
Abstract
Introduction:
Although radiation exposure from CT and plain film imaging has been characterized, the radiation received by patients during modern-era fluoroscopy has not been well described. The purposes of this study were to measure absolute organ and tissue-specific radiation doses during ureteroscopy and to determine the influence of body mass index (BMI) and sex on these doses.
Materials and Methods:
Eight cadavers underwent a simulated left ureteroscopy. Using a modern C-arm with automatic exposure control settings, thermoluminescent dosimeters were exposed for a fluoroscopy time of 145 seconds (mean time of clinical ureteroscopies from 2006 to 2008). Total tissue exposures were compared by BMI and between sexes using the Wilcoxon signed ranks test and the Mann–Whitney test with p < 0.05 considered significant.
Results:
Among all cadavers, radiation doses were significantly lower in all contralateral organs excluding the gonad (p < 0.012). Doses were similar bilaterally in the gonad in cadavers with BMI <30, and in all organs in cadavers with BMI >30 (p > 0.05). There were significantly higher mean bilateral gonadal doses in female cadavers (3.4 mGy left and 1.9 mGy right) compared with male cadavers (0.36 mGy left and 0.39 mGy right). The highest cancer risk increase was seen at the posterior skin equivalent to 104 additional cancers per 100,000 patients.
Conclusion:
Contralateral doses were lower for all organs except the gonad when the BMI was <30. In contrast, when the BMI was >30, there was no difference in radiation dose delivered to the ipsilateral and contralateral organs. Gonadal doses were significantly higher in female cadavers. Modern-era fluoroscopy remains a significant source of radiation exposure and steps should be taken to minimize exposure during ureteroscopy.
Introduction
Although the organ and tissue radiation doses for CT and plain film imaging have been characterized, 3 –6 the tissue radiation doses received by the patient during fluoroscopy in the modern era are not well described. The existing descriptions of radiation doses during fluoroscopy were not performed on modern equipment, 7 focused primarily on the exposure received by the operating room staff, 1 or in the case of patient dose, measured skin exposure only. 7,8 Modern equipment has features such as digital image capture, last image hold, and foot control, which reduce patient radiation exposure time. 9 In addition, modern fluoroscopy provides equivalent or improved imaging at lower exposure because of the image intensifiers and television images utilized in digital fluoroscopic equipment. 10 For most non-CT imaging, it has been shown that radiation exposures have decreased by 25% to 60%. 4
The purpose of this study was to determine organ and tissue-specific radiation dose received during ureteroscopy utilizing modern fluoroscopic equipment. This study also determined the effects of body mass index (BMI) and sex on organ dose. The mean dosage for each organ system is described and compared with published limits and other commonly used radiological imaging modalities. In addition, an increased risk of malignancy was estimated based on the mean radiation dose for each organ system.
Materials and Methods
Following approval of the protocol by the Department of Anatomic Pathology, and in accordance with the institutional policies for use of anatomic specimens, eight human cadavers were obtained, four male and four female. All cadavers underwent fluoroscopy consistent with a simulated left ureteroscopy for treatment of a ureteral stone. The mean fluoroscopy time of 145 seconds (range, 0.1–14 minutes) was calculated from all ureteroscopy cases performed at a single academic center between 2006 and 2008. A fluoroscopy time of 145 seconds was an average derived from the individual logged fluoroscopy times from the C-arm equipment for cases performed between 2006 through 2008. Patients with additional procedures such as percutaneous nephrostolithotomy were excluded from the calculation of the mean fluoroscopy time. To simulate a clinical ureteroscopy, the fluoroscopy time of 145 seconds was divided arbitrarily so that 40% (58 seconds) was directed over the left kidney, 20% (29 seconds) over the ipsilateral ureter, and 40% (58 seconds) over the bladder.
