nephrectomy; LRC = laparoscopic radical cystectomy; LRP = laparoscopic radical prostatectomy; ON = open nephrectomy; ORC = open radical cystectomy; ORP = open radical prostatectomy; QOL = quality of life; RAN = robot-assisted nephrectomy; RARC = robot-assisted radical cystectomy; RARP = robot-assisted radical prostatectomy.
Thirty-four percent of respondents in ENA declared RARP to be the gold standard for prostatectomy. Over 20% of respondents believed it too early to form judgments regarding RARP. Even taking into account the differential access and training noted previously, 46% of respondents in MEA believed RARP to be the gold standard. A higher proportion of MEA respondents (83% vs. 72%) would recommend RARP over ORP or LRP for themselves or their family though this did not reach statistical significance (p = 0.12).
Robot-assisted radical cystectomy
Urologists surveyed in ENA were also more likely to have performed robot-assisted radical cystectomy (RARC) as individuals (15% vs. 6%, p = 0.03) as well as in their institutions (28% vs. 6%, p < 0.01). Stratification by case volume showed no differences, as all institutions had low numbers of RARC completed (<100). Respondents in MEA were much more likely to have performed laparoscopic radical cystectomy (LRC) before embarking on RARC (56% vs. 10%, p = 0.01). Seventy-five percent of those surveyed believed that a robotic surgical system would assist with an extended pelvic lymph node dissection. There were differences in perceived advantages of RARC (p < 0.01) with more respondents in ENA citing a quality of life advantage (49%) compared with more MEA respondents believing RARC to be easier to perform (40%).
Regarding the status of RARC, many respondents believed it too early to make conclusive judgments (35%). Fourteen percent of respondents in ENA believed RARC to be the gold standard for cystectomy. As with prostatectomy, MEA respondents were more likely to believe RARC to be the gold standard (34%) (p < 0.01). A higher proportion of MEA respondents (64%) would recommend RARC versus open radical cystectomy or LRC for themselves or their family members (p < 0.01).
Robot-assisted nephrectomy
Generally, few institutions surveyed were performing robot-assisted nephrectomy (RAN), though there was a higher proportion in ENA (32% vs. 16%, p < 0.01). Most surgeons transferred previous skills in open nephrectomy (ON) or laparoscopic nephrectomy (LN) surgery to the performance of RAN. There were again differences in perceived advantages of RAN (p = 0.03) with more respondents in ENA citing a quality of life advantage (41%) compared with more MEA respondents believing RAN to provide improved oncologic outcomes (30%). Seventy-one percent of all respondents believed that RAN would not prolong warm ischemia time, but 52% felt that the robotic arms would have difficulty reaching the bladder cuff in nephroureterectomy scenarios. The most commonly cited advantages of RAN over LN included benefits of 3D vision, endowrist action, and instrument mobility.
Regarding the status of RAN, 21% of respondents believed it too early to judge. Twenty-six percent of ENA respondents deemed RAN to be the gold standard for nephrectomy. As with the other operations surveyed, a higher proportion of MEA respondents supported RAN as the surgical gold standard (39%). For themselves or family, urologists in MEA were more likely to recommend RAN than ON or LN (p < 0.01). The majority of ENA respondents would recommend an MIS option, without any preference for LN or RAN.
Discussion
While much has been written about the use of MIS in operative advancement, there is a dearth of usage data from the practitioners. This study represents ongoing analysis from our robotic survey data warehouse. 2 This survey administered in different parts of the world allowed for a diversity of responders, and as such was designed to determine differential exposure and attitudes toward robotics. Operative practices and perceptions of RAS were dramatically different across continents. This represents differential market penetration and surgeon exposure and illustrates worldwide views on RAS. Survey respondents in ENA were much more likely to be currently performing RARP, RARC, and RAN, but surgeons in MEA actually held these surgeries in higher regard (Fig. 2).

Perceptions of robot-assisted surgery subtypes.
At the conclusion of 2008, 1111 units of the da Vinci surgical robot had been sold worldwide. The vast majority were distributed in the United States (825) and Europe (194) with only 92 (8%) sold in the rest of the world. 3 This emphasizes the supply gap in accessibility of robots in different countries. Similarly in this study, robotic surgical systems were much more prevalent in ENA. Nonetheless, many larger centers in Asia and the Middle East have acted as robotic surgery leaders and trendsetters. 1 Practice differences may also be affected by cultural perception of technology and MIS. Some markets where new technology has not fully matured may be more inclined to embrace it or be biased by the perceived possible advantages. Marketing may also have an effect on the overall awareness and opinion. It is possible that a more mature RAS market (ENA) has achieved more realistic expectations and perceptions. Therefore, additional longitudinal follow-up of the emerging market trends in MEA should yield interesting results.
RAS is constantly evolving and will increasingly affect the way surgery is conceived, perceived, and performed. The robotic evolution of surgical care has been tempered by increased costs, lack of institutional support and funding, a shortage of surgeons with specialized training, and a paucity of long-term analysis of outcomes. With any novel approach, a period for acquiring competence and proficiency, and later expertise, is required. Ever more important are financial and economic constraints that affect widespread dissemination of new technology. Shah and Haas 4 illustrated a lack of significant price reduction in robotic infrastructure in contrast to many other technological economies of scale.
