
Abstract
Purpose:
We evaluated the use of narrow-band imaging (NBI) cystoscopy for the detection of bladder cancer and analyzed its diagnostic efficacy in cases of carcinoma in situ (CIS) and in cases with known urine cytology results.
Patients and Methods:
A prospective controlled study of NBI was conducted in 104 consecutive patients with definite or suspected bladder cancer. Transurethral targeted biopsies were performed after white light imaging (WLI) and NBI cystoscopy, and the histologic outcomes were compared.
Results:
A total of 313 biopsies were taken, including 161 from sites identified as potentially abnormal by NBI and/or WLI cystoscopy, and 152 from apparently normal sites. The percentage of malignancies in the sites identified only by NBI was 55.7% (39/70 places). In 26.9% of patients (28/104), bladder tumors were detected only by NBI. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and likelihood ratio of a negative test (NLR) for the detection of bladder tumors using NBI in all patients were 92.7%, 70.9%, 63.4%, 94.7%, and 0.10, respectively. The sensitivity, specificity, PPV, NPV, and NLR for the detection of CIS using NBI were 89.7%, 74.5%, 78.8%, 87.2%, and 0.14, respectively. The sensitivity, specificity, PPV, NPV, and NLR for the detection of bladder tumors using NBI in patients with positive vs negative urine cytology were 85.4% vs 98.4%, 75.7% vs 66.3%, 61.2% vs 64.5%, 92.0% vs 98.5%, and 0.19 vs 0.02, respectively.
Conclusions:
NBI is a simple and effective method for identifying bladder tumors including CIS without the need for dyes because of its high sensitivity, high NPV, and low NLR.
Introduction
Several novel endoscopic imaging techniques have been developed for the detection of bladder tumors, and the efficacy of fluorescence cystoscopy using dyes, such as 5-aminolevulinic acid (ALA), 6,7 hexaminolevulinate 5-ALA (HAL), 7,8 or hypericin, 7,8 has been reported. These studies showed that significantly more tumor lesions could be detected by fluorescence cystoscopy using dyes than by conventional cystoscopy using white light imaging (WLI) cystoscopy. Fluorescence cystoscopy demonstrated a sensitivity of >90% and a specificity ranging from 40% to 90% for the detection of tumor lesions. 6 –9
The narrow-band imaging (NBI) technique, in which modified optical filters are used in the light source of a video endoscope system, narrows the bandwidth of the spectral transmittance. NBI enhances the differences in penetration depth between wavelengths, because light penetration depth within the tissue is highly dependent on the wavelength; the shorter the wavelength, the more superficial the penetration. Blue light therefore penetrates most superficially, while red light penetrates deepest. In the NBI system, the relative intensity of the blue and green light is increased while the intensities of red light are decreased to a minimum. This enhances contrast in images of capillaries in the surface layers of the mucosal membranes and the detailed patterns on the mucosal membranes, without the use of dyes. Recent reports have suggested that NBI cystoscopy is more effective than standard WLI cystoscopy for the detection of bladder tumors. 10,11
The aim of this study was to examine the relationship between morphology and malignancy in the sites that are identified by NBI and to investigate the efficacy of this technique for the detection of malignancies in patients with suspected bladder cancer, using a prospective controlled study design.
Patients and Methods
Patients and study design
From July 2007 to January 2009, 104 consecutive patients with definite or suspected bladder tumor were enrolled in a prospective multicenter controlled study. The exclusion criteria included evidence of active bladder infection or exposure to radiation therapy or intravesical bacille Calmette-Guérin instillation therapy. Characteristics of the patients are shown in Table 1. In the patients with definite or suspected bladder tumor on cystoscopy, the average number of lesions is 1.7, ranging from 1 to 7. The patients were entered into the study after giving informed consent. This study was approved by the Institutional Review Board of each hospital involved.
NE = not evaluated; BT = bladder tumor.
Endoscopy equipment
The NBI system was equipped with a red, green, blue (RGB) sequential illumination light source unit (VISERA Pro, Olympus, Tokyo, Japan) and a video processor (CV–240, Olympus, Tokyo, Japan). NBI can be performed by using a light source with an option filter of NBI (CV-180). The light source contained two sets of rotating RGB filters; a WLI set for white light endoscopy and an additional set for NBI. The band-pass ranges of the RGB colors in the RGB filters designated for NBI were 600 to 620 nm, 530 to 550 nm, and 400 to 430 nm, respectively. In addition, the band-pass ranges of the red components of white light were narrowed, and the relative intensity of the blue and green light was increased. Switching between WLI and NBI was achieved by pushing a button on the video processor or using a foot switch.