Radiation dose can be determined directly or indirectly. In this study, dose was measured directly using a previously described technique. 11 Direct measurements using thermoluminescent dosimeters (TLDs; Harshaw TLD-100 chips; Thermo Fisher Scientific, Waltham, MA) were taken at different anatomic locations in or on the cadaver to determine organ/tissue dose at specific points within the cadaver. The point dose for each organ was then used to assume the dose received by an organ during ureteroscopy. Each TLD underwent a four-part calibration process. TLDs were (1) annealed in a PTW annealing oven (PTW-New York Corporation, New York, NY) for 6 hours at high temperature to remove any prior radiation exposure, (2) exposed to a known dose (0.052 cGy) with ∼35 keV X-rays, (3) stored for 24 hours, (4) read using a Harshaw 3500 TLD reader (Thermo Fisher Scientific) and assigned a calibration factor (an average calibration factor of 27.3 nC/cGy).
Fluoroscopy was performed using an OEC 9900 Elite General Electric C-arm (General Electric, Fairfield, CT) with automatic exposure control settings programmed into the C-arm by the manufacturer. The fluoroscopy tube was below the cadaver while the image intensifier was situated above the cadaver. Each cadaver was positioned on a Maquet split leg fluoroscopy table (Maquet, Wayne, NJ) in the lithotomy position, identical to that used for clinical ureteroscopy at our institution.
Doses were measured by placing each TLD in the cadavers at the following locations: left and right anterior renal hilum; anterior skin surface in line with the left renal hilum; posterior skin surface beneath the left renal hilum; left and right midureter; left and right gonad; left and right lung base; and left cornea. After fluoroscopic exposure, TLDs were read using a Harshaw 3500 TLD reader, in which charge is converted to dose received using the previously determined calibration factors (Fig. 1).
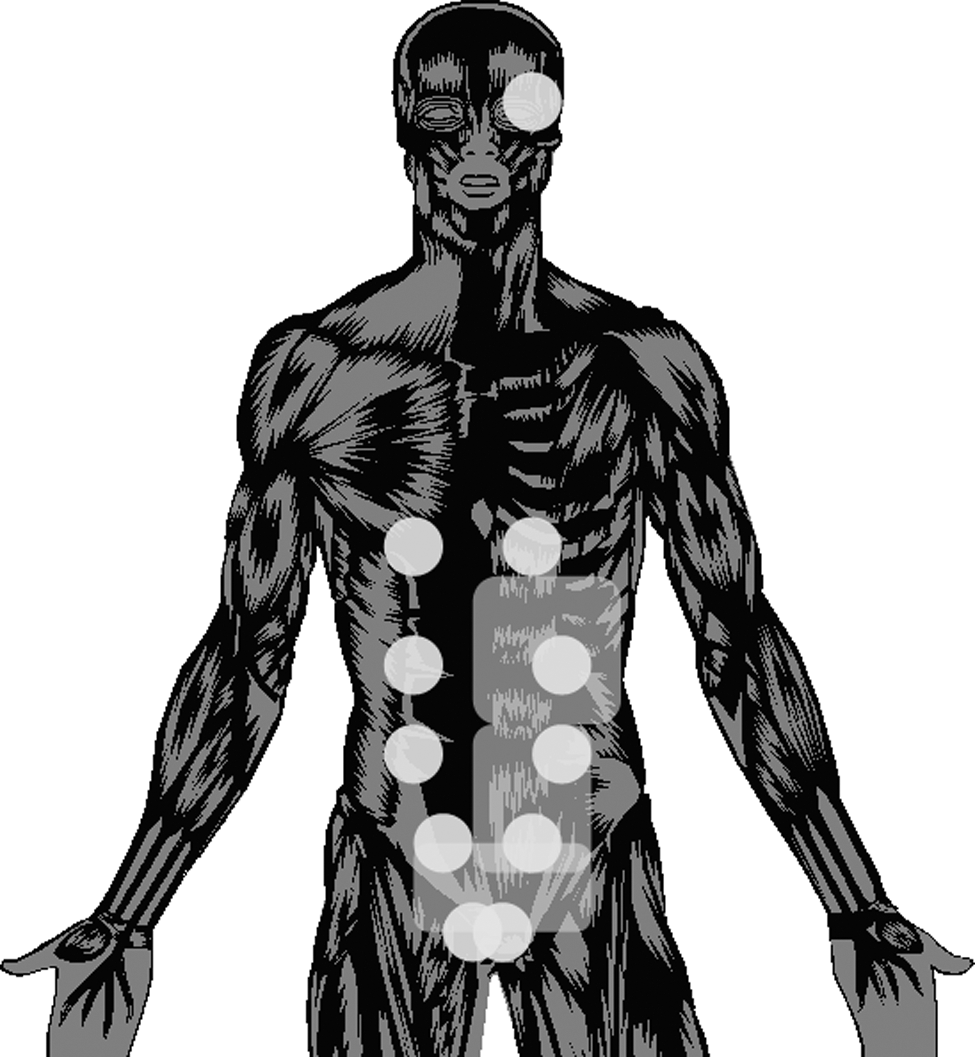
Cartoon depicting thermoluminescent dosimeter placement on cadaver (indicated by circles) and areas where fluoroscopy was concentrated to simulate left ureteroscopy (indicated by squared areas).
