
Abstract
Background and Purpose:
Percutaneous endoscopic management of bladder stones is not new. The ideal technique to establish suprapubic access, however, is still not justified. In this study, we used the 12-mm self-retaining laparoscopic trocar for access during management of large bladder stones.
Patients and Methods:
With the patient in the lithotomy position, a 12-mm self-retaining laparoscopic trocar was inserted in a full bladder under cystoscopic visual control. A 28F nephroscope was used to fragment the stone using ultrasound and pneumoclast lithotriptors. After stone treatment, the trocar was left in place, and transurethral resection of the prostate (TURP) was completed when indicated. Both urethral and suprapubic catheters were left at the end of the procedure. Clinical examination, urinalysis, and ultrasonographic examination were routinely performed during follow-up visits.
Results:
The mean stone size was 4.07 + 0.20 cm (2.8–6 cm). The average time for stone fragmentation was 32.78 + 2.16 minutes (range 8–53 min). A concomitant TURP was performed in 12 patients. The mean hospital stay was 2.56 + 0.15 days (range 1–4 days). All patients were stone free, and a total of six complications occurred, including extravasation, one patient; hematuria, two patients; and fever, three patients. All were treated conservatively. The mean follow-up time was 15.65 + 1.51 months (range 9–36 mos).
Conclusions:
Suprapubic percutaneous cystolithotripsy is a safe, minimally invasive alternative for management of large bladder stones. The use of a self-retaining trocar facilitates access and allows use of a large nephroscope for rapid fragmentation and extraction of the stone fragments. The presence of specific trocars for suprapubic access into the urinary bladder will encourage more transvesical end-laparoscopic procedures.
Introduction
PCL emerged in the last two decades to avoid urethral trauma and facilitate stone manipulation. There are different ways to establish suprapubic access. The most commonly used techniques are similar to those for percutaneous access to the kidney using both endoscopic and fluoroscopic facilities. 9 –11 In the present study, a new and simple one-step access to the bladder is reported using a self-retaining laparoscopic trocar under cystoscopic control. The technique is designed to facilitate and maintain suprapubic access during treatment of patients with large bladder stones.
Patients and Methods
During the last 5 years, the technique has been used to treat all patients who presented with large bladder calculi in our department. The inclusion criteria were bladder stone(s) burden of 3 cm or greater (measured by the larger diameter on plain radiography) and sizable stone bladder or posterior urethra (≥1 cm) in preadolescent children. The procedure was performed under regional or general anesthesia. A prophylactic perioperative antibiotic was administered to all patients.
With the patient in the lithotomy position, the procedure commences by transurethral panendoscopy using a small rigid cystoscope. The bladder is filled with normal saline. A suprapubic incision is made in the midline through the fascia and anterior wall of the bladder 3 to 4 cm above the symphysis pubis, and a 12-mm self-retaining laparoscopic trocar is inserted into the full bladder under cystoscopic monitoring (using the cystoscope light as a landmark). The self-retaining balloon is inflated with 20 mL saline, and the trocar is then locked to the anterior abdominal wall by sliding the stopcock on the outer surface of the trocar toward the abdominal wall (Fig. 1). The cystoscope is then removed and a suitably sized Foley catheter is left for continuous bladder drainage during the procedure.

Self-retaining laparoscopic trocar fixed to the anterior bladder wall.
A 28F nephroscope is then used via the trocar to fragment and remove the stone. Both Swiss pneumoclast and ultrasound lithotripter are used to fragment the stone. The stone forceps is used to remove fragments via the trocar. Also, flushing of the bladder with saline via the urethral catheter is performed to wash out the small residual stone fragments through the suprapubic trocar by transient disabling of its valve. The suprapubic trocar is left in place until the transurethral resection of the prostate (TURP) is completed. Otherwise, the procedure is ended by cystoscopic bladder examination, removal of the suprapubic trocar under vision, and placement of a suprapubic catheter on a guidewire, which is left in the bladder before removing the trocar. The cystostomy tube is usually removed 1 or 2 days postoperatively, followed by removal of the urethral catheter 1 day later.
All patients were seen 1 week after discharge for clinical assessment, including a routine examination by abdominal ultrasonography and plain urinary tract (PUT). Follow-up was continued every 6 months thereafter.