Endoscopic procedure and histologic assessment
A total of 104 consecutive patients with definite or suspected bladder tumors were enrolled at four hospitals and treated according to the protocol. Biopsies were performed under anesthesia after observation by WLI and NBI rigid cystoscopy under the senior surgeons who had the experience of more than 20 cases of NBI cystoscopy. Initial observations were performed using WLI, followed by NBI. Abnormal-looking areas detected using either method were mapped and captured on image. Biopsies of definite or suspected tumor lesions were then obtained for pathologic examination. All patients received at least one biopsy from normal looking mucosa. The biopsies, which sites were decided before the biopsy, were performed under observation by both NBI and WLI to take a tissue sample accurately. To reduce potential variables, the WLI and NBI procedures for each patient were performed sequentially by the same surgeon, and all pathologic specimens were evaluated by a central pathologist.
Results
A total of 313 biopsies were obtained, including biopsies from sites identified by NBI and/or WLI as apparently normal (152 sites) or abnormal (161 sites). Seventy of the 161 (43.5%) abnormal-looking sites were identified only by NBI, while 91 (56.5%) sites were identified by both NBI and WLI (Table 2). All sites identified by WLI were also detected by NBI. Many of the sites identified only by NBI appeared as enhanced red or dark brown lesions against pale white normal mucosa, as shown in Figure 1, while many cases identified by both NBI and WLI appeared as red or dark brown, or tangible lesions, such as papillary tumors. In the sites identified only by NBI, malignancies such as CIS (25 sites) or pTa stage tumors (13 sites) were identified as red, edematous, or enhanced lesions. Inflammation (5 sites) and normal tissue (24 sites) were also identified (Table 3). The percentages of malignancies in the sites that were identified only by NBI and those identified by both NBI and WLI were 55.7% (39/70 sites) and 69.2% (63/91 sites), respectively. In 28 of 104 (26.9%) patients, bladder tumors were identified only by NBI.
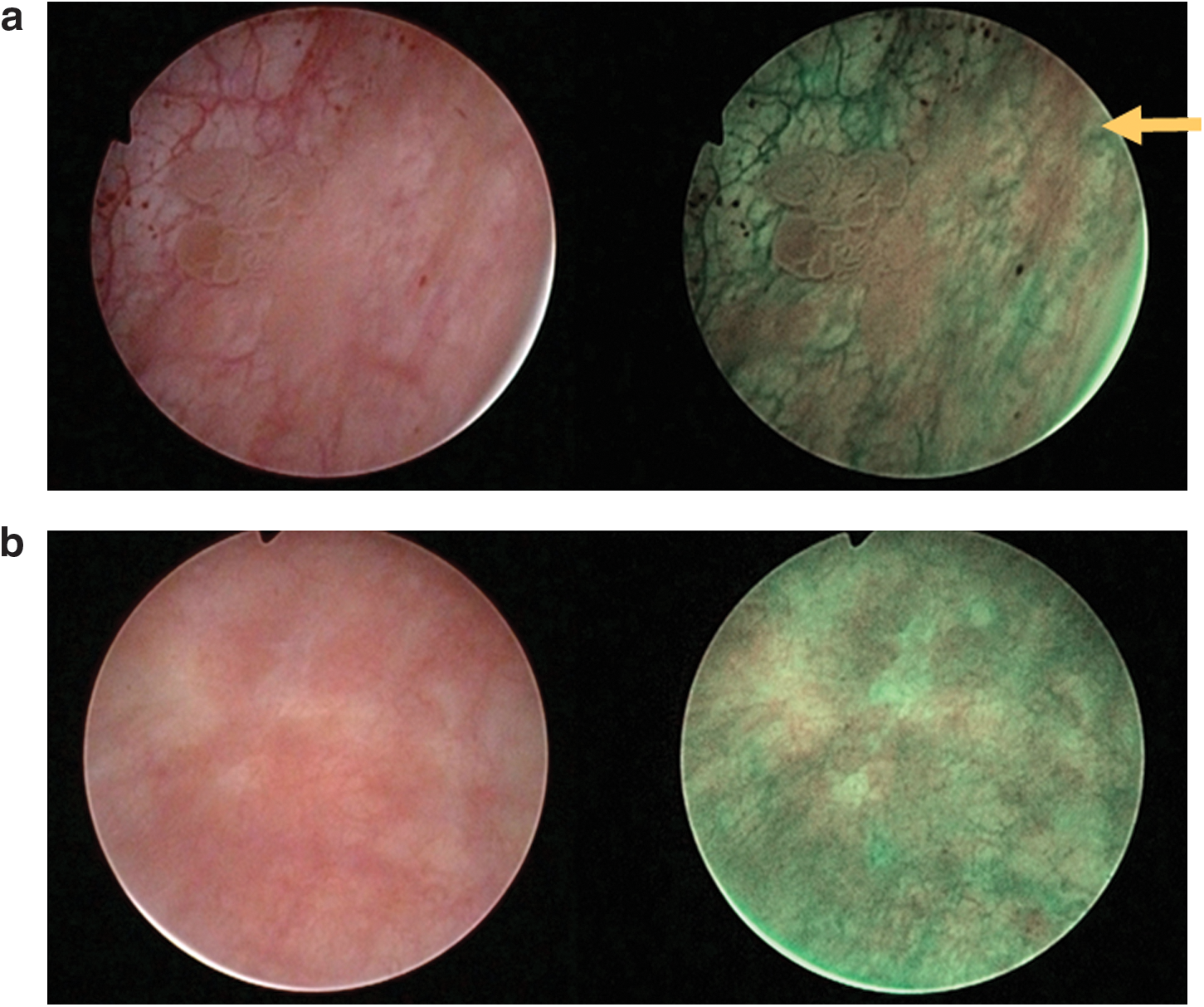