Tissue doses were compared by BMI and between sexes. Mean dose by organ system was calculated by average organ dose received per cadaver. Using data from the Biological Effects of Ionizing Radiation (BEIR) VII report and International Commission on Radiological Protection (ICRP) publication 103, cancer risks per 100,000 patients were calculated by organ. 12,13 Calculations were performed by multiplying the mean dose (point dose averaged over eight cadaveric measurements) measured at the organ by the given tissue risk factor in the ICRP report. When the location or organ system was not mentioned specifically in the ICRP report, a general risk model was used as outlined in the BEIR VII report.
Statistical analysis was performed with SPSS 17 (SPSS, Chicago, IL). Radiation dosages were compared using the Wilcoxon signed ranks test and the Mann–Whitney test. A p-value of <0.05 was considered significant.
Results
The mean dose for each organ was recorded and stratified based on sex (Table 1). Sex appeared to have a minimal effect on any organ dose except the gonad (Table 1). The ipsilateral (left) female gonad received an average of 3.4 mGy compared with 0.36 mGy for the ipsilateral (left) male gonad (p = 0.021). The contralateral (right) female gonad received 1.9 mGy compared with 0.39 mGy for the male contralateral (right) gonad (p = 0.020).
Bold faced values indicate significant variables with a p ≤ 0.05.
mGy = milligray.
Organs were then compared for significant differences based on laterality and stratified by BMI. Although some organs in cadavers with a BMI of >30 received larger radiation exposures (particularly in the posterior skin), these differences were not statistically significant (Table 2). Overall, ipsilateral organ radiation dose was significantly higher compared with contralateral organ radiation dose except in the gonad (Table 3a). When stratifying for a BMI of <30, ipsilateral organs received a significantly higher radiation dose except for the gonad (Table 3b). For cadavers with a BMI of >30, ipsilateral and contralateral organs had similar doses for each organ.
BMI = body mass index.
Posterior skin.
Anterior skin.
Bold faced values indicate significant variables with a p ≤0.05.
Posterior skin.
Anterior skin.
Bold faced values indicate significant variables with a p ≤0.05.
To provide a familiar reference for comparison of radiation exposures, the mean sample posterior skin fluoroscopic dose (10.4 mGy) was converted into posterior-anterior (PA) chest X-ray (CXR) equivalents. Utilizing an entrance skin dose for a PA CXR of 0.14 mGy, 14 the posterior skin received a maximum exposure of 74 CXR equivalents.
Using ICRP and BEIR VII criteria, data regarding the increased cancer incidence were calculated (Table 4). The highest increase was seen at the posterior skin, with a 0.25% increased risk, equivalent to 104 additional cancers per 100,000 patients. Excluding the posterior skin, increased cancer rates ranged from 0.2 to 7.4 per 100,000 patients per organ system examined.
Discussion
Diagnostic radiology services are used in urologic surgery with little understanding of the amount of ionizing radiation delivered to the patient. Previous studies that have quantified the amount of radiation received during ureteroscopy and other fluoroscopic procedures have concentrated primarily on the exposure of the surgical staff. 1,7,8 Some of these studies did quantify patient dose, but only at the skin. 7,8 In contrast to previous studies, we directly measured radiation levels received by individual organs utilizing modern-era fluoroscopy equipment and determined how the factors of BMI and sex affect these doses.