Deficiencies in residency training for the purpose of preparing the workforce for MIS have been documented. Wang and Winfield 5 found that 85% of respondents believed that they were inadequately trained during residency. Duchene et al 6 found that 54% of institutions performed RAS; however, only 38% of residents felt that their laparoscopic experience was average or acceptable. The emergence of MIS education relies on operative exposure, learning visual cues, and repetition with help from virtual reality surgical simulation. 7 The emphasis on rigorous integration of an evidence-based virtual simulation curriculum into residency training will help bring about a paradigm shift in surgical education.
Other studies have previously examined practice patterns in MIS. A survey of urologists in the Midwest United States in 2003 found that approximately 50% were performing laparoscopic surgery. 5 Practitioners who were older or had been in practice longer performed fewer laparoscopic procedures. Respondents in this study believed that the main advantages of MIS were reduced morbidity and faster recovery. In recent gynecology–oncology literature, Mabrouk et al 8 determined that 91% of surgeons surveyed performed laparoscopic surgery and 27% performed RAS. Barriers to laparoscopic surgery were mostly lack of training, increased operative time, and a steep learning curve. Barriers to RAS were mainly a lack of an institutional robotic system.
Overall, a high percentage (∼80%) of responders in this study performed MIS, demonstrating adaptation to progress and a positive acceptance trend. Historically, younger surgeons and those with fewer years of practice performed more MIS. Presently, although MEA respondents were older and more likely to be in practice, they were more accepting of RAS as a surgical option. Surgeons in ENA were more likely to have formal training in RAS, but most respondents surveyed in MEA (92%) would seek an RAS fellowship if available to them. There was also a difference in training perception such that MEA respondents predominantly presumed that a fellowship was the best way to achieve competency, whereas ENA surgeons believed that they could derive sufficient skills from residency training, proctorships, sabbaticals, or self-teaching.
RARP remains the most commonly performed RAS in urology with increasing numbers performed each year. While 1500 RARPs were performed in the United States in 2000, that number increased to 8000 in 2004 and 50,000 in 2007. 9 A recent prospective comparative study showed improved urinary continence and erectile function with similar oncologic outcomes with RARP compared with radical retropubic prostatectomy. 10 A greater percentage of ENA urologists in this study performed RARP, which corresponds to robot availability. However, a higher proportion of urologists in MEA held that RARP was the surgical standard. More than 80% of MEA respondents had enough confidence with RARP to recommend it for themselves or their family members. Most surgeons performing RARP transferred skills from open surgery. Most facilities continued to perform ORP while most did not perform LRP. This trend away from LRP toward RARP will likely widen as the availability of robotic surgical systems increases.
RARC remains a somewhat controversial means of bladder extirpation and continued outcome variables are ever more being acquired and analyzed. Again, higher proportions of RARC were being performed in ENA, reflective of the differential access to a robotic system. No institutions polled at the time of this survey had completed >100 RARCs. Eighty percent of urologists in ENA were able to transfer skills from RARP to RARC, likely because of increased numbers of those proficient in RARP in this group. MEA respondents were more likely to have previously performed LRC, while more ENA surgeons transitioned from open to RARC. Nearly all respondents believed that performing up to 100 RARPs would be enough to improve the comfort level of performing RARC. As with RARP, MEA respondents were more confident in supporting RARC as the gold standard or as good as LRC, whereas more ENA respondents felt that it was too early to make that determination. Again MEA respondents were more comfortable recommending RARC for themselves or their families as compared with open or LRC. About half of respondents believed proximal lymph node dissection to be challenging through robotic means. We have not experienced significant difficulty with performing extended pelvic lymph node dissection up to the level of the aortic bifurcation using four-arm da Vinci surgical systems.
RAN is a more recent burgeoning domain of robotic urologic surgery. The main theoretical advantages of RAN over LN include robotic suturing, improved observation, endowrist flexibility, and improved technical ergonomics. Many urologists continue to perform renal MIS by means of hand-assisted laparoscopy (HAL). This alternative can make the transition to advanced laparoscopy more intuitive. However, HAL is not without its detriments. In a study by Gofrit et al, 11 HAL surgery contributed to hand wrist numbness in 45% of surgeons and 37% also had pain. RAN would potentially reduce much of this operator morbidity. Few institutions polled were performing RAN although ON and LN were commonly carried out. The learning curve for RAN has not been established, but nearly all those polled believed that performing up to 100 robot-assisted radical or partial nephrectomies would be sufficient. Greater than 70% of respondents in this study supported that RAN would not prolong warm ischemia time for partial nephrectomy, in agreement with the literature. 12 Similar to the previous RARP and RARC data, RAN was felt to represent the gold standard to more respondents in MEA.
Limitations of this study include survey and selection bias. Respondents may be more inclined to answer the survey if they were performing MIS or RAS or had more of an interest in novel techniques or operative options. Several responses were left blank on various surveys, but the vast majority of data were complete and thus the surveys were fully analyzed. Another possible hindrance of the survey was a lack of a translated version. To prevent confusion, personnel were available to explain the questionnaire and the survey was formulated for easy understanding and completion. Another limitation is that the results of this study may not be generalizable to the community urologist. Seventy-five percent of respondents felt RAS training to be either beneficial or required. This may not reflect the general consensus of the community. Academic urologists at organized meetings may exhibit more awareness of cutting-edge technology depending on institutional investments and bias.
Conclusions
RAS in urology is becoming increasingly prevalent. As a developing commodity, RAS represents the gold standard for a minority of urologists. There appears to be major difference in RAS availability, usage, and perception depending on the geographical place of practice. Although urologists in the MEA have endured limited formal robot-assisted training, performed fewer cases, and have less availability of robotic surgical systems, they view RAS more favorably.
Footnotes
Disclosure Statement
No competing financial interests exist.