Examples of the differences between tumors visualized with white light imaging (WLI) (left) and narrow-band imaging (NBI) cystoscopy (right). (
NBI = narrow-band imaging; WLI = white light imaging.
NBI = narrow-band imaging; WLI = white light imaging.
The detection of bladder tumors using NBI and WLI cystoscopy is compared in Table 4.
P < 0.01.
NBI = narrow-band imaging; WLI = white light imaging; PPV = positive predictive value; NPV = negative predictive value; NLR = likelihood ratio of a negative test: specificity/(1-sensitivity).
The sensitivities for detecting bladder tumors in all 104 patients (313 biopsies) were 92.7% for NBI and 57.3% for WLI (P < 0.01), while the specificities were 70.9% and 86.2% (P < 0.01), positive predictive values (PPVs) were 63.4% and 69.2% (not significant), negative predictive values (NPVs) were 94.7% and 78.8% (P < 0.01), and the negative likelehood ratios (NLRs) were 0.10 and 0.50, respectively. There were more NBI-positive malignant lesions than WLI-positive malignant lesions (true positive; 102 vs 63). Conversely, there were fewer NBI-negative malignant lesions than WLI-negative malignant lesions (false negative; 8 vs 47).
The detection of CIS using NBI and WLI cystoscopy in 30 patients with CIS (113 biopsies) is shown in Table 5. The sensitivities for detecting tumors in patients with CIS were 89.7% for NBI and 50.0% for WLI (P < 0.01), while the specificities were 74.5% and 83.6% (not significant); PPVs were 78.8% and 76.3% (not significant); NPVs were 87.2% and 61.3% (P < 0.01); and the NLRs were 0.14 and 0.60, respectively. The true positive rate for NBI was higher than that for WLI (52 vs 29), and the false negative rate was lower for NBI than for WLI (6 vs 29). In 30 patients with CIS, 14 patients had CIS detected only by NBI.
P < 0.01.
As shown in Table 6, the sensitivity of NBI was 85.4% in patients with positive urine cytology (40 patients, 155 sites) and 98.4% in patients with negative urine cytology (63 patients, 157 sites). The specificities were 75.7% and 66.3%; PPVs were 61.2% and 64.5%; NPVs were 92.0% and 98.5%; and NLRs were 0.19 and 0.02, respectively. Of 63 patients with negative urine cytology, 8 had either CIS (7 patients) or T1 G3 high-grade tumor (1 patient) that were detected only by NBI.
Discussion
Since the development of the NBI system, several studies have demonstrated its ability to display enhanced images of the surface layers of various organ systems. 10 –15 In the field of urology, some reports have also indicated that NBI might be helpful in revealing suspicious areas in bladder tumors. 16 –19 We were able to confirm this by the generation of enhanced images of mucosal and vascular patterns in the bladder. A recent report showed that individual variation among urologists, including a novice, using NBI cystoscopy to evaluate patients for recurrent bladder cancer was minimal, and concluded that there does not appear to be a learning curve of NBI cystoscopy. 20
We performed a pilot study in 98 outpatients at four hospitals between November 2006 and January 2007, to determine if NBI was able to produce visually satisfactory results for the diagnosis of bladder tumors and to determine if there were any features that clinically interfered with cystoscopic examinations. These preliminary experiments failed to detect any significant problems that hindered cystoscopic diagnosis using NBI, except in the case of one patient who had bleeding and inflammation in the bladder. This preliminary investigation provided experience of NBI and helped to determine the design of the current prospective study. The visibility of cystoscopy using NBI is reduced in patients with bleeding or inflammation because enhanced images are generated by emission of light from target areas in two narrow wavebands that are strongly absorbed by hemoglobin. Our earlier experiences suggested that bleeding or active inflammation in the surface layers made it difficult to detect abnormal lesions. In these cases, NBI might not be a suitable auxiliary method to WLI, because WLI has better visibility than NBI.
It may not be appropriate to compare the efficacies of NBI and WLI based on the results of this study, because the results were not independently evaluated for each procedure. It is possible that the sensitivity of NBI could have been increased by previous WLI cystoscopy. Prospective randomized studies are needed to confirm the usefulness of NBI for the detection of bladder tumors.
The results of the current study, however, suggest that NBI can provide a useful complementary method to standard cystoscopy, with the ability to detect abnormal lesions missed by WLI. Furthermore, because NBI is a simple procedure that allows accurate detection without the need for agents such as 5-ALA or HAL, it is suitable for the detection of bladder tumors in outpatients.
The specificity of NBI demonstrated in this study was slightly lower than that of fluorescence or NBI cystoscopy reported in some previous studies. 7,8,18,21 As shown in Table 3, this reduction in specificity might have been because of the detection of inflammatory lesions by NBI. The specificity of the technique, however, increases as the number of NBI-negative normal tissues increases. It is necessary to evaluate not only the sensitivity and specificity, but also the predictive value and likelihood ratio. The sensitivity and NPV of NBI were >90% and the NLR was low, especially in combination with negative cytology (Table 6), indicating that it was an effective technique for identifying abnormal lesions, and useful for excluding a diagnosis of bladder tumor.
A definitive diagnosis of bladder cancer increases the chance of an effective therapeutic outcome. The diagnosis and treatment of CIS in particular is important for the control of tumor progression, because of the high potential of CIS for recurrence and infiltration of bladder muscle, and the increased risk of disease-specific mortality. 4,5 The results of our preliminary experiments suggested that the nonspecific identification of inflammatory change in patients with CIS led to a reduction in the specificity of NBI. Indeed, some red or enhanced lesions detected by NBI in the current study were inflammation pathologically, as shown in Table 3. The specificity of NBI for detecting bladder tumors, however, was high in patients with CIS (Table 5). The narrow waveband is unable to distinguish between a malignant cell and a normal cell but enhances the appearance of thick or inflamed mucosal layers. NBI can therefore detect increased thickness or inflammation of the urothelium associated with CIS. Furthermore, early recurrence of bladder tumors can result from incomplete resection of the tumor or growth of coexisting microscopic lesions not detected endoscopically during surgery. NBI provides better visualization of lesions by precise delineation of the surface layer, and may thus be useful when making decisions regarding the excision site of the tumor.
Conclusions
NBI is an effective method for the identification of abnormal lesions and can provide a useful auxiliary method to standard cystoscopy. It can be valuable for excluding a diagnosis of bladder tumors, including CIS, because of its high sensitivity, high NPV, and low NLR.
Footnotes
Acknowledgments
This work was supported in part by a grant from the Japanese Foundation for Research and Promotion of Endoscopy (JFE-2007).
Disclosure Statement
No competing financial interests exist.