
Abstract
Objective:
To present the initial clinical experience in children undergoing unilateral and bilateral laparoendoscopic single-site nephrectomy.
Patients and Methods:
We reviewed our experience with pediatric patients who had undergone single-port nephrectomy (SPN) at our institution since August of 2009. Access was obtained by using the Hassan technique to place a 2-cm SILS™ Port (Covidien Surgical Devices, Norwalk, CT), which contains a gas insufflation channel and three individual cannulas that can readily accommodate laparoscopic instruments up to 12 mm in diameter. Nephrectomy was performed using a standard set of laparoscopic instruments and a rigid 5 mm 30 degree laparoscope (Karl Storz, Tuttlingen, Germany) with an end-on light source. Patient demographics, operative details, and postoperative treatment parameters were collected and recorded.
Results:
SPN was successfully performed in three consecutive pediatric patients (one female and two male patients: aged 11, 10, and 13 years, respectively) without placement of additional trocars or conversion to open surgery. The operative time for the unilateral SPN was 188 minutes, whereas bilateral SPNs required 214 and 300 minutes, respectively. Estimated blood loss for the unilateral and bilateral SPNs was 25, 20, and 30 mL; whereas patients were discharged on postoperative days 1, 3, and 12, respectively. The prolonged hospital stay was secondary to fever and pseudomembranous colitis in a patient with dialysis who also required a blood transfusion.
Conclusions:
Laparoendoscopic single-site simple nephrectomy is a technically demanding yet feasible procedure in children. Further studies are necessary to define the indications, advantages, and limitations of this technique as compared with standard laparoscopy.
Introduction
The primary advantage of these techniques is the avoidance of large abdominal or flank incisions and their attendant morbidity. In addition, traditional laparoscopic surgery typically uses three or more ports for a given urologic procedure. Each additional port placement increases the potential morbidity from damage to internal organ structures and hemorrhage and decreases the cosmetic outcome. 1 –3 As a result of the perceived advantages of using a single port, a significant amount of interest has recently been given to advancing the technique of laparoendoscopic single-site surgery (LESS).
Recently, LESS has been successfully used for a number of procedures in pediatrics, including peritoneal dialysis catheter placement, varicocelectomy, and simple nephrectomy. 4 –6 Initially, this approach did not gain widespread acceptance due to the increased difficulty of surgical dissection through a single port, as compared with conventional multiport laparoscopy. With improvements in technology and refinement of surgical technique, however, urologists have been able to perform a number of procedures with an increasing degree of complexity. Herein, we describe our initial experience with single-port nephrectomy (SPN), and, to our knowledge, we report the first use of LESS for bilateral simple nephrectomy in pediatric urology.
Patients and Methods
We retrospectively reviewed our experience with pediatric patients who have undergone simple nephrectomy using the LESS technique. Three patients at our institution have undergone SPN since August of 2009. These patients included an 11-year-old girl who underwent unilateral simple nephrectomy for a nonfunctioning, massively hydronephrotic right kidney and 10- and 13-year-old boys who underwent bilateral simple nephrectomy for severe nephrotic syndrome and end-stage renal disease (ESRD).
Operative technique
Patients are catheterized and positioned in the standard manner for SPN as has been previously described by our group. 7 Briefly, patients are placed in a modified flank position, and a semilunar incision is made within the lateral aspect of the umbilicus. The umbilicus is then sharply elevated, and the fascia is incised and vertically extended in both directions for a total of 2 cm. The inferior flange of the SILS Port (Covidien Surgical Devices) is then compressed and passed through the opening into the peritoneal cavity. The unique properties of the foam allow it to be compressed and readily reexpand and conform to the peritoneal incision, allowing the port to maintain excellent pneumoperitoneum without the use of fascial sutures to hold it in place. The system contains gas insufflation access and three individual cannulas that can readily accommodate 5-mm instruments, with any of the three cannulas able to accommodate up to a 12-mm instrument, again due to the inherent elastomeric properties of the foam construction (Fig. 1). Moreover, this novel port accommodates a wide variety of laparoscopic instrument brands, allowing the surgeon the ability to use the laparoscopic instruments with which he or she is most comfortable.