Results
A total of 23 suprapubic PCL procedures using a self-retaining laparoscopic trocar were performed. The average patient age was 58.22 ± 3.39 years (range 14–73 y). The study included two old children and two female patients. The stone size ranged from 2.8 cm to 6 cm, in the largest linear diameter on plain radiography, with an average size of 4.07 ± 0.209 cm. The stone was single in 16 patients and multiple in 7 patients. Distribution of the patients and procedures are shown in Table 1.
This group included four patients with benign prostatic hyperplasia (under α-blocker), two patients with atonic bladder (spinal cord injury), one patient with advanced prostate cancer, and two patients with unknown etiology.
One patient had visual internal urethrotomy and one patient had bladder neck incision using a hot knife.
TURP = transurethral resection of the prostate.
TURP was performed after stone treatment in 12 (52%) patients; all had preoperative significant obstructive lower urinary tract symptoms with or without a history of long-time use of an alpha α-blocker. The average prostate volume was 58.88 ± 2.93 g with a range from 40 g to 82 g. The other four patients with benign prostatic hyperplasia had mainly irritative symptoms and, as such, we elected to treat them medically with a selective α1-blocker after stone clearance. One patient underwent visual urethrotomy prior to the stone treatment and another patient had a transurethral incision of the obstructing (elevated) bladder neck after stone removal.
The ultrasound lithotripter was used alone for complete fragmentation of the stone in five patients. On the other hand, the Swiss LithoClast® was used in 7 patients and both lithotripters were used in 11 patients to achieve complete fragmentation of the stones. The average time for stone fragmentation and removal was 32.7 minutes (range 8–53 min). All patients were stone free at the end of the procedure (Figs. 2 and 3).

Preoperative plain radiograph of the abdomen and pelvis for a patient with large bladder stone and benign prostatic hyperplasia.
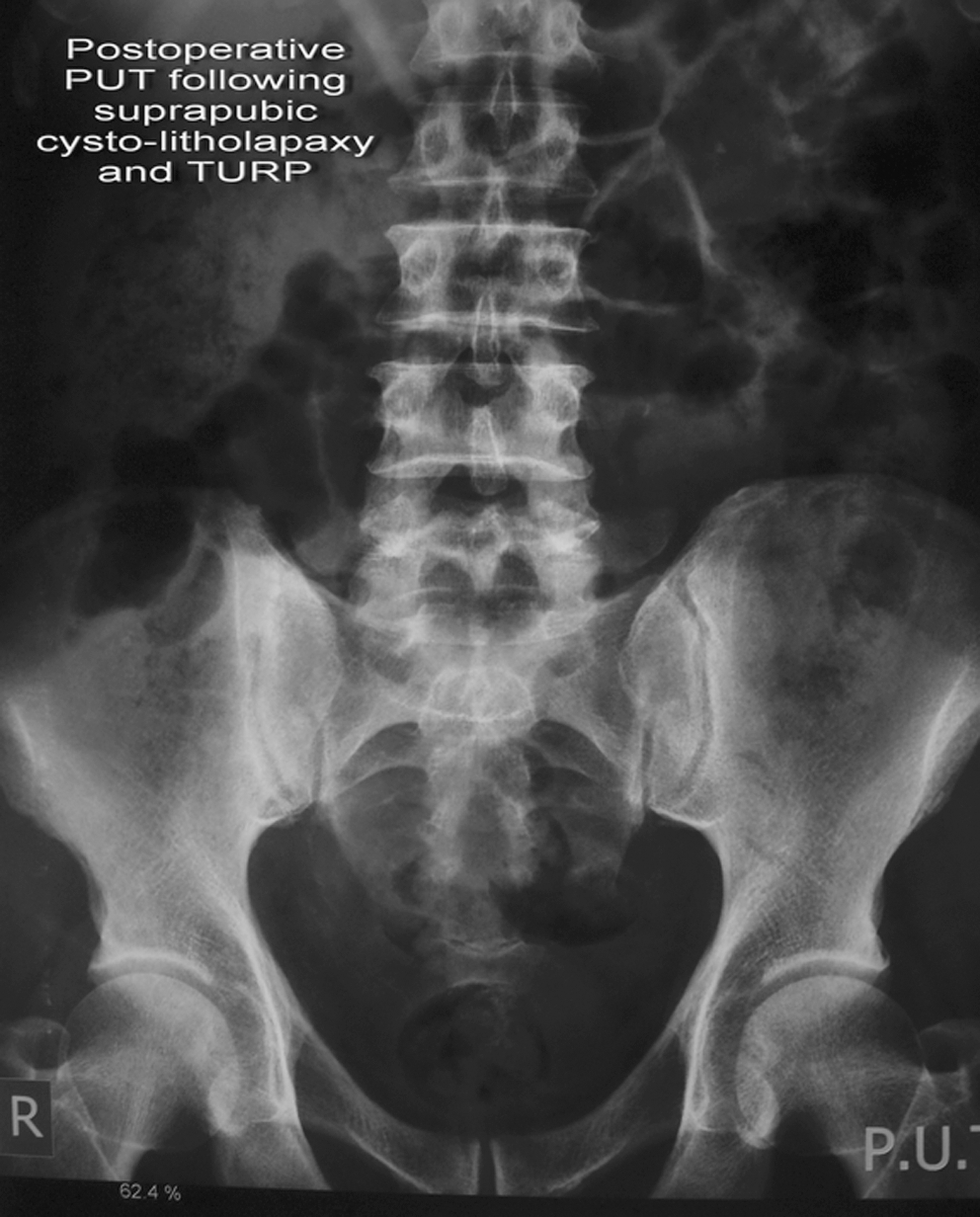
Postoperative plain radiograph for the same patient after percutaneous cystolithotripsy and transurethral resection of the prostate.
All procedures were successfully completed with a 100% stone-free rate and without intraoperative complications. The mean hospital stay for all patients was 2.56 ± 0.15 days (range 2–4 days). The suprapubic catheter was removed 24 hours postoperatively in 11 (48%) patients. In the other 12 (52%) patients with concomitant TURP, the suprapubic catheter was left for 48 hours postoperatively.
The average time for the urethral catheter was 2.8 days (range 2–7 d). In two (8.6%) patients, the urethral catheter had to be left for 4 days to control post-TURP hematuria. In another two (8.6%) patients, the urethral catheter was left for 1 week: One after visual internal urethrotomy and one with a moderate retropubic fluid collection that was diagnosed by ultrasonography during the first postoperative visit.
Postoperatively, a total of six complications occurred, including retropubic extravasation documented by abdominal ultrasonography (one patient), hematuria (two patients), and fever (three patients). All were treated conservatively, and bladder drainage was performed in three patients. All patients attend the first two visits (1 week and 1 month) and 19 (82.6%) patients were available for routine (3, 6, 12 months and annually) follow-up after the procedure. The mean follow-up time was 15.6 ± 1.51 months (range 9–36 mos) with no late complications related to the procedure.
Discussion
There are variable techniques for management of large bladder stones. In a recent publication, open cystolithotomy was found to be an effective combination with TURP and added no further complications. 12 While open cystolithotomy is considered safe and easy to be performed with or without concomitant TURP, it is still an invasive procedure.
In the last decades, many changes in the treatment modalities for bladder stones have occurred, including use of SWL as the least invasive method. SWL still has stone size limits together with other technical difficulties when used in the bladder. Endoscopic treatment of bladder stones is still the most common minimally invasive technique used by most urologists today. Also, new lithotripters are more preferred than mechanical stone fragmentation to avoid the associated bladder trauma (10% or more). 5,7,8
Two main challenges are considered during any transurethral procedure for bladder stone treatment including the long time necessary for stone fragmentation and the caliber of the urethra in children. As such, suprapubic percutaneous access to the bladder has emerged as an alternative to the transurethral technique. Different ways have been described to achieve suprapubic access. The most commonly used technique was suprapubic needle puncture and consequent dilatation until a 30F or 34F Amplatz renal dilator sheath is introduced into the bladder. The technique has been used with and without fluoroscopic assistance. 6 Laparoscopic technique and devices had been used to aid in retrieving stones from a neobladder and proved to be successful. 9 Elder 11 has described an interesting method by using an endotracheal tube to achieve suprapubic access and inflated the balloon to prevent its slippage out of the bladder during stone manipulation.
In the present study, we used the self-retaining laparoscopic trocar to gain a single-step, fast, and secure access to the bladder. The trocar has a 20 mL capacity balloon that was inflated inside the bladder after insertion and a stopcock on the outer sheath that tightens the device to both the anterior abdominal wall and bladder wall. By doing this, we think the chances for fluid to escape around the trocar will become very low. The technique was successfully used in 23 cases with various ages (two preadolescent children) with no intraoperative complications or conversion to open surgery because of failure or complicated access.
Different types of energy are used to fragment the stone bladder including Swiss pneumoclast, electrohydraulic, ultrasound lithotripter, and laser. 7,13 Pneumoclast lithotripsy is the most commonly used because it is cheap, widely available, and successful in fragmenting large stones. In this study, both pneumoclast and ultrasound lithotripters were used in combination to fragment stones and accelerate removal of the fragments. We prefer to start with the pneumoclast in cases with large and hard stones; ultrasound is used to fragment the moderate-sized stones.
The suprapubic PCL approach offers several advantages for management of large bladder stones with or without concomitant TURP. First, the use of a large caliber trocar allows the use of a large working endoscope, which facilitates fragmentation and subsequent washout/removal of large stone fragments. Also, the technique allows better control on the stone within the large cavity bladder during lithotripsy. In addition, by using this technique, the urethra will be saved from long-time manipulation with possible postoperative urethral complications. Urethral stricture is still a concern after long-time transurethral procedures. An 8% rate of urethral stricture has been reported after transurethral cytolithotripsy with concomitant TURP. 6 In this study, the authors spent an average of 40 minutes to fragment bladder stone in addition to the time needed to perform TURP. Using suprapubic percutaneous access would save the urethra for at least one-third of the total procedure time, and this would definitely decrease the risk of postoperative urethral stricture.
Extravasation of the irrigation fluid from around the access tube during suprapubic PCL is an important cause of technical failure. The time of extravasation may be intraoperative or early postoperative. The intraoperative extravasation could be a major reason to convert to open surgery, especially with intraperitoneal fluid collection. In a large series, Al-Marhoon and associates 14 had reported four (14.7%) cases of extravasation; three of them had needed exploration to drain intraperitoneal fluid collection after suprapubic percutaneous litholapaxy in children. Also, Aron and colleagues 15 had one case with postoperative extravasation after suprapubic percutaneous litholapaxy and TURP. 15 Both authors used a similar technique for bladder access. In this series, one patient had suprapubic small extravasation that was discovered during abdominal ultrasonographic examination 1 week after the procedure. The patient was treated conservatively with antibiotic and anti-inflammatory drugs with no need for intervention.
In our experience, the use of a self-retaining trocar together with keeping pressure low inside the bladder by having a suitably sized urethral catheter in place during the procedure are two important factors that will prevent intraoperative extravasation of the irrigation fluid during suprapubic PCL.
Comparative studies between transurethral and suprapubic percutaneous lithotripsy for management of bladder stones are few. 6,15 Tugcu and coworkers 6 compared percutaneous and transurethral procedures for stone fragmentation. The authors could fragment and clear larger stones in a shorter time using a suprapubic technique. In their study, three (8%) patients in the transurethral group needed another session to clear residual fragments that have been overlooked by bleeding from a fragile prostate. All patients in the percutaneous group were stone free. Similarly, we could achieve a 100% stone-free rate in a single treatment session using the suprapubic PCL approach.
Conclusions
Suprapubic PCL is a safe, minimally invasive technique for management of large bladder stones with a 100% stone-free rate. The technique saves urethral manipulation and decreases the possible risk of postoperative urethral stricture when concomitant endoscopic procedures are needed. The use of a self-retaining trocar facilitates and secures the access as well as enhances rapid extraction of large stone fragments through the 12-mm trocar. The presence of specific trocars for suprapubic access into the urinary bladder will encourage more transvesical endolaproscopic procedures for different intravesical pathologies.
Footnotes
Disclosure Statement
No competing financial interests exist.