The fluoroscopy time used in this study for simulated ureteroscopy, 145 seconds, fell within the range of 78 to 1668 seconds reported in the literature. 1,8,11,15,16 This level was calculated based upon the actual mean fluoroscopy time used during clinical ureteroscopy cases in our institution. In this study, all cadavers were imaged with automatic exposure control settings as a method of standardization across individuals with varying BMI. The maximum minute dosage of 4.3 mGy/min, calculated based on mean dosage received at the posterior skin, was lower than the literature range of 10 to 1000 mGy/min. 17 This highlights the reduction in radiation exposure provided by modern-era fluoroscopy equipment with improved image intensifiers and television images utilizing digital fluoroscopy.
The highest radiation dose measured at any single organ location was at the posterior skin over the left kidney. The mean dose in our study was 10.4 Gy, with a maximum dose of 16.4 mGy seen in one TLD. This mean point dose is equivalent to the radiation exposure of 74 CXRs at this site. Skin doses have been reported in several ways in the literature. Bagley and Cubler-Goodman 7 reported a maximum posterior costovertebral skin dose of 100 mGy over 3.5 minutes, which is nearly 10 times higher than values observed in this study. Mahesh and colleagues reported a typical skin dose as a function of time with patients receiving 30 mGy/min. This value is seven times higher than the 4.3 mGy/min maximum rate observed at the posterior skin in our study. 11 The FDA suggests a skin radiation threshold of 1000 mGy per exposure, whereas another source lists the threshold for deterministic damage at 2000 mGy. 11,17 The deterministic effects of radiation include a sunburned appearance of the skin (may be delayed for several weeks), skin erythema, ulcers, telengiectasias, and dermal atrophy. 11,17 Fortunately, our study shows that reaching the threshold for deterministic effects would require a mean exposure of 465 minutes, which is far above the levels used for routine ureteroscopy.
In contrast to the deterministic effects of radiation, the stochastic effects, those that initiate cancer, do not have a threshold. The stochastic effect may occur at any level of radiation. Once cancer has been induced the outcome is the same regardless of the exposure dose. 11 Although some believe that a threshold exists at which no mutation will take place, many experts including the NCRP subscribe to the linear “nonthreshold” model. 13 Cancer risk estimates were calculated based on the BEIR VII and the ICRP 103 reports. The ICRP 103 report presented risk estimates by organ system. 12 Using this model, the largest theoretical increase in cancer risk in our study was observed at the posterior skin, with 105 additional skin cancers induced per 100,000 patients (Table 4). From the linear “nonthreshold” model estimates, ∼1;1 of every 1000 patients would develop a malignancy at the posterior skin caused by a single ureteroscopy. These models estimate cancer risk in an adult population; children are even more vulnerable to the effects of radiation. They have been shown to develop cancer at four to five times the adult rate for a given radiation dose. 9
The amount of radiation needed to capture an acceptable fluoroscopic image has traditionally been considered higher for individuals with an increased BMI. Taylor and Selzman 18 found that during defibrillator implants, obesity was a risk factor for increased radiation exposure. Arbique and colleagues 19 found an exponential relationship between BMI and dosage measured at the skin. Similar to previous studies, the radiation doses in cadavers with a BMI of >30 was increased at the skin. In contrast to these prior studies, this difference was not statistically significant. This may be partially attributed to the small number of cadavers with a BMI of >30 (n = 3). In addition to the skin dose comparison, our organ-specific model allowed the dose at the internal organs to be evaluated with relation to increased BMI. The trend of higher mean dose in the cadavers with a BMI of >30 was also seen at the left kidney, but significance was not reached (p = 0.297). Despite a nonsignificant radiation increase in ipsilateral organs among the higher BMI subjects, contralateral organs did not receive higher radiation doses (Table 2). Although increasing amounts of adipose tissue require higher levels of radiation for adequate ipsilateral tissue penetrance, this tissue may have reduced the radiation dose received by contralateral organs.
Gonadal doses were significantly higher for female than male cadavers (p = 0.02). This finding is not unexpected given the anatomic location of the female gonads (Table 1). Although gonadal dosages are not as large in comparison to the skin dosage, it has the potential to induce germline mutations. 20 When assessing the risks associated with radiation of the female gonad, age of the patient plays a vital role. Older women are at less risk for passing on genetic mutations and for tumorigenesis. 20 It is important that efforts be focused upon reduction of ovarian exposure, particularly in the young female population.
One limitation of this study is the use of fixed cadavers, which may image differently and require a different amount of radiation than a live patient. However, using a cadaver model allowed the direct measurement of organ and tissue radiation levels in a manner that is not possible in a live subject. Although the fluoroscopic imaging properties of fixed tissue are not well known, fixed tissue does appear to image similar to fresh tissue when using CT. 21 Another potential limitation was the small sample size (n = 3) for patients with a BMI over 30. There was a limited availability of obese cadavers at the time of the study. In addition, the cadavers are subjected to desiccation, which may decrease the BMI.
Another limitation lies within the fluoroscopy machine itself. The machine was used in a continuous fluoroscopy mode versus intermittent, which could change the radiation dose compared with intermittent mode levels. Further studies are needed to evaluate the actual radiation dose difference between intermittent versus continuous fluoroscopy modes in ureteroscopic cases.
An additional limitation is the assumption of whole-organ dose from a single TLD. Although this approximation may be close to the effective organ dose of a small organ, a single TLD dose may not be an accurate approximation for a summation of total organ radiation received during fluoroscopic exposure in larger organs. Given this limitation though, the primary objective in this study is to quantify organ dose by using modern-day fluoroscopic equipment. We believe this was achieved through publishing radiation point doses for organs during simple ureteroscopy. As point doses were measured in this study, we present the published skin entrance dose of a PA CXR and compare that with the measured posterior skin dose during fluoroscopy as an equivalent measurement of radiation. An effective dose was not calculated. This skin dose of a CXR was compared with the skin dose during ureteroscopy to provide a simple reference for comparison.
In this study, the cadavers were not connected to a ventilator because of the fixed nature of their tissues. Patients during surgery have respiratory excursion, which may broaden the radiation exposure. However, this is unlikely to affect the dosages as movement of the kidney is small (2 cm) and the fluoroscopic field is large. Lastly, there is likely some variability in the breakdown of exposure time over various body regions during ureteroscopy, and organ exposures would be affected by the location of the beam. Every ureteroscopy will produce differing exposures in different areas. These arbitrary levels were chosen to allow standardization between cadavers of different sex and BMI.
Despite these limitations, this study presents the most comprehensive determination of organ and tissue doses during ureteroscopy by using modern-era equipment. Use of a cadaver model allowed direct measurements at selected organs and at the skin to determine the actual radiation levels delivered rather than relying upon estimates or calculations. This study also allowed comparison of radiation doses between cadavers with different sex and BMI. This information can be extrapolated to understand radiation exposure in all patients undergoing fluoroscopy.
Radiation exposure to both the patient and staff during fluoroscopic cases should be reduced. One method is to use modern-era equipment with protocols employing last image hold, a surgeon-directed foot control, and digital imaging. A second technique is to manually decrease the mAs or kVp setting on the machine when image quality can be sacrificed at the discretion of the surgeon. Often, for wire placement or ureteroscope positioning, high-quality images are not required and a lower-quality image will suffice. A third option is to shield specific organs and parts of the body that are outside the field of interest. Finally, concerted efforts should be made to reduce the amount of time that the fluoroscopy is activated during surgery. All of these options can be implemented to reduce the radiation exposure for both the patient and staff.
Conclusion
Contralateral organs received significantly less radiation as expected, except for the gonad and for subjects with a BMI of >30. Gonadal doses in female cadavers were significantly higher than that in male cadavers. Even with modern-era equipment, fluoroscopy delivers a significant amount of radiation and steps should be taken to minimize patient's radiation dose exposure.
Footnotes
Acknowledgment
Steven Rightnar (Radiobiology Research Department) assisted with the measurement and conversion of radiation dose in this study.
Disclosure Statement
No competing financial interests exist.