SILS™ Port (Covidien Surgical Devices, Norwalk, CT).
Pneumoperitoneum of 15 mm Hg is achieved, and nephrectomy is carried out with the following standard laparoscopic instruments: rigid 5-mm 30 degree laparoscope (Karl Storz, Tuttlingen, Germany), atraumatic bowel grasper, laparoscopic scissors, hook electrocautery, suction-irrigator, clip-applier, and a laparoscopic vascular stapling device. Although some authors feel that articulating instruments are essential to successful completion of SPN, 8 we did not find it necessary to employ them in our series. Of course, the patient populations (pediatric vs. adult) and procedure type (simple vs. radical nephrectomy) were different and may have a significant influence on the specific instruments that are ultimately chosen to complete a given procedure.
In all three patients, the colon was sharply reflected with the laparoscopic scissors and the judicious use of bipolar electrocautery, identifying the lower pole of the kidney and the psoas muscle posteriorly. The plane was further developed until the ureter was identified, circumferentially dissected, and grasped for the purpose of traction. Dissection was then carried superiorly to the hilum where the renal artery and vein were circumferentially dissected. Vascular control was obtained with the use of either Hem-o-lok clips (Weck Closure Systems, Research Triangle Park, NC) or the Autosuture™ ENDO GIA™ stapler. Additional blunt and sharp dissection was undertaken until the kidney was completely mobilized and the ureter was divided. The kidney was then brought out through the 2-cm umbilical incision intact. We did not find that a laparoscopic retrieval bag was necessary in all cases, although we did use one to remove the renal unit in the 11-year-old child with a massively hydronephrotic kidney to aid in complete extraction. For bilateral cases, the patient is then repositioned in the contralateral flank-up position. The single port (SP) is then replaced through the umbilical incision, and the contralateral kidney is removed in a similar fashion. Finally, the SP is then reintroduced, and laparoscopy is performed to confirm good hemostasis; and no intraabdominal organ injury has occurred. The SP is then removed, the fascia is closed with a running absorbable suture, and the skin is reapproximated with a running subcuticular absorbable suture.
Results
One unilateral and two bilateral SPNs were successfully completed in three pediatric patients (aged 11, 10, and 13 years, respectively) without the placement of any additional trocars or conversion to an open procedure. The operative time for the unilateral SPN was 188 minutes, whereas the bilateral procedures required 214 and 300 minutes, respectively. Estimated blood loss for the unilateral and bilateral SPNs was 25, 20, and 30 mL, respectively. The patient who underwent a unilateral SPN was discharged on postoperative day 1, whereas the patients who underwent bilateral SPN were discharged on postoperative days 3 and 12, respectively. At a mean follow-up of 6 weeks (range = 4–8), all patients were functionally at baseline, and cosmesis was excellent (Fig. 2).

Healed single-port umbilical incision 2 weeks postoperatively.
In the unilateral and one of the bilateral SPNs, we transumbilically placed our SP in the standard fashion. In the case of our second bilateral nephrectomy, we were able to utilize an existing left lower quadrant incision from the patient's prior peritoneal dialysis catheter placement. After removal of the peritoneal dialysis catheter, we extended the original 1.5-cm incision to the 2-cm necessary for SP placement. Incidentally, this was the only patient in which we had a complication for the series. Throughout his postoperative course, the patient had persistent fevers, developed significant diarrhea, and was ultimately found to have pseudomembranous colitis. This was not completely unexpected, however, as the patient had been receiving parenteral antibiotics for 2 weeks preoperatively due to a central venous catheter infection. On postoperative day number five, a workup for persistent fevers and anemia prompted an abdominal computed tomography scan that revealed a 9 × 5 cm retroperitoneal fluid collection in the left renal fossa, which may have been hematoma or irrigation fluid. The patient remained hemodynamically stable; however, due to symptomatic anemia, the patient required packed red blood cell transfusion. By this point, the patient had undergone three hemodialysis treatments, and the hematocrit had steadily declined since surgery. The serous, dark brown fluid collection was percutaneously drained, and both the gram stain and final cultures were negative.
The hilum was transected using a stapling device with one vascular load placed across both the renal artery and vein. After firing of the stapling device, we felt that hemostasis was adequate and moved to the contralateral side and performed nephrectomy in the same manner. As per our normal practice, after removing both renal units, we reintroduced the laparoscope through the SILS port and reinspected both renal fossae to assure excellent hemostasis had been achieved (which it had to the best of our knowledge). We feel that the anemia sustained had more to do with fluid balance issues than acute surgical blood loss and are, therefore, not entirely convinced that the drop in hematocrit was secondary to bleeding from the hilar staple line. Therefore, although we would acknowledge that the need for transfusion is rare after traditional laparoscopic nephrectomy, we would contend that the transfusion in this case had more to do with our patient population (ESRD requiring chronic hemodialysis) than the procedure itself and do not believe that LESS necessarily confers an increased risk of vascular injury due to decreased instrument maneuverability.
Discussion
Initial applications of laparoscopy in pediatric urology were diagnostic in nature, beginning with the report by Cortesi et al, 9 who used laparoscopic techniques to identify nonpalpable testes. This largely diagnostic role was continued until the early 1990s, when laparoscopy began to be used therapeutically. 10 Simple nephrectomy was actually the first major laparoscopic procedure performed in children. 11
Our patients ranged in age from 10 to 13 years, and although they are considered pediatric patients, it would be useful to know how to successfully apply these techniques in infants and toddlers. One of the first reported cases of SPN in pediatric urology was published in 2009. 12 The authors constructed a home-made single-port device using a surgical glove fashioned over an extra-small Alexis wound retractor. This was performed in a 3-year-old toddler. Although they were concerned about the limited abdominal workspace and adult-sized instruments, contrary to their expectation, they noted little difference between the pediatric and adult LESS after creation of adequate pneumoperitoneum (14 mm Hg in this case). Although LESS nephrectomy in infants has, to our knowledge, not yet been described, we would have similar concerns regarding limited working space and unsuitable instrumentation.However, with the ongoing efforts to develop more ergonomic instruments and achievement of adequate pneumoperitoneum, it may only be a matter of time until SPN is successfully performed in infants.
The traditional laparoscopic technique typically employs three or four ports ranging from 5 to 12 mm in size. Using the “triangulation rule,” the individual trocars are placed so as to maximize the intracorporeal working space to allow for proficient anatomic dissection while minimizing the clashing of instruments extracorporeally. This recurring issue is precisely what makes dissection through a single port more difficult than conventional multiport laparoscopy and is undoubtedly responsible for this technology not being adopted more broadly.
There are a few key points that we feel have been integral in allowing our team to successfully complete these procedures in a safe and timely manner. First, the standard laparoscopes that have been in use for decades have a large and somewhat cumbersome profile with a light cable that exits perpendicular to the telescope, which only adds to the problem of clashing extracorporeal instrumentation. This problem can be circumvented by using a lower profile camera which integrates the video element of the laparoscopic system with a coaxial light source that is in line with the shaft of the telescope. Second, as the instruments are passed through the fulcrum of the single port, the shafts are intentionally crossed, such that the extracorporeal right-handed instrument becomes the left-handed instrument intracorporeally and vice versa (Fig. 3). This move limits the amount of internal and external “sword fighting” that typically occurs when multiple instruments are introduced in parallel through a single port. It should be noted, however, that since this technique requires the surgeon to cross his or her hands, the anatomic dissection is often performed with the nondominant hand and necessitates ambidexterity and advanced three-dimensional spatial recognition by the surgeon. As such, there is a distinct learning curve involved with endeavoring to pursue LESS procedures of any kind. Certainly, with the advances made in surgical instrumentation (e.g., flexible laparoscopes, articulating and prebent instruments, magnetic anchoring and guidance systems), the learning curve for this technique will continue to be flattened and may even improve standard laparoscopy. 13
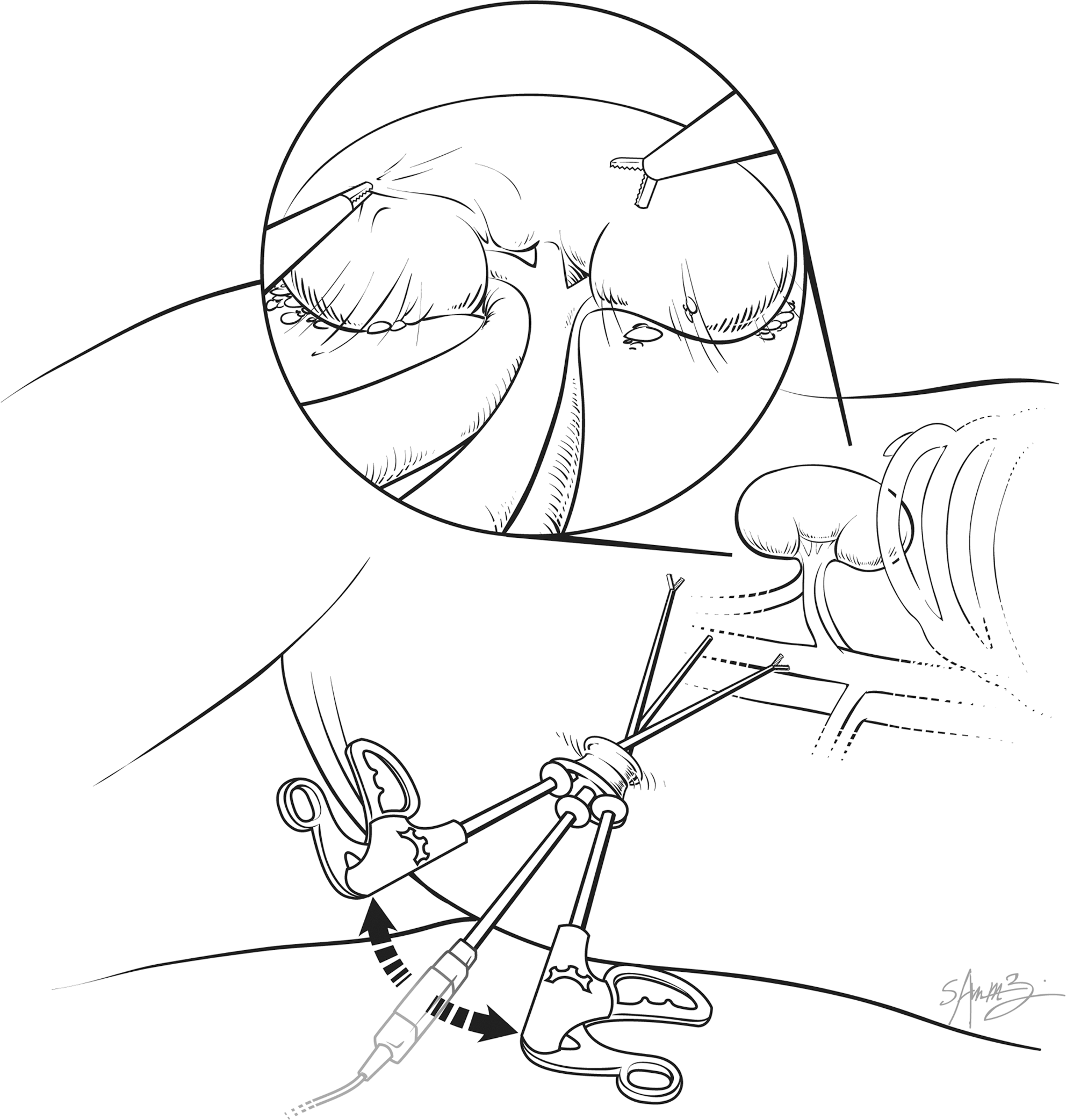
Laparoendoscopic single-site surgery using single-port device. The double-headed arrow denotes maximizing extracorporeal distance to minimize intracorporeal instrument clashing as the instruments cross the fulcrum. Note also the low profile camera with a coaxial end-on light source.
Although we did reposition the patients on their contralateral side to facilitate completion nephrectomy, certainly we feel that not having to place additional ports saved valuable operating room time and decreased the potential complications faced with each additional port placement. Although the only complication in our series was in one of the two children who underwent a bilateral nephrectomy, we do not believe that the bilateral nature of the procedure made it inherently more prone to operative complications and will continue to evaluate this parameter as we continue our pediatric LESS experience.
Another plausible option for laparoscopic bilateral nephrectomy has been previously described using three midline ports while making a separate Pfannenstiel incision to remove both enlarged renal units. 14 Although we would agree that this approach allows the surgeon to approach both sides while simultaneously obviating the need to place additional ports, the LESS approach has the added benefit of removal of both renal units through the same umbilical incision, thereby improving ultimate cosmesis.
Much of the pediatric laparoscopic extirpative work can now be performed using 3-mm ports or even percutaneously placed 2.3-mm instruments and one 3-mm port for the camera (expanded to retrieve the specimen) as opposed to the 5- to 12-mm ports used in our series. Through the use of our single-port device (which would hold true for other single-port devices), any number of differently sized instruments can be used, which we feel to be advantageous as we are not limited to using only “needlescopic” sized instruments. Also, in our experience, we have found the optics of the 5-mm camera to be far superior to the 3-mm cameras.
Until we have prospective trials demonstrating improvements in clinical outcomes, the relative merits of SPN are debatable. In infants, it has been our experience that recovery from laparoscopic (and even open) procedures is equally rapid. As children age, however, we would argue that the difference in postoperative recovery becomes progressively more significant. Perhaps the most noteworthy benefit from LESS in our series was observed in patients who underwent a bilateral procedure. It is our contention that by being able to perform the entire procedure and remove both kidneys through a single 2-cm incision, we were able to significantly reduce the morbidity that would be associated with bilateral flank incisions or a midline abdominal incision large enough to adequately perform a bilateral nephrectomy in the standard open fashion. In addition, even traditional laparoscopy, which avoids these larger incisions, would require multiple ports to successfully perform a bilateral nephrectomy. SPN seems particularly attractive for patients undergoing bilateral extirpative procedures.
As the minimally-invasive experience has matured, so has the technological sophistication and expertise, such that the era of extirpative and even reconstructive pediatric laparoscopic surgery is now well underway. Although the theoretical benefits to patients are significant, the temptation to be overzealous should be tempered by the limitations of this promising technology. Expectations are everything, and excessive expectations too early in the natural development of this new technique will ultimately impede meaningful progress and halt this technology from reaching its true potential. To this end, although we have shown that this approach is technically feasible and has a number of potential advantages in the pediatric population, the ultimate benefit must be weighed in further larger studies.
Conclusions
We have shown that both unilateral and bilateral LESS simple nephrectomy is technically feasible in the pediatric population by those proficient in laparoscopic surgery. With continued improvement in access devices, optics, and instrumentation, this new laparoscopic surgery platform will continue its dissemination throughout the urological community.
The indications for SPN and other LESS procedures in the pediatric population remain to be more clearly defined. Proper patient selection is imperative to determine for which individuals this technique is most appropriate. We believe this laparoscopic format will be most applicable when approaching urologic conditions that are bilateral in nature and when specimen extraction is necessary. Future directions include performing prospective clinical trials designed to evaluate the difference in clinical outcomes as compared with open and standard laparoscopy. It is only through this objective assessment that we can maximize clinical benefit while limiting the number of unnecessary complications and poor surgical outcomes.
Disclosure Statement
No competing financial interests